
Abstract

To the Editor:
Tick-borne diseases are increasing in prevalence. Ticks are best removed as soon as possible, because the risk of disease transmission increases significantly after 24 hours of attachment. 1 Furthermore, signs and symptoms of tick paralysis improve within hours of tick removal, and complete recovery occurs within 24 hours. 2 Removing ticks may not be easy and it is very difficult to remove nymphs without damaging them. It is important to completely remove the tick, including the mouth part and the cement the tick has secreted to secure its attachment. 1 A small tick remnant in the skin is difficult to detect and localize, and attempts to remove these parts may result in significant skin trauma or a secondary skin infection. Improper tick removal may lead to infection or granuloma formation, which must always be surgically resected during a second procedure. An effective tick removal method must reduce the possibility of fluid regurgitation and transmission into the host during the procedure. Although there is conflicting evidence whether the removal technique influences infection rates, killing the tick in situ may increase the risk of regurgitation and transmission of infectious agents. Theoretically, touching the tick during the removal attempt may also irritate the tick and cause it to force more liquid into the wound. To prevent tick-borne disease, therefore, it is important to urgently remove the tick, to use the correct removal procedure, and to remove the whole tick, intact and alive, without any remnants. 1 It is preferable that a medical practitioner remove the tick as an office procedure and not in an outdoor condition, especially in areas where ticks are endemic.
Numerous techniques for tick removal have been reported, with limited experimental evidence, and many of them have proved unsatisfactory in daily medical practice, leading to tearing ticks apart, leaving parts embedded, and making the situation worse instead of better. Few of these techniques have scientific support, and some may even cause harm by inducing the tick to salivate and regurgitate into the host. 3 Unfortunately, there is no single appropriate and absolutely effective and safe tick removal technique—no technique will completely remove every tick, and no technique will remove every tick with the first attempt. The most commonly recommended and successful tick removal method has been manual extraction (with a continuous and steady action) of the tick using a blunt, medium-tipped angled forceps or fine point tweezers. 1 When we used this method, however, many times a mouthpart remnant broke off and remained in the skin. Moreover, excessive pressure (which is difficult to objectively measure) exerted with forceps can crush the tick's thorax and head—particularly for tiny species—and possibly force infectious body fluids through the tick's mouth parts into the wound. 4 Miyamoto and Hashimoto 5 recommended surgical tick removal if more than 24 hours have passed since the tick bite. Surgical removal should also be considered when the tick is smashed or crushed because of a previous failed removal attempt or when the tick is a small nymph, making complete removal difficult by any other means.
During the last 5 years, we have removed many ticks—attached to the neck, scrotum, armpit, extremities, or anywhere else on the body—using a minimally invasive surgical technique as described in Murtagh's General Practice. 6 After a subcutaneous injection of xylocaine around the bite point, we make a limited skin excision (epidermis and dermis 2 mm to 3 mm in diameter and depth) of the entire area, and remove en bloc the tick-skin junction along with the parasite in full (Figure). The surgical wound is closed by placing a single stitch of 6-0 nonabsorbable suture or by using sterile strips. We do not touch the tick during the procedure; that is important because it eliminates the possibility of regurgitation and transmission of infectious agents by the tick into the host. Patients who have topical skin erythema around the bite point receive amoxicillin by mouth for 7 days. The dermal wound stitch is removed on the fifth or sixth postoperative day. None of our patients (6 to 65 years old) has had any systemic or local wound complication after the tick removal.
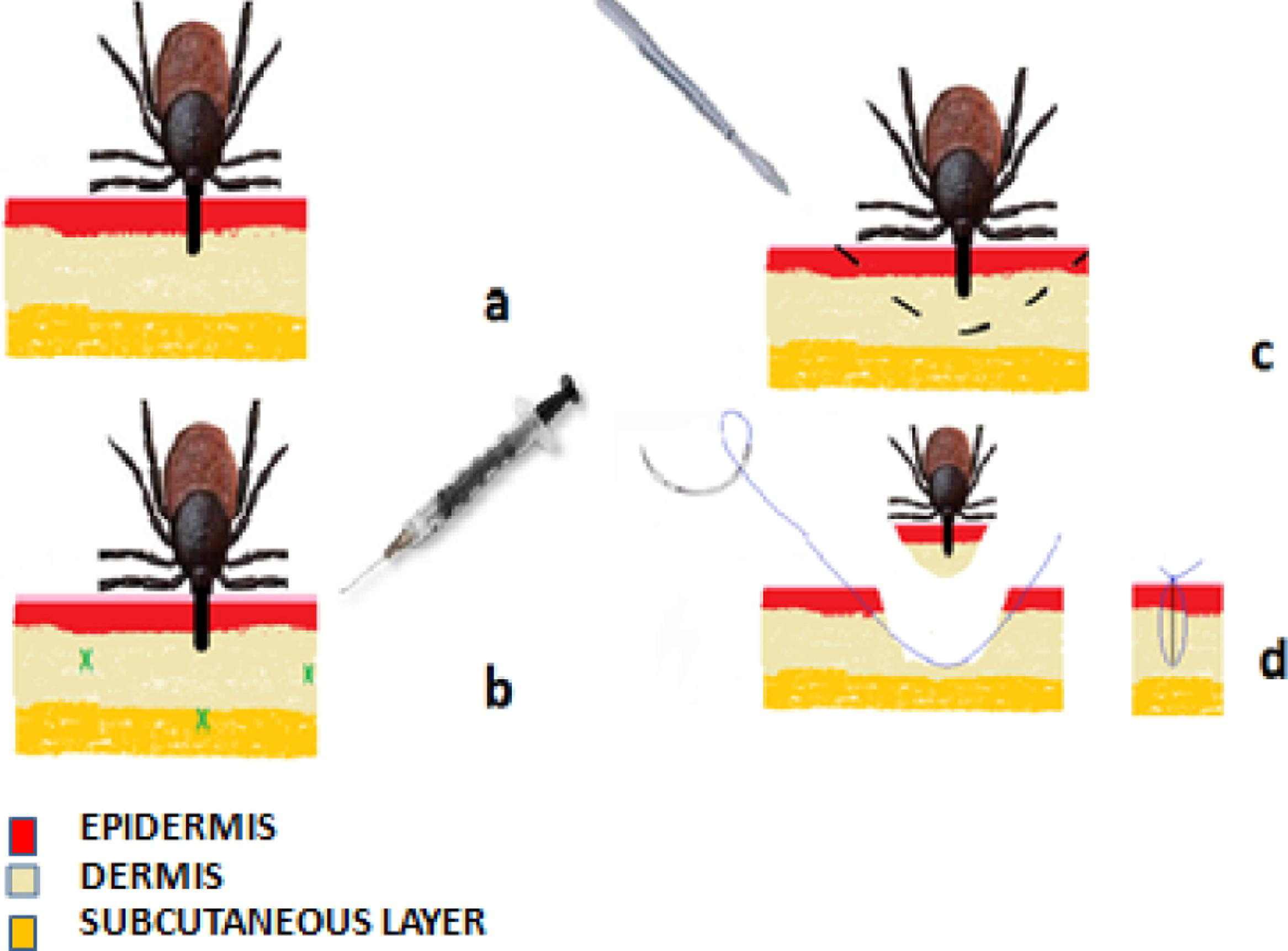
a, Tick attachment. b, Subcutaneous xylocaine injection. c, Limited skin excision (epidermis and dermis, diameter and depth = 2 mm to 3 mm) of the entire area around the bite. d, Complete tick removal (en bloc, the tick–skin junction with the parasite in full) and wound closure.
Some could argue that the average tick bite does not require surgical removal, and that this procedure can be reserved for complicated cases (eg, smashed tick), for a small nymph, and for tick bites more than 24 hours old. We believe that this method can be applied routinely in an organized medical room in areas where tick-borne diseases are endemic: it is painless, safe, and not time consuming; it is tolerated by cooperative school-aged children; and it can be easily performed by every healthcare practitioner. Compared with any other technique, it is the only one that excludes any tick contact or excitation that could provoke the tick's transmission of infectious agents into the host. Furthermore, this method secures complete removal of the mouthparts and ensures no tick remnant remains inside the skin. The only disadvantage of this method is that it is invasive—but only minimally. The only contraindication to this technique is a tick bite on a torulus or an eyelid.