
Abstract
Foreign body migration in the deep spaces of the neck is particularly concerning due to the increased risk of damage to the great vessels and nerves. In addition, migration often cannot be easily predicted as objects may travel outside the confines of anatomic fascial planes. Although patients may be asymptomatic for years prior to presentation, timely removal of foreign bodies is ideal to preclude injury to important vascular and neurological structures as well as to prevent the development of recurrent infections and foreign body reactions. The authors report two cases of removal of migrated foreign bodies that presented at their institution. In one case, they report the use of intraoperative computed tomography (CT) imaging to help locate the position of a migrating dental needle. In another, they report the retrieval of a bullet fragment six months after the initial trauma. The classic method for retrieval of foreign bodies within the craniomaxillofacial complex centered around review of static radiographic imaging and a “blind,” broad exposure of the site in an attempt to localize and retrieve the material. This often resulted in iatrogenic injuries to surrounding structures or migration of the foreign body to a location, which may cause the patient additional harm. The utilization of intraoperative CT technology and computer navigation affords the craniomaxillofacial surgeon an additional tool for retrieval of these foreign bodies, often in a manner that affords minimally invasive surgical approaches, identification of vital structures within the operative field, and decrease in overall operative time for removal. Referral to institutions, which have this technology, should be considered early in the operative care of patients who encounter retained foreign bodies in the craniomaxillofacial region.
Foreign body penetration in the craniomaxillofacial region may be secondary to a variety of causes, ranging from the traumatic, such as gunshot wounds to the head and neck or shrapnel from explosives, impalement from motor vehicle or industrial accidents, to iatrogenic, such as broken medical instrumentation or dental anesthetic needles. While some patients may initially be asymptomatic, removal of these foreign bodies in their entirety should be seriously considered in a timely manner to avoid potentially catastrophic damage to the complex neurovascular structures of the region as well as recurrent infections, abscess formation, and development of draining sinus tracts. Although the mechanism of foreign body migration is not altogether clear, it is thought that this process may be due to the contraction of the pharynx during the acts of mastication and swallowing, resulting in penetration of the object into the surrounding soft tissues, nerves, and vasculature.1 2 Some patterns of foreign body migration may be predicted, for example, needles fractured during inferior alveolar nerve blocks that are utilized for dental procedures are quite commonly found in the pterygomandibular region of the infratemporal fossa.2 3 However, retained foreign bodies may also migrate outside the confines of anatomic planes, posing a challenge for craniomaxillofacial surgeons attempting to accurately localize and to remove the object to prevent further harm.
Surgical removal of foreign bodies in the craniomaxillofacial complex is complicated by multiple factors, such as the material nature of the foreign body in question and the chronicity of the injury. The craniomaxillofacial surgeon must take this into consideration prior to intervention; however, there is no general consensus on timing and technique with regards to surgical removal of these foreign bodies. The aim of this study is to discuss the indications and considerations for foreign body removal, the use of specific imaging modalities for diagnosis and treatment, as well as the intraoperative use of surgical navigation systems in this patient population, with case presentations of two patients who underwent removal of a migrating foreign body which was localized using either preoperative or intraoperative computed tomography (CT) imaging at our institution. Utilizing this information, we have also outlined a potential treatment algorithm for removal of foreign bodies.
Clinical Indication and Timing for Removal
A review of current literature illustrates several important concepts in the management of retained and migrating foreign bodies in the head and neck region. Although it had once been recommended to only remove retained foreign bodies if they are causing symptoms, it is now generally advocated that removal be undertaken as soon as possible to minimize the risk of migration.4 In the long term, foreign bodies that are retained within the soft tissues of the head and neck can result in localized inflammatory reactions and scarring that can complicate later surgical retrieval if the patient should require intervention secondary to worsening symptoms. Chronic retention may also result in the development of soft tissue infection, further complicating regional anatomy.5 Retained foreign bodies may also result in a gamut of predictable and/or unusual complications varying from localized pain at the site of impaction to hearing loss or dysphagia, depending on the path of migration.3 6 Absolute clinical indications for foreign body removal include airway compromise, damage of local vascular structures, and intimate contact with other viable structures, such as sensory or motor nerves, and intimate contact with muscles where the development of fibrosis or scarring may result in the decrease in function, such as the extraocular muscles. Relative indications include the presence of grossly contaminated wounds, palpable soft tissue foreign bodies concerning to the patient, and whether removal of object is possible without significant risk of damage to vital structures. Upon the initial inciting event, patients should be advised to minimize repetitive muscular activities pertinent to the region of injury until accurate localization of the foreign body is performed.
Imaging Modalities
The use of imaging technology, such as conventional radiographs, ultrasonography, CT, or magnetic resonance imaging (MRI), is valuable in the localization of foreign bodies. Ultrasonography may serve as a first-line imaging modality, especially for radiolucent foreign bodies. Studies have previously reported a sensitivity of 95% and a specificity of 86% when utilizing ultrasonography for the localization of foreign bodies consisting of organic, radiolucent material, such as wood.7 8 It is most beneficial for locating superficial foreign bodies, but its accuracy may be compromised by the presence of air. This may prove to be especially problematic in the craniomaxillofacial complex, if the foreign body penetrates or tracks into the paranasal sinuses. Ultrasonography should be considered in patients with acute foreign body penetration who have not undergone previous retrieval attempts.
While conventional radiographs are useful for the identification of radiopaque substances, the accuracy of this modality may be compromised by the dimensions of the object. Thus, CT imaging, or cone beam CT, is a superior modality for localizing retained foreign objects, with the capacity for identifying both radiopaque and radiolucent foreign bodies. Most notably, the accuracy of CT imaging is not compromised by the presence of air. The use of CT imaging to locate retained foreign bodies was first described in 2002, and both in vitro and in vivo studies have shown CT imaging to be more sensitive to MRI and plain radiography when determining the size and location of a retained foreign body in the deep tissues of the neck.9 10 11 12 Patients presenting with retained foreign bodies should undergo not only preoperative imaging to aid with planning, but also intraoperative CT, if feasible, to allow for complete visualization of the foreign object and surrounding soft tissue, neural, and vascular structures. One of the critical aspects of utilizing CT imaging for the localization of radiopaque and/or radiolucent foreign bodies is for the operating surgeon to be comfortable with alteration of the Hounsfield units on the CT scan to assist with determining the presence of the foreign body. The ability to manipulate the Hounsfield units easily and accurately interpret the differences in appearance, will significantly increase the specificity of localizing the foreign body and assist with removal.
Surgical Navigation for Foreign Body Removal
The classic method for retrieval of foreign bodies within the craniomaxillofacial complex centers around review of static radiographic imaging and a “blind,” broad exposure of the site in an attempt to localize and retrieve the material. This often resulted in iatrogenic injuries to surrounding structures, migration of the foreign body to a location, which may cause the patient additional harm, or poor aesthetic outcomes. The utilization of intraoperative CT technology and computer-based surgical navigation affords the craniomaxillofacial surgeon an additional tool for retrieval of these foreign bodies, often in a manner that affords minimally invasive surgical approaches, identification of vital structures within the operative field, and decrease in overall operative time for removal. Referral to institutions, which have this technology, should be considered early in the operative care of patients with retained foreign bodies in the craniomaxillofacial region, limiting “blind” approaches to selective cases where the foreign body is definitively identified as superficial and palpable.
A systematic review of the craniomaxillofacial literature illustrates the usefulness of surgical navigation in improving intraoperative precision and surgical planning in the areas of traumatology, orthognathic surgery, oncologic and reconstructive surgery, and skull-base surgery.13 Currently, there is a deficit of randomized clinical studies focusing on the influence of surgical navigation on postoperative outcomes in patients undergoing foreign body removal; much of the literature is characterized by studies utilizing cadaver models or retrospective case series. In a human cadaver model of foreign body penetration in the head and neck region, the use of a computer navigation system resulted in a decreased time to localization and removal of objects of varying compositions as well as smaller incision lengths compared with control models in which navigation was not utilized.14 A retrospective case series examined the postoperative outcomes of five patients who underwent surgical navigation in the removal of maxillofacial foreign bodies and showed that the navigation system was accurate to within 0.8 mm.15 Gröbe et al compared a retrospective review of 50 patients, 32 of whom underwent imaged-guided surgical removal of bullet fragments in the maxillofacial region and 18 who did not.16 The use of surgical navigation was associated with fewer intra- and postoperative complications and a trend toward a reduction in total operative time compared with the control group. These studies not only illustrate the potential for surgical navigation to improve outcomes of foreign body removal but also motivate the need for further study of the use of this technology in this patient population. Future studies could focus on providing a cost—benefit analyses and a potential mechanism for identification of which subset of patients would most benefit from the use of intraoperative computer-guided surgical navigation.
Case Example A: Intraoperative Computed Tomograpy-Guided Removal of Iatrogenic Foreign Body
The patient was an otherwise healthy 60-year-old male who was referred for the removal of a broken dental injection needle after two separate unsuccessful retrieval attempts were made outside of our institution. It was decided to proceed with removal of this foreign body using intraoperative computer navigation.
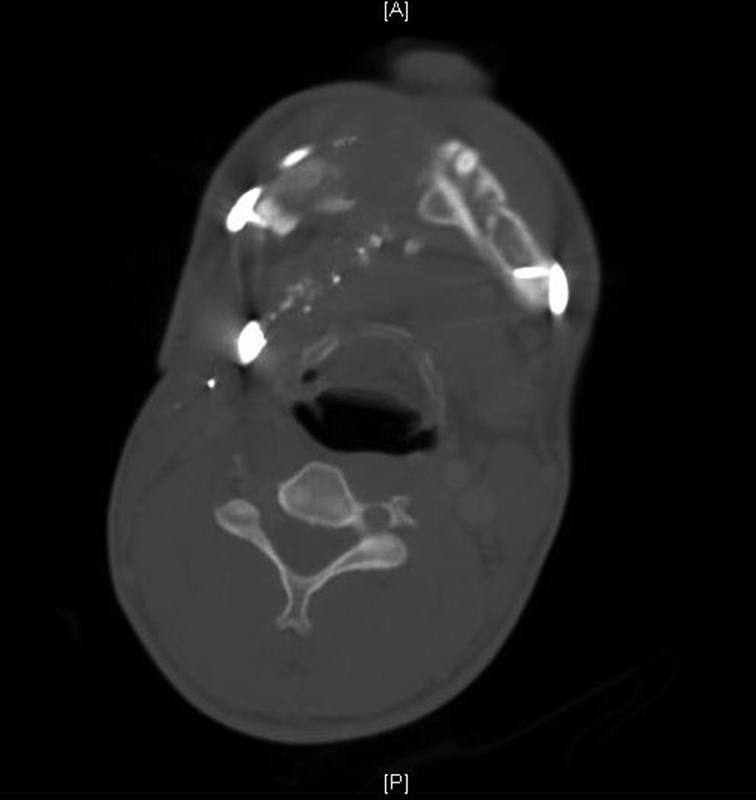
An immediate preoperative CT scan of the region of the right mastoid process was conducted to positively identify the current location of the broken dental needle near the right mastoid process. Calibration of skeletal reference points was performed, and intraoperative navigation was conducted throughout the surgical procedure to identify landmarks and to prevent iatrogenic injury to the patient. A curvilinear incision was made posterior to the skeletal external auditory canal, beginning approximately at the level of the superior aspect of the cartilaginous external auditory canal and terminating with an elliptical extension on the right lateral neck. Electrocautery was used to open this curvilinear incision to the level of the temporal bone/mastoid region. The subperiosteal plane was identified, and inferior dissection was accomplished using Freer elevators; the sternocleidomastoid muscle was released from the mastoid process, to allow for complete visualization of the mastoid. Verification of positioning of the broken needle was performed with the BrainLab software unit: the needle was confirmed to be medial and inferior to the mastoid tip. Blunt-tipped dissection occurred with Mosquito hemostats in the direction of the expected course of the facial nerve branches. The branches of the facial nerve were never visualized during the dissection, despite close monitoring throughout for potential involvement. After creation of a soft tissue pocket, two additional CT scans were sequentially obtained to triangulate the location of the needle within the soft tissue. After the last scan, the broken needle was identified between the styloid process and the medial border of the mandible in the parotid gland and was removed with a hemostat (Figs. 1, 2).
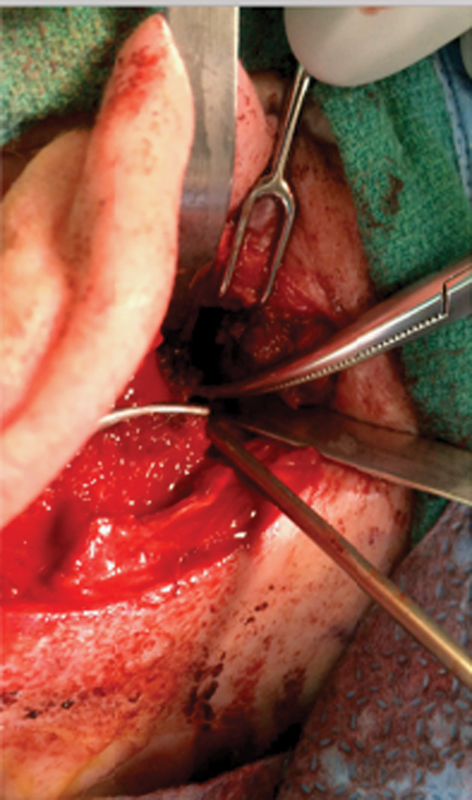
A curvilinear incision was made in an existing skin crease posterior to the skeletal external auditory canal. The broken needle was identified between the styloid process and the medial border of the mandible in the parotid gland and was removed with a Mosquito hemostat.

A 3.5-cm fragment of broken dental needle removed after triangulation using 3D intraoperative CT imaging. 3D, three dimensional; CT, computed tomography
Immediately upon extubation, the patient was noted to have weakness of the right facial nerve, although gross continuity of the nerve was confirmed as evidenced by some facial muscle movement along all five branches of the nerve. Findings were most consistent with neuropraxia, At a 5-month follow-up visit, the patient reported improved right facial nerve weakness, which was also clinically apparent on physical examination.
Case Example B: Preoperative Computed Tomography Imaging for Removal of Retained Foreign Body
The patient was a 30-year-old male with a past medical history of gunshot wound to the right mandible. At the time of the original trauma, he underwent emergent tracheostomy, evacuation of cervical hematoma, removal of bullet fragments, and excision of an unsupported segment of the mandible. His recovery was complicated by multiple irrigation and debridement procedures with eventual removal of hardware and finally, placement of allogenic bone graft in the right mandible. Approximately 6 months after the initial trauma, he present to the Craniomaxillofacial Trauma service at our institution with drainage from his neck wound and increasing jaw pain. (Fig. 3). An interval CT scan showed a retained bullet fragment that had migrated to the superficial aspect of the right lateral neck (Fig. 4). It was decided to proceed with removal of this foreign body as well as exploration of the neck wound.

The patient had a previous area of purulence and apparent protrusion of a metallic fragment noted along a pre-existing surgical scar line in the right neck (circled in red). A 3-cm incision was made through the existing scar with a #15 scalpel blade. Exploration of the site showed evidence of a retained bullet fragment measuring approximately 1/2 inch × 3/4 inch. The exploration continued and extended to the level of the sternocleidomastoid muscle, with no further identification of additional retained GSW fragments or other foreign body. GSW, gunshot wounds.
Intraoperative CT imaging showing a protruding bullet fragment in the right neck superficial to the sternocleidomastoid muscle without evidence of an adjacent fluid collection or vascular injury. CT, computed tomography.
The patient was brought to the operating room were an adequate level of anesthesia was obtained via oral endotracheal intubation and inhalational anesthesia. The patient had a previous area of purulence and apparent protrusion of a metallic fragment noted along a pre-existing surgical scar line in the right neck. An incision was made through the existing scar, and exploration of the site showed evidence of a retained bullet fragment measuring ∼0.5 × 0.75 inches. The exploration continued and extended to the level of the sternocleidomastoid muscle, with no further identification of additional retained fragments or other foreign bodies.
Treatment Algorithm
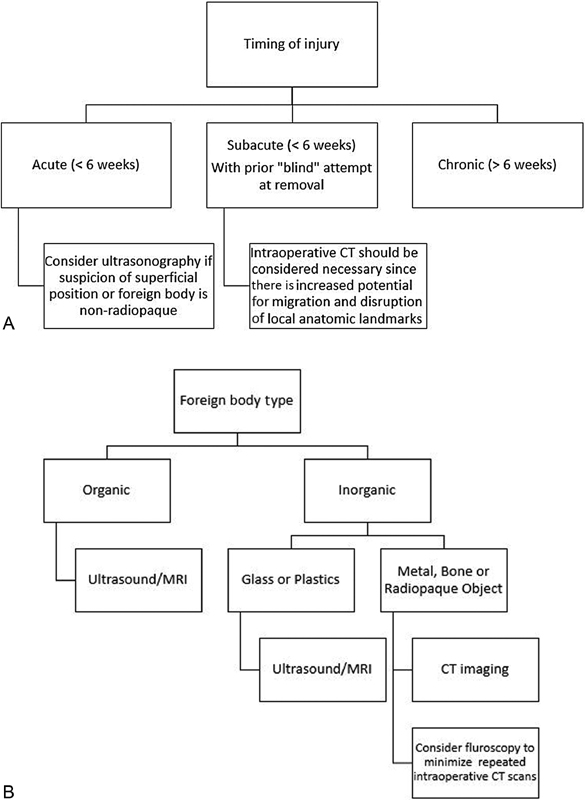
Fig. 5A, B shows a generalized algorithm for foreign body removal. Generally, this should be performed under general anesthesia. With regards to the chronicity of the injury, patients should be classified into three strata: acute (< 6 weeks), subacute (< 6 weeks, with a history of previous “blind” retrieval attempt), and chronic (> 6 weeks). Removal of foreign bodies in the acute setting must be undertaken with extreme caution. In this timeframe, there is minimal scar tissue present around the foreign body, resulting in an increased risk for displacement during the retrieval process. The use of ultrasonography may be considered in these patients if the injury is superficial or the foreign body is organic in nature. Subacute injuries provide a more challenging dilemma for the craniomaxillofacial surgeon. Previous blind retrieval attempts can lead to the disruption of normal anatomic landmarks and migration of the foreign body outside the normal fascial planes. The risk of further iatrogenic injury is high in these patients, so the use of intraoperative computer-based surgical navigation is necessary for accurate localization of the foreign body with minimal dissection. Chronic injuries also necessitate the use of intraoperative CT and surgical navigation, since the presence of scar tissue can distort normal anatomy and prove to be a significant impediment during meticulous dissection. It is worth noting that fluoroscopy can be used as an adjunctive measure for localization of a radiopaque foreign body if there are concerns about excessive radiation exposure to the patient secondary to repeated intraoperative CT scans.
(
Conclusion
Foreign body penetration and migration in the head and neck is particularly concerning due to the increased risk of damage to the great vessels and nerves. In addition, migration often cannot be easily predicted as objects may travel outside the confines of anatomic fascial planes. Although patients may be asymptomatic for years prior to presentation, timely removal of foreign bodies is ideal to preclude injury to important vascular and neurological structures as well as to prevent the development of recurrent infections and foreign body reactions. Current literature is rife with diverse case series outlining unusual patient presentations and creative surgical interventions for foreign bodies in the head and neck. Given the challenging anatomy of the region as well as the heterogeneity of patient presentations, it is important for the craniomaxillofacial surgeon to utilize multidisciplinary resources and appropriate diagnostic tools when assuming the care of these patients.
Footnotes
None.