512 Therapeutic administration of plasminogen activator inhibitor-1 prevents hypoxic-ischemic brain injury in newbrons
D. Yang1, N. Nemkul1, D. Lawrence2, D. Lindquist3 and C.-Y. Kuan1
1Pediatrics, Division of Neurology, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio; 2Internal Medicine, University of Michigan, Ann Arbor, Michigan; 3Radiology, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA
Objectives: Neurovascular proteases, including the matrix metalloproteases (MMPs) and plasmniogen activators (tPA and uPA), have important pathological functions in adult brains, but their roles in perinatal cerebrovascular diseases are less certain. In the Rice-Vannucci model of neonatal cerebral hypoxia-ischemia (HI), the induction of MMP-9 activity only occurred after the onset of much irreversible brain damage. In contrast, we recently showed that cerebral HI rapidly induces the parenchymal tPA activity in immature brains, suggesting that tPA may be an early mediator of neonatal HI brain injury (Adhami et al, 2008). The objectives of the present study are twofold. First, we wish to determine whether inhibition of the brain tPA and uPA activity with plasminogen activator inhibtor-1 (PAI-1) prevent MMP-9 activation after HI in newborn brains. Second, does brain infusion of PAI-1 have an overall therapeutic efficacy?
Methods: P7 Wistar rat pups were challenged by the Rice-Vannucci model of neonatal cerebral HI (unilateral carotid artery-ligation plus 90-min 10% oxygen). After the HI insult, animals received intracerebroventricle (ICV) injection of saline or PAI-1. The brain protein samples were prepared at 4 and 24 h of recovery for biochemical analysis, including plasminogen activator (tPA/uPA) activity assay, MMP zymogram, and occludin-immunoblot. Magnetic Resonance Imaging (MRI) analysis, including T2, apparent diffusion coefficient (ADC) and diffusion tensor imaging (DTI), were also performed at 24 h of recovery. The extents of brain damage in saline- or PAI-1-injected animals were compared after 7 days of recovery to determine dose-response curve and therapeutic window of the PAI-1 treatment.
Results: We found that the PAI-1 treatment greatly reduced tPA and uPA activities at both 4 and 24 hrs, and blocked MMP-9 induction at 24 hrs of recovery. PAI-1 therapy also prevented HI-induced extravasation of immunoglobulins and degradation of the BBB-associated proteins. Moreover, the PAI-1 treatment decreased the extent of brain edema, cortical cell death, and white-matter oligodendrocyte degeneration at 24 to 48 h of recovery based on multiple biochemical, MRI, and histological assays. Finally, PAI-1 treatment provided a dose-dependent preservation of brain tissues at 7 days of recovery, and the therapeutic window is at least 4 h after HI.
Conclusion: Activation of the brain parenchymal PA system precedes and is required for MMP-9 induction in the experimental (Vannucci) model of neonatal HI brain injury. Overall, PAI-1 therapy protects against HI-induced BBB damage and brain edema in immature brains. Future studies are warranted to test whether a similar pathological mechanism also occurs in infants diagnosed with hypoxic-ischemic encephalopathy.
907. Alternative splicing of BCL-X regulates neural cell death after neonatal hypoxia-ischemia
J.-M. Lee, A. Ford, P. Yan, E. Gonzales, R. Perez and Q. Xiao
Neurology, Washington University School of Medicine, St Louis, Missouri, USA
Objectives: Perinatal hypoxia-ischemia (H-I) is increasingly recognized as a common neurological disorder. What distinguishes perinatal H-I from adult stroke is the prominence of apoptosis as a form of cell death. Preliminary evidence suggests that pre-mRNA alternative splicing may play a role in the regulation of apoptosis. For example, the apoptotic regulatory gene, bcl-x, generates two mRNA isoforms with opposing actions: Bcl-xL (the longer form) is anti-apoptotic, while Bcl-xS (the short form) is pro-apoptotic. This study aimed to investigate the role of alternative splicing of Bcl-x in neural injury following neonatal H-I.
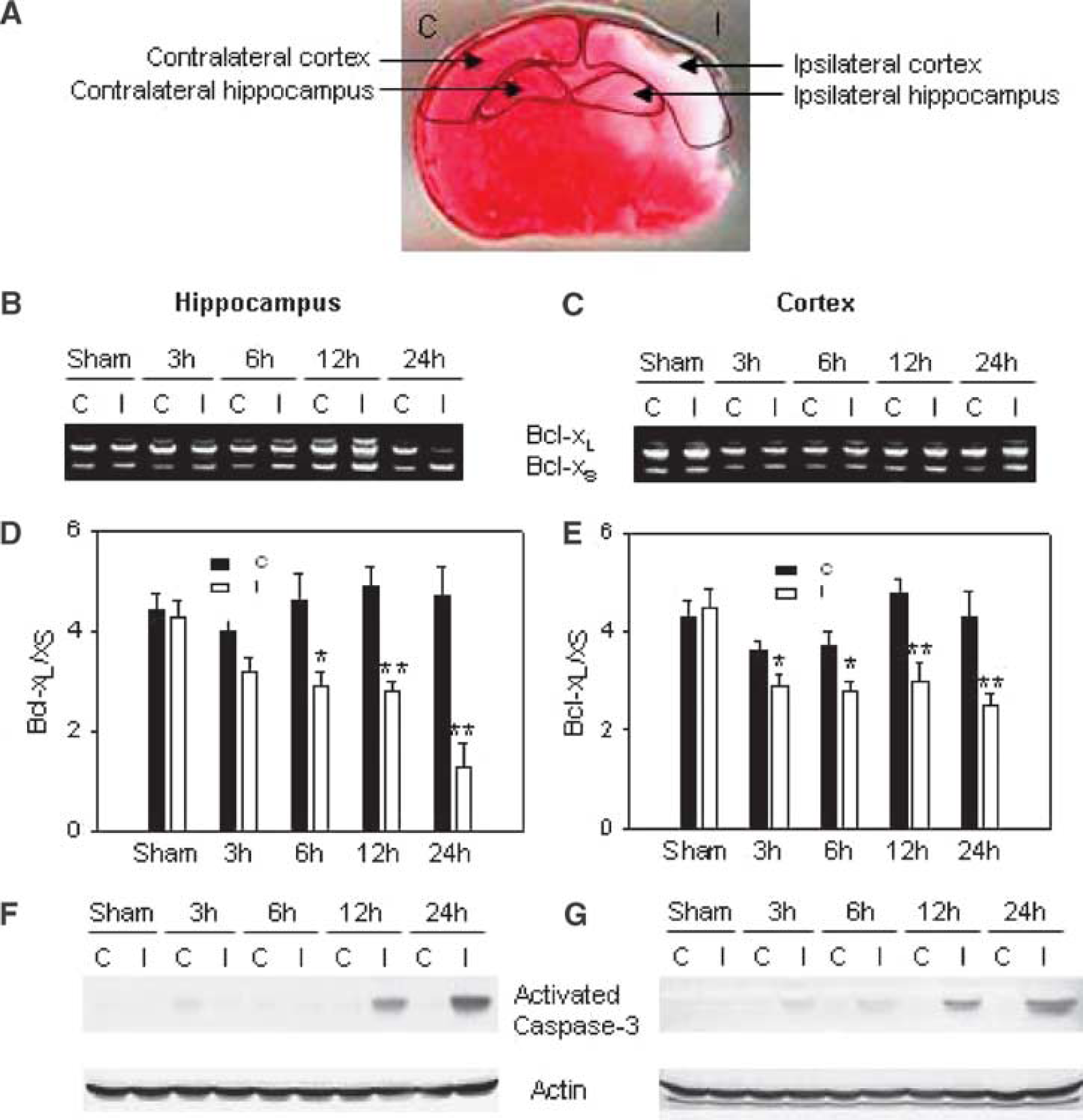
Methods: P7 Sprague Dawley rat pups were subjected to unilateral carotid ligation and hypoxia (8% O2 for 2.5 h). Bcl-x splicing was determined by RT-PCR from the ischemic and contralateral hippocampus and cortex. Because oligodendrocyte progenitors (OPs) are particularly vulnerable to H-I at this age, Bcl-x splicing was evaluated in OP cells induced to undergo apoptosis with C2-ceramide. Cell death was assessed by LDH assay and DNA fragmentation. Western blotting was used to detect Bcl-x, activated caspase-3 and CUG-BP1. Minigene mutagenesis experiments and RNA EMSA were performed to examine RNA binding proteins that might regulate Bcl-x splicing. RNA interference was employed to knockdown Bcl-xS and CUG-BP1 in vitro.
Results: Neonatal H-I resulted in a significant decrease of the Bcl-xL and a concurrent increase of Bcl-xS in the ischemic hippocampus and cortex (well before procaspase-3 cleavage), while the contralateral side remained unchanged compared to controls. Within 1 h of exposing OP cells to C2-ceramide, the Bcl-xL/Bcl-xS ratio was decreased prior to capase-3 activation and cell death. Specific knockdown of Bcl-xS (without significantly altering Bcl-xL) attenuated ceramide-induced cell death. Using a transfected bcl-x minigene, we identified a UG rich motif immediately downstream of Bcl-xL 5′ spicing site that altered Bcl-x splicing patterns. Supershift analysis indicated that splicing factor CUG-BP1 bound to this UG motif, and dephosphorylation of the CUG-BP1 abolished this RNA-binding activity. Overexpression of CUG-BP1 in OP cells altered splicing of the Bcl-x, favoring Bcl-xL, and protected cells from ceramide-induced cell death. In contrast, knockdown of CUG-BP1 aggravated cell vulnerability to ceramide. While CUG-BP1 is found predominantly in the nucleus, ceramide induced its translocation to the cytosol and consequently decreased the Bcl-xL/Bcl-xS ratio in OP cultures. In the brains of neonatal rats, CUG-BP1 decreased in nuclei within 3 h after H-I (concurrent or prior to Bcl-x splicing changes).
Neonatal H-I alters Bcl-x alternative splicing.
Conclusions: Bcl-x alternative splicing may be an important regulatory mechanism for apoptosis following hypoxia-ischemia in neonates. The splicing factor CUG-BP1 appears to be a critical regulator of Bcl-x pre-mRNA splicing, and is altered following H-I. These results raise the possibility that regulators of alternative splicing may provide a novel target for neuroprotective intervention, increasing pro-survival factors (Bcl-xL) while decreasing anti-survival factors (Bcl-xS).
685. Effect of the cannabinoid agonist win 55212–2 on remyelination and neurogenesis after newborn rat brain hypoxia-ischemia
D. Fernandez-Lopez1, J.A. Martínez-Orgado2, I. García-Yébenes1, R. Cañadas1, O. Hurtado1, M.A. Moro1 and I. Lizasoain1
1Pharmacology, Complutense University of Madrid; 2Neonatology, Alcorcón Hospital Foundation, Madrid, Spain
Background and purpose: Cannabinoids have emerged as interesting neuroprotective agents which efficacy has been proven in several animal models of acute and degenerative CNS diseases.1 More recently, the endocannabinoid system has also been involved in the modulation of the proliferation, survival and differentiation of neural stem cells and progenitors,2 as well as in the prevention of oligodendrocyte cell degeneration and death under pathological conditions.3,4
The CB1 and CB2 cannabinoid receptor agonist WIN 55212–2 (WIN) has shown a neuroprotective effect after experimental newborn brain hypoxia-ischemia (HI),5 but its possible effects on the remyelination, proliferation and neurogenesis in this animal model remain unexplored. The main purpose of this work is to test the potential effect of the treatment with WIN in the aforementioned processes, which ocurrence strongly determine the long-term functional outcome after newborn brain HI.
Methods: 7-day old (P7) Wistar rat were submitted to unilateral permanent section of the common carotid artery, followed by the exposure of the rat pups to 90 min of hypoxia (8% O2/92% N2). The pups were administered either WIN (1 mg/kg i.p.) or vehicle twice daily for 7 days after HI, and BrdU (50 mg/kg i.p.) twice daily from days P12 to P14 (5 to 7 days after HI). The immunohistochemical density of myelin binding protein (MBP) was measured at the end of the treatment period in several white matter areas. The total number of BrdU+ cells in the ipsilateral SVZ was estimated using unbiased stereology at 7, 14 and 28 days after HI. Finally, the number of neuroblasts (Dcx+ and BrdU+/Dcx+ cells) was quantified in the adjacent striatum 14 and 28 days after HI.
Results: HI induces a significant decrease of the density of MBP 24 h after the insult. The treatment with WIN enhanced the recovery of the density of MBP in the ipsilateral external capsule 7 days after HI, reaching values similar to those observed in the non-injured hemisphere.
The total number of BrdU+ cells in the ipsilateral SVZ was significantly higher in the WIN-treated animals than in the non treated animals (182570±11049 versus 144373±7877, P<0.01) at the end of the treatment with WIN (P14). The presence of double-positive cells for BrdU and Dcx in the adjacent striatum at P21 was higher in the WIN-treated animals, suggesting that some of the BrdU+ cells observed in the SVZ after the treatment with WIN might have migrated and adquired the neuroblast phenotype at P21.
Conclusions:
WIN 55212–2 facilitates the remyelination of the injured white matter 7 days after HI.
WIN 55212–2 transiently increases the proliferation of neural stem cells in the ipsilateral SVZ 7 days after HI, as well as the presence of newly-generated neuroblasts in the injured striatum 14 days after HI.
539. Prolonged decrease in cerebral blood flow following a transient severe hypoxia in late gestation fetal sheep
A. Baburamani1, E. Yan2 and D. Walker1
1Physiology, Monash University; 2National Trauma Research Institute, The Alfred Hospital, Melbourne, VIC, Australia
Background: Transient hypoxic and/or asphyxic episodes are major contributors to brain injury in the developing fetus. Brain regions susceptible to hypoxic injury may associate with the degree of perturbation of regional cerebral blood flow (RCBF) during and after such insults.
Aim: To determine changes of global and RCBF in late gestation fetal sheep where transient systemic asphyxia was induced by complete umbilical cord occlusion (UCO) for 10 mins.
Methods: At 124–127 days gestation (term 147 days), fetal sheep underwent surgery for implantation of catheters and the placing of an inflatable cuff around the umbilical cord. UCO (n = 4) was induced by inflating the cuff for 10 min, while for control fetuses (n = 5) the cuff was not inflated. An ultrasonic crystal probe was placed directly above the sagittal sinus to measure blood flow velocity (SSbfv). Mean arterial blood pressure (MAP) and heart rate (HR) were also measured throughout the experiment. At 130–132 days, differently colored microspheres were injected to determine RCBF at −1, +1, +5, +10, and +24 h with respect to UCO or sham manoeuvre.
Results: During the 10 min UCO, MAP increased and peaked at 2 min and then fell becoming hypotensive, until the cuff was released. Bradycardia was observed for the duration of the UCO. MAP and HR had returned to the basal levels by +30 min. SSbfv followed the changes of MAP during the UCO, but it remained significantly below normal values for up to +12 h before returning to the pre-UCO level. Before UCO, blood flow to various brain regions was between 200–300 ml/min/100 g tissue. UCO significantly decreased blood flow to all brain regions (brainstem, grey matter, white matter, diencephalon, cerebellum, hippocampus, striatum, subventricular white matter) at +1 h, +5 h, and +10 h post-UCO. The greatest falls of RCBF occurred in the midbrain, frontal and occipital cortex (−164%, −155%, −177%, respectively). At 24 h after UCO, blood flow to all brain regions was not different from the pre-UCO (−1 h) values.
Conclusions: A 10 min severe fetal hypoxia induced transient changes in MAP and HR, but prolonged decreases in RCBF for up to 10 h, and significant persistent reduction in SSbfv for up to 12 h following UCO. This study has validated SSbfv as a sensitive and reliable measurement for determining cerebral blood flow when compared to the direct measurement by microspheres. It is unclear if the prolonged decrease of cerebral blood flow is concomitant with depressed cerebral metabolism, or dissociation of cerebral blood flow and metabolism. However, it is notable that it occurs despite recovery of fetal systemic physiological parameters, suggesting that currently-used clinical observations of fetal well-being would not be able to detect the prolonged derangement of cerebral perfusion.
483. Cerebral oxygen metabolism (CMRO2) reactivity to hypercapnia in neonates with severe congenital heart defects measured with diffuse optics
T. Durduran1,2, M.N. Kim2, E.M. Buckley2, C. Zhou2, G. Yu2, R. Choe2, S.M. Durning3, S. Mason4, L.M. Montenegro5, S.C. Nicholson5, M.E. Putt6, R.A. Zimmerman7, J. Wang1, J.H. Greenberg8, J.A. Detre1,8, A.G. Yodh2 and D.J. Licht4
1Radiology; 2Physics and Astronomy, University of Pennsylvania; 3Division of Respiratory Therapy; 4Divison of Neurology; 5Division of Anesthesiology and Critical Care, Children's Hospital of Philadelphia; 6Department of Biostatistics & Epidemiology, University of Pennsylvania; 7Division of Neuroradiology, Children's Hospital of Philadelphia; 8Neurology, University of Pennsylvania, Philadelphia, Pennsylvania, USA
Objectives: Optical, ‘diffuse correlation spectroscopy’ (DCS) is a novel technology for non-invasive transcranial CBF monitoring. When hybridized with ‘near-infrared spectroscopy’ (NIRS) to measure cerebral oxy-, deoxy- and total-hemoglobin (HbO2, Hb, THC), the instrument permits calculation of cerebral metabolic rate of oxygen extraction (CMRO2). DCS was previously validated against arterial spin labeled perfusion MRI in neonates with severe congenital heart defects. In this study, we estimate changes of CMRO2 in this population due to hypercapnia.
Methods: A DCS/NIRS instrument with a MRI compatible optical probe was used to measure thirty-three neonates (22 hypoplastic left heart syndrome, 11 transposition of the great arteries) who were scheduled for cardiopulmonary bypass. All patients were full term at birth (37 to 42 weeks). All were prepared for surgery with protocolized ventilation and anesthesia (Fentanyl 5–10 μg/kg, pancuronium 0.2 mg/kg). Vital signs including blood pressure, electrocardiogram, pulse oximetry and end-tidal CO2(EtCO2) were continuously monitored. After confirmation of normocapnia (pCO2 = 40–45 mm Hg) by arterial blood gas sampling baseline data was acquired for 10 min. CO2 was then added to the gas mixture to achieve an FiCO2 of 2.7% as measured by capnometry. Conventional anatomic MRI sequences were obtained while the gases were equilibrating (15 min). Continuous optical data was acquired throughout the procedure. At the end of this period, arterial blood gas samples were drawn to confirm higher PaCO2. Oxygen extraction fraction (OEF) was estimated from NIRS data assuming a compartmentalized model for the vasculature and baseline values for microvascular blood oxygenation and volume. CMRO2 was then calculated as the product of OEF and CBF using a standard model.
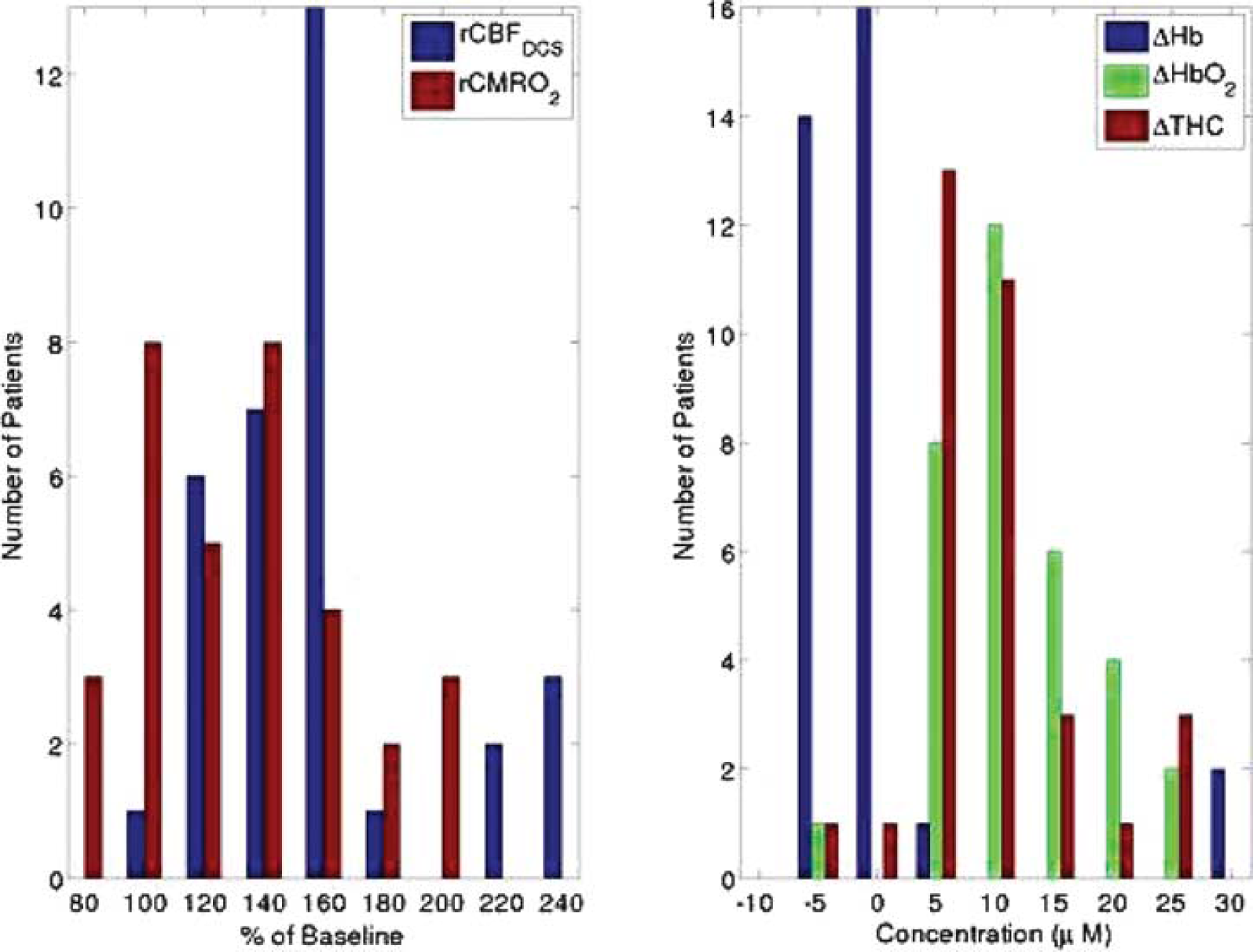
Results: Mean (±standard error) changes in CBF of 59±6%, HbO2 of 11.0±1.1 μmol/L, Hb of −2±0.4 μmol/L, THC of 9.4±1.1 μmol/L, CMRO2 of 130±7% and EtCO2 of 21±2 mm Hg were observed (Figure 1), and vascular reactivity was calculated to be 4.2±1.6 %CBF/mm Hg. All changes were significant (P<0.05).
Conclusions: CBF-CO2 reactivity was intact and consistent with literature values of 1.5–9% CBF change/mm Hg.1–3 Calculated CMRO2 increased significantly with hypercapnia in most patients, though the magnitude of this change depended on assumed baseline values. This increase persisted when assumed values were varied across a (wide) physiological range. This finding contrasts with the common understanding that, in healthy persons, CMRO2 is unaffected by hypercapnia. The observed increase in CMRO2 in neonates with congenital heart disease suggests that baseline CMRO2 may be reduced in response to very low CBF (10.2±0.8 ml/min/100 g), and supports the notion that hypercapnia may be neuroprotective. The next phase of this study will employ an improved NIRS instrument and algorithm to reduce the number of required assumptions.
725. Comparison of independent techniques for measuring cerebral venous oxygenation in neonates
K.M. Tichauer1, J.T. Elliott1,2, J.A. Hadway1,3, T.-Y. Lee1,2,3 and K. St Lawrence1,2
1Imaging Division, Lawson Health Research Institute; 2Medical Biophysics, University of Western Ontario; 3Imaging Research Laboratories, Robarts Research Institute, London, ON, Canada
Objectives: Measurement of the cerebral metabolic rate of oxygen (CMRO2) by near-infrared spectroscopy (NIRS) requires knowledge of cerebral venous oxygenation. In previous studies from our group, venous oxygenation was calculated from the cerebral concentration of deoxy-hemoglobin (HHb) and assuming the cerebral blood volume (CBV) is comprised of 25% arterial blood and 75% venous blood.1 However, a study in sick children suggested that the arterial-to-venous ratio varies substantially from patient to patient.2 The purpose of the present study was to compare our HHb technique of measuring cerebral venous oxygenation with two alternate NIRS techniques—the partial venous occlusion3 and head tilt4 methods—that do not rely on assumptions of blood compartment ratios. Measurements were obtained over a range of arterial blood oxygenation levels in piglets and cerebral venous blood samples were collected for gold standard measurements of cerebral venous oxygenation.
Methods: Experiments were conducted on piglets (<1 week) that were anesthetized with isoflurane. Cannulae were inserted through a burr hole in the skull into the superior sagittal sinus and into an ear vein for administration of the NIRS contrast agent, indocyanine green. Following surgery, cerebral venous oxygenation was measured using the three independent NIRS techniques at fraction of inspired oxygen levels of 50%, 21%, and 10%. The HHb technique relied on normalizing the NIRS measurement of HHb by the CBV, which is determined using an indicator-dye dilution method.1 The second and third techniques required measuring changes in cerebral blood oxygenation following either partial venous occlusion of the jugular veins or a 15° negative head tilt—actions that resulted in cerebral oxygenation changes from only the venous compartment.
Results: Data were collected from nine piglets (5 males, 4 females: 2.8±1.1 days, 1.8±0.1 kg) over a sagittal sinus oxygenation range of 12–90%. Similar statistically significant correlations (P<0.05) were observed for all three NIRS calculations of venous oxygenation compared to corresponding superior sagittal sinus blood oxygenation (R2 = 0.71, slope = 1.01 for the HHb technique; R2 = 0.77, slope = 0.74 for the partial venous occlusion technique; and R2 = 0.72, slope = 0.82 for the head tilt technique).
Conclusions: The statistically significant correlations between all NIRS techniques and the gold standard suggest that each technique could be used interchangeably for measuring CMRO2. The agreement between the techniques also suggests that the assumed 25:75 ratio of arterial-to-venous blood used by the HHb technique is reasonable in the newborn piglet; however, the partial venous occlusion and head tilt techniques have the advantage of not relying on this assumption, which could be beneficial to clinical studies. The advantage with the HHb technique is that it does not require any manipulation of the patient and, as such, might be associated with a higher success rate. Future clinical studies are needed to assess this assertion.
References
1.
AdhamiFYuDYinWSchloemerABurnsKALiaoGDegenJLChenJKuanCY. Deleterious effects of plasminogen activators in neonatal cerebral hypoxia-ischemia. Am J Pathol2008;172:1704–16.