
Abstract
Increasing evidence points to a role for circulating endothelial progenitors, including populations of CD34-positive (CD34+) cells present in peripheral blood, in vascular homeostasis and neovascularization. In this report, circulating CD34+ cells in individuals with a history of cerebral infarction were correlated with changes in neurologic function over a period of 1 year. Patients with decreased levels of CD34+ cells displayed significant worsening in neurologic function, evaluated by the Barthel Index and Clinical Dementia Rating. These results support the hypothesis that levels of circulating CD34+ cells have prognostic value for neural function, consistent with their potential role in maintaining cerebral circulation.
Introduction
Increasing evidence points to a role for circulating CD34-positive (CD34+) cells in maintaining vascular homeostasis, both as a pool of endothelial progenitor cells (EPCs) and as a source of multiple growth/angiogenesis factors (Majka et al, 2001). Previously, we have shown accelerated neovascularization after administration of CD34+ cells in an experimental model of stroke (Taguchi et al, 2004b), and observed a positive correlation between levels of circulating CD34+ cells and neovascularization (Yoshihara et al, 2008) and regional blood flow (Taguchi et al, 2004a) in patients with chronic cerebral ischemia. In addition, we have delineated a contribution of circulating CD34+ cells in support of neurologic function, presumably through their positive influence on the cerebral circulation in settings of ischemic stress (Taguchi et al, 2008). A role for circulating CD34+ cells in vascular homeostasis has also been considered in other ischemic settings, such as myocardial (Okada et al, 2008) and peripheral vascular disease (Fadini et al, 2006b).
On the basis of these observations, we have hypothesized that circulating CD34+ cells may contribute to the maintenance of neurologic function by enhancing cerebrovascular homeostasis in patients with a history of cerebral infarction. In this study, we have investigated the predictive value of the level of peripheral CD34+ cells on neurologic function in patients with past cerebral infarction. Our results display a correlation between decreased levels of CD34+ cells and diminished neurologic function over a study period of 1 year.
Methods
This study was approved by the institutional review board of the National Cardiovascular Center. All subjects provided written informed consent. A total of 40 individuals with history of cerebral infarction (3 years or more from the last onset of stroke) were enrolled and followed for 1 year. Exclusion criteria included the following: patients who experienced a vascular event within 30 days of enrollment, patients with neurodegenerative diseases including Alzheimer's-type cognitive impairment, history of cerebral hemorrhage, cerebral infarction not classified according major causes (lacunar, atherothrombotic, or cardiogenic embolism), evidence of infection, malignant disease, and/or premenopausal women. On the day the first blood sample was obtained and 1 year after, all individuals were evaluated using the National Institutes of Health Stroke Scale (NIHSS), modified Rankin Scale (mRS), Barthel Index (BI), and Clinical Dementia Rating (CDR) by a single examiner masked to the experimental protocol and level of circulating CD34+ cells. Hypertension, hyperlipidemia, and diabetes mellitus were defined based on the need for oral anti-hypertensive, anti-hyperlipidemic, or oral anti-diabetic drug therapy (or insulin), respectively, prescribed by the primary care physician. Smoking was defined as a history of > 2 years and/or smoking in the last year. Using a modification of the International Society of Hematotherapy and Graft Engineering (ISHAGE) Guidelines (Sutherland et al, 1996), the number of circulating CD34+ cells was quantified as described (Kikuchi-Taura et al, 2006) at the point of the entry and 1 year later. In brief, blood samples were incubated with phycoerythrin (PE)-labeled anti-CD34 antibody, fluorescein isothiocyanate (FITC)-labeled anti-CD45 antibody, 7-aminoactinomycin-D (7-AAD), and internal control (all of these reagents are in the Stem-Kit, BeckmanCoulter, Marseille, France). 7-AAD-positive dead cells and CD45-negative cells were excluded, and the number of cells forming a cluster characteristic of CD34+ cells (i.e., low side scatter and low-to-intermediate CD45 staining) was counted. The absolute number of CD34+ cells was calculated using the internal control. On the basis of our previous studies, the cumulative intraassay coefficient of variation of the measurement was 7.4% and test—retest intraclass correlation of the level of CD34+ cells is 0.88 (Taguchi et al, 2004a). For statistical analysis, JMP version 5.1J was used. Individual comparisons were performed using a Mann-Whitney's U-test, χ2-test, or two-tailed unpaired Student's t-test. Pearson's correlation coefficient was used to evaluate the correlation of the levels of CD34+ cells between measurements. Mean ± s.e. is shown.
Results
To investigate the possible relationship between circulating CD34+ cells and changes in neurologic status over the 1-year-study period, individuals were divided into two groups according to the level of circulating CD34+ cells at the point of the entry. Baseline characteristics of the groups are shown in Table 1. Comparing these groups, there were no significant differences in age, gender, etiology of cerebral infraction, hypertension, hyperlipidemia, diabetes mellitus, smoking, and drug treatments. In univariate analysis, each cerebrovascular risk factor, including hypertension (P = 0.46), hyperlipidemia (P = 0.35), diabetes mellitus (P =0.12), and smoking (P= 0.35), was not significantly correlated with a decrease in the numberofcirculatingCD34+ cells. Treatment with a Ca-channel blocker (P =0.73), angiotensin-converting enzyme (ACE) inhibitor (P = 0.053), angiotensin II receptor blocker (ARB) (P = 0.53), diuretics (P = 0.52), statins (P = 0.47), aspirin (P = 0.86), and/or ticlopidine (P = 0.80) also did not correlate with a consistent difference in the number of circulating CD34+ cells. Each cerebrovascular risk factor and particular drug treatment was also not associated with a significant difference in neurologic function in 1 year, based on NIHSS, mRS, BI, and CDR (data not shown). At the point of entry, there were no significant differences in neurologic or cognitive function between groups (Figures 1A-1D). Compared with levels of circulating CD34+ cells in non-stroke control subjects presented in our previous report (0.81 ± 0.06 cells/μL; age, 74.2 ± 0.7; n = 32) (Taguchi et al, 2008), the level of circulating CD34+ cells was significantly reduced in patients in the CD34+ cell low group in the current study (P < 0.001). There was no significant difference between the level of circulating CD34+ cells in the CD34+ cell high group (in the current study) and the previously reported value (P = 0.20; Taguchi et al, 2008). During the period of our observation, no patients had special exercise training, other than intensive rehabilitation in patients who had recurrent strokes.

The level of circulating CD34+ cells and neurologic function in the study group after 1 year. (
Baseline characteristic
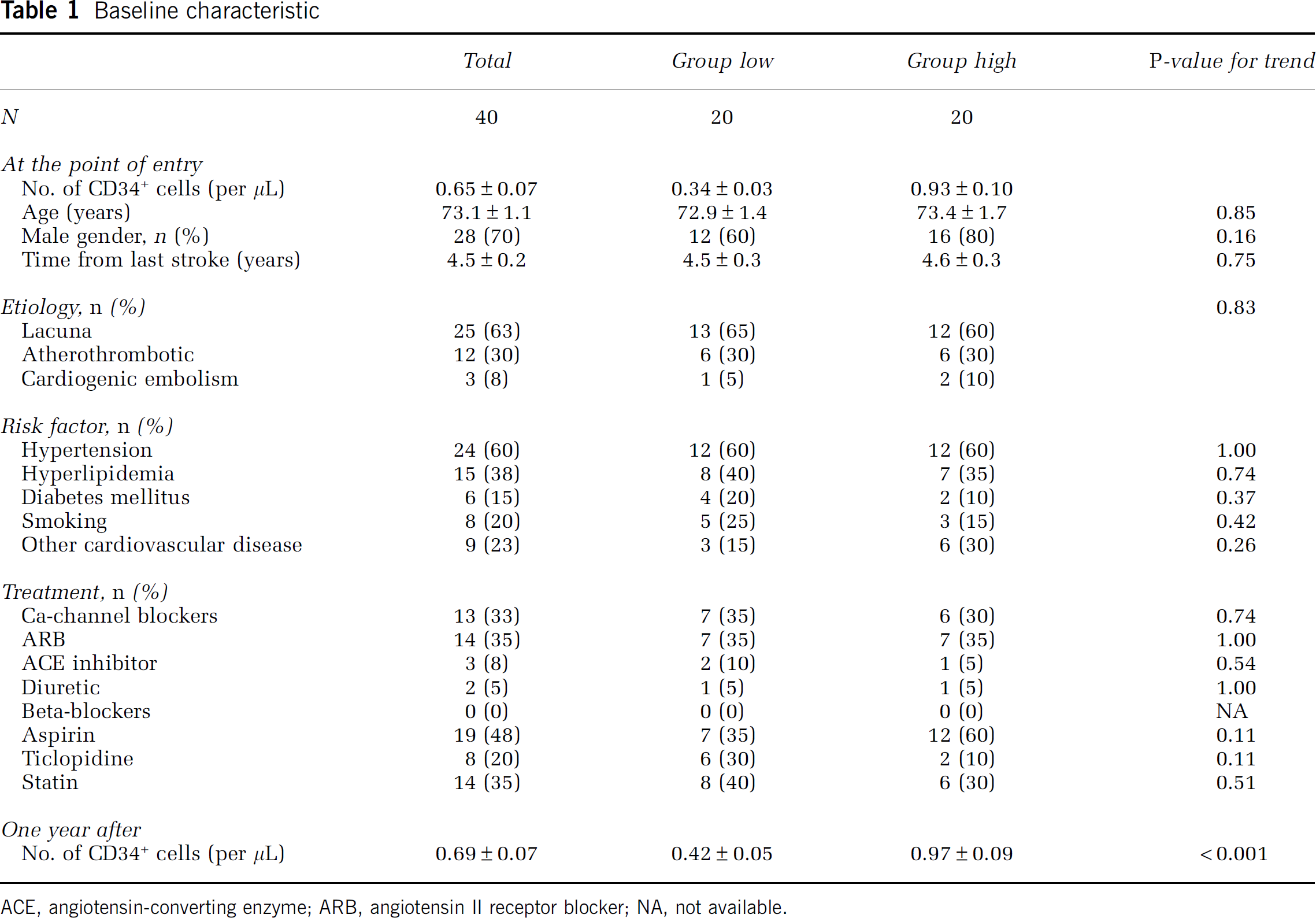
ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; NA, not available.
During the 12-month-study period, 5 patients had recurrent strokes (3 patients in the lower CD34+ and 2 in the higher CD34+ group, respectively; P = 0.63 between groups). After 12 months, neurologic and cognitive functions of all patients were reexamined, and changes in each score were recorded. Although there was no significant difference in the NIHSS score between groups (Figure 1E, P = 0.28), there was significant worsening in neurologic function, based on BI in patients with decreased levels of CD34+ cells versus the group with increased levels (Figure 1F, P = 0.04). Similarly, a trend towards worsening of mRS occurred in patients with decreased levels of CD34+ cells versus the group with increased levels, although these results did not achieve statistical significance (Figure 1G, P = 0.65). In terms of cognitive function, a significant worsening in the CDR score was observed in patients with decreased levels of CD34+ cells, compared with the higher CD34+ cell group (Figure 1H, P = 0.002). It is notable that no individual in the highest quartile (n = 10) for levels of CD34+ cells displayed worsening of the CDR or BI score over the I-year-study period. In the analysis of the patients without a recurrent stroke, a similar trend was observed (Figures 1I-1L), although the change of BI did not achieve statistically significant (P = 0.08). Analysis of the correlation coefficient of the levels of CD34+ cells between at the point of the entry and 1 year later revealed significant strong correlation in patients without recurrence (P < 0.001, R2 = 0.68).
Discussion
In this study, we have found that the level of circulating CD34+ cells has prognostic value for neural function in support of activities of daily living (BI) and cognitive function (CDR) in patients with a history of cerebral infarction. This result is potentially consistent with a role of CD34+ cells in maintenance of cerebral vasculature.
Similar to the correlation between mobilization of CD34+ cells and improved myocardial function after a coronary ischemic event (Wojakowski et al, 2006), mobilization of circulating CD34+ cells has been shown to correlate with functional recovery during the acute phase of cerebral infarction (Dunac et al, 2007; Yip et al, 2008). Our report herein shows a relationship between increased levels of CD34+cells and improved functional outcome even in the extensive phase after stroke. These observations may reflect a close relationship between angiogenesis and neurogenesis under physiologic (Louissaint et al, 2002), as well as pathologic (Taguchi et al, 2004b) conditions.
The level of EPCs can be quantified using an assay for endothelial colony formation or fluorescence-activated cell-sorting analysis with multiple markers, including CD34 and kinase insert domain receptor (KDR) (Werner et al, 2005). Although the population of CD34+ cells is enriched in EPCs, it comprises multiple and heterogeneous subpopulations, indicating the possible advantage of selectively quantifying EPCs. However, measurement of EPCs is quite inexact, as large variations in their levels have been reported (i.e., by ~ 100-fold between reports) (Fadini et al, 2006a; Werner et al, 2005). Thus, there appears to be a need to standardize measurement of EPCs, in addition to a requirement for a relatively large blood volume to do the assay (for example, Loomans et al collected a 60 mL blood sample for EPC analysis) (Loomans et al, 2004). Our method for quantification of CD34+ cells is simple, reproducible (Kikuchi-Taura et al, 2006) and requires only 200 μL of peripheral blood. The latter method is suitable for screening a broad group of patients at risk for cerebrovascular disorders. Furthermore, CD34+ cells have been shown to secrete multiple growth/angiogenesis factors (Majka et al, 2001), contributing to maintenance of the microvasculature in addition to serving as a source of EPCs. These considerations indicate the value of quantitating peripheral CD34+ cells as a clinical biomarker in patients with vascular disease, not only as a substitute for quantifying EPCs.
In conclusion, our results indicate that circulating CD34+ cells in patients with cerebral ischemia have a positive impact on the course of disease, in terms of maintenance of neurologic function. In contrast, decreased levels of circulating CD34+ cells, possibly because of ‘exhaustion’ of the bone marrow or inability to mount an increase in cell counts, are associated with deterioration of neurologic status. Taken together with our previous results indicating that the level of circulating CD34+ cells can be correlated with cerebral blood flow and cerebral metabolic rate in patients with chronic cerebral hypoperfusion (Taguchi et al, 2004a), our present findings provide further support for a contribution of circulating CD34+ cells in maintenance of neurologic function in settings of ischemic stress. Although further basic and clinical studies will be required, we speculate that treatments with the goal of increasing levels of circulating CD34+ cells have the possibility of improving neurologic outcome in patients with impaired cerebral microcirculation.
Footnotes
Acknowledgements
We thank K Obata and Y Okinaka for technical assistance.
We declare that we have no conflicts of interest.