
Abstract
Intracapsular condylar fractures may account for 65% of all condylar fractures. This diversity of classifications makes epidemiological data collection challenging. Historically, intracapsular condylar fractures were treated in a closed or conservative manner, without open surgery and fixation of the bone fragments. Closed treatment has been described with acceptable outcomes without the risk of complications associated with the surgical treatment, that is, infection, damage to the facial nerve, and unaesthetic extra-oral scar. Recently, studies reporting the surgical treatment of condylar head fractures have reported better results regarding mandibular functional aspects, dental, and aesthetic results. It is also suggested that the repositioning of the articular disc during the surgical procedure, could prevent the consequences of its displacement in possible temporomandibular joint dysfunctions. The objective of this study is to report a clinical case of intracapsular condylar head fracture with open treatment, using lag screw fixation according to AO/ASSIF (Arbeitsgemeinschaft für Osteosynthesefragen/Association for the Study of Internal Fixation) protocols and recommendations.
Mandibular fractures are among the most common facial fractures. Regarding only mandibular fractures, the incidence of condylar fractures may vary, reaching up to 52% in some studies.1 Several proposals for the classification of condylar fractures have already been proposed in the literature.2 This diversity of classifications makes epidemiological data collection challenging.2 The classification proposed by Loukota et al in 2010 for condylar head fractures should be mentioned. Accordingly to the authors, three types of condylar head fracture patterns may be found and classified as: type A, when the fracture line runs through the medial part of the condylar head; type B, when the fracture line runs through the lateral part of the condylar head; and type C, when the fracture line is near to the attachment of the lateral capsule.3 According to previous studies, intracapsular condylar fractures may account for 65% of all condylar fractures.12
Following the concepts and philosophy of the AO/ASIF treatment, the decision for the surgical treatment of condylar fractures should be grounded on specific factors, such as the patient's medical condition and their compliance with the treatment, the presence of functional limitations, such as malocclusion or mouth opening limitation, other associated facial fractures, the degree of the displacement of the condylar head, and the bone fragments fractured, as well as dentition status.4 Two recent systematic literature reviews point to an improvement in mandibular functional movements (protrusion and laterality) and maximum interincisal opening when the surgical treatment is adopted, compared with the closed treatment.56 It is also suggested that there is a significant difference favoring the adoption of the surgical or open treatment for postoperative temporomandibular joint (TMJ) pain and for facial symmetry during the mouth opening.6
In cases of intracapsular or condylar head fractures, the rupture of the joint capsule is frequent, and in some of these cases, the fracture line may divide the condylar head sagitally.4 Recent studies on the treatment of condylar head fractures have suggested that better results are achieved when the surgical procedure is used.2378 A prospective long-term follow-up study by Kolk and Neff evaluating vertical height, disc mobility, and mandibular movements after surgical treatment of condylar head fractures treated with small-fragment positional screws found stable and good functional results in all the mentioned items evaluated.9 Surgical treatment of condylar head fractures allows early functional recovery and mandibular movement. Moreover, compared with the closed or “conservative” treatment, it avoids extensive condylar remodeling, loss of posterior facial height, and occlusal disturbances.27 It also allows repositioning of the articular disc during the surgical procedure, preventing the consequences of its displacement in possible temporomandibular joint dysfunctions, such as osteoarthritis and ankylosis.291011 This is relevant because studies show that intracapsular fractures present a higher incidence of articular disc displacement when compared with the condylar neck or subcondylar fractures.101112
The objective of this study is to report a clinical case of intracapsular condylar head fracture with open treatment, using lag screw fixation according to AO/ASIF protocols, and recommendations.
Case Report
An 18-year-old male patient sought the Maxillofacial Surgery Department after suffering a cycling accident. The individual was projected over the bicycle which caused a direct trauma in the region of the mandibular symphysis.
The patient complained of pain during mandibular movements, masticatory difficulties, and mouth opening limitation (Fig. 1). He also claimed that his teeth were not correctly aligned. Clinical intra- and extraevaluation allowed the detection of typical signs of condylar fractures. The patient presented laceration in the soft tissues of the mandibular symphysis region, as well as mouth opening deviation to the right side (the fractured one) during the opening (Fig. 2). He also presented an occlusal alteration characterized by an open bite on the left side (unaffected) and a slight decrease in the posterior facial height, caused by a reduction in the mandibular posterior ramus on the right side (Fig. 3). The preoperative cone bean tomographic examination indicated a fracture of the condylar head with a sagittal fracture tract and medial displacement of the fractured segment (Fig. 4A-C).

Maximum interincisal opening. Limitation of the mouth opening due to the condylar fracture.

Mouth opening deviation to the fracture side.

Left side of the occlusion with a slight open bite as a consequence of the reduction or the height of the mandibular ramus on the right side.

(
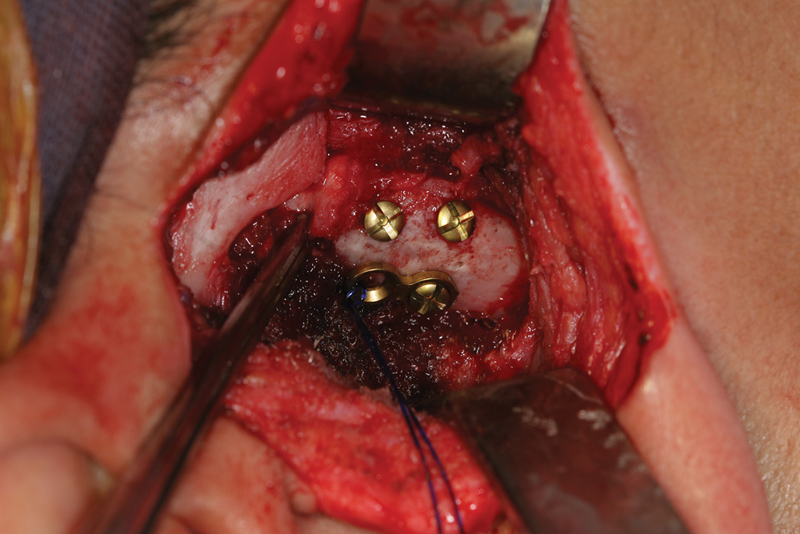
Seven days after the patient's first visit and 15 days after the incident, the surgery for reduction and fixation of the condylar fracture was planned and performed. Although lag screw fixation has been poorly described in the literature, following a suggestion of protocol for fixation of intracapsular fractures by AO/CMF, it may be the best or only way to stabilize the fractured segment, especially the fractures with a sagittal component of the mandibular head or medial displacement of the fractured segment. The suggestion for this fixation method is because there is usually no sufficient space to reduce and stabilize the bone fragment using plates and screws, in this type of fracture. One important maneuver to aid in the capture and reduction of the fractured bone fragment is the mandibular downward traction, which increases the available space in the articular cavity. This maneuver can be performed using a screw in the mandibular ramus, more inferiorly, near the region of the mandible angle and with a steel wire attached to it, so as to draw the mandible downward (Fig. 5). After the reduction of the medially dislocated bone fragment, it was stabilized using 2 12 mm screws according to the lag screw technique. This procedure approximated the performed bone reduction, stabilizing the fractured segment. After the reduction and fixation of the condylar head fracture, the articular disc was repositioned back to its anatomical position and stabilized with a Prolene 2.0 suture (Ethicon, Jonhson and Jonhson, USA) attached to a mini-plate installed onto the mandibular posterior ramus region (Figs. 6 and 7). This technique allowed the disc to be stabilized and held anatomically in a satisfactory way.

Mandibular downward traction with a screw and steel wire. White arrows show the proposed AO/ASIF maneuver.
Capture and reduction of the articular disc to its anatomical position.

Stabilization of the articular disc with a 2.0 Prolene sutured in a 2 hole 1.5 mm plate.
The immediate postoperative tomographic image confirmed the adequate reduction and fixation of the fractured segment (Fig. 8A-C). The patient was kept in mild postoperative physical therapy during the first postoperative weeks. During the 30-day postoperative follow-up, the patient did not report any painful symptomatology and showed improvement in symmetry and maximum mouth opening (Figs. 9 and 10). The dental occlusion was functionally restored (Fig. 11A, B) and the postoperative scar of the preauricular approach presented satisfactory aesthetics (Fig. 12). Over the first postoperative weeks, the patient showed mild weakness of the facial nerve, which was normalized entirely later (Fig. 13 A, B).


Postoperative mouth opening with a symmetric mandibular movement.

The 30-day postoperative maximum interincisal opening.

Left occlusion restablised after surgery.

Good aesthethic results with 30 days after surgery for the preauricular approuach.

(
Discussion
There is still some confusion in the literature in regard to the best treatment of condylar fractures.6 This problem is aggravated by the various classifications of existing condylar fractures. The lack of standardization makes it difficult to obtain reliable and accurate data on the treatment of this type of fracture. This is also the result when systematic reviews are performed on what would be the best treatment and results for condylar fractures, if surgical or nonsurgical treatments, without an ultimate consensus.613 In 2014, the AOCMF (Arbeitsgemeinschaft für Osteosynthesefragen CranioMaxillofacial) level 3 classification system for condylar process fractures was proposed. It is expected that with a protocol on the diagnosis process, a more accurate evaluation of the condylar process fractures will be better understood and compared among different centers and studies published.14 The decision for the surgical treatment of condylar fractures should be based on factors, such as the patient's individual profile (systemic, dental, and psychosocial factors), functional limitation (mastication, mouth opening, and malocclusion), concomitant fractures (e.g., associated mandibular or middle-third fractures), where it is necessary to reestablish a reliable reference, such as the posterior facial height and the degree of condylar displacement.2 456 Conservative treatment is still widely used for condylar fractures and should always be the first option for pediatric patients, nondisplaced fractures, or to those with small functional alterations.2 45613
When dealing exclusively of intracapsular fractures, the recommendations are less precise or not clarified entirely in the literature, and many authors suggest that the treatment of this type of fracture is performed conservatively.11315 Closed treatment is associated with acceptable results without some risks associated with surgical treatment, such as postoperative infection, increased risk of damage to the facial nerve, unaesthetic facial scar, and possibility of osteoarthosis and bone resorption due to the open treatment.1316
However, there has been an increase in the number of studies reporting and suggesting advantages for the surgical treatment of condylar head fractures.23 4567891011 Condylar head fractures are often associated with displacement of the articular disc, as well as rupture of the capsule and ligaments of the temporomandibular joint. Several studies suggest and confirm the importance of surgical treatment for this type of fracture, as it allows the repositioning of the articular disc back to its habitual anatomical position, which, in turn, can prevent or reduce the chances of internal TMJ disorders, osteoarthrosis, and even fibrous or bone TMJ ankylosis.27101117 Some literature reviews and clinical studies point to a lower risk of condylar deformation, loss of height or reduction of the mandibular ramus, and facial asymmetry, improvement of mouth opening and protrusive and laterotrusive mandibular movements, and a lower incidence of malocclusion, pain, and TMJ dysfunction in short- and long-postoperative period.25671011 Kolk and Neff, evaluating the results of surgical treatment of mandibular condylar head fractures with small-fragment positional-screw osteosynthesis in a long-term period (5 years), found stable and excellent functional results. The major goals evaluated (vertical height, prevention of occlusal disorders, physiological functional of the disc, and condyle and pain-free results) were all achieved, and comparing with the group treated surgically with small microplates, the results with positional screws were better.8 On the other hand, the most significant complications reported for the surgical treatment of intracapsular fractures are the facial nerve injury during extra-oral surgical approaches and the nonaesthetic scar which are not present in the conservative treatment. A recent systematic review evaluating the risk of facial nerve weakness after the surgical management of mandibular condylar process fractures, found that transient weakness of the nerve can vary from 4.3 to 18.7%, depending if the nerve is encountered or not during the surgical approach.18 Furthermore, some authors question the real need for surgical treatment of this type of fracture, when previous (and less recent) studies point to positive results with the adoption of conservative treatment.1 413
The decision to adopt surgical treatment in our case is due to the individual characteristics presented by the patient and the literature background supporting the surgical treatment of intracapsular fractures. The advantages of surgical treatment, especially regarding the possibility of repositioning of the articular disc back to its anatomical position, lowering the risk of future internal TMJ derangements cannot be ignored. In the last international symposium for condylar fracture osteosynthesis realized in Marseille, France, in 2012, it was suggested that the surgical treatment with osteosynthesis reduction and internal fixation of condylar head fractures is highly recommended. Although it was mentioned by this position paper published in 2014 that this recommendation requires further investigations.19 For all the others condylar fractures (condylar base and neck fractures), surgical treatment may now be considered as the gold standard.19 In this case presented, patient showed occlusal alteration with an slight open bite on the opposite side to the fractured side, posterior right facial height reduction, and pain and limitation on mouth opening, all of which were crucial factors for us to go on with the surgical treatment plan. In addition, the most important factor is that the patient favored the surgical treatment when both options (surgical and conservative) were presented to him. Furthermore, the fact that he was young, cooperative, had no missing teeth and did not present any systemic health alterations, added up positively upon our decision to perform a surgical treatment. The reduction and fixation of this type of fracture are challenging. Following the guidelines of the AO/CMF handbook for intracapsular condylar fractures, we used the lag screw technique to finalize the approximation of the bone fragment reduced and its proper stabilization, inserting two screws in the affected region, as there was no other way to fix the fractured bone segments, due to the lack of room to perform any other type of fixation method. The inferior traction of the mandible with the aid of a wire attached to a screw in the region of the mandibular ramus was another extremely valuable maneuver during surgery. It increased the articular space, facilitating our visualization when searching for the medially displaced fractured bone segment, as well as the reduction and maintenance of its position, while the lag screw fixation was performed. It is worth mentioning that the articular disc was captured and held in place with a 2.0 Prolene suture attached to a two-hole plate, stabilized and fixed at the posterior border of the mandibular ramus. In developing countries, such as Brazil, not all of the public health service hospitals have equipment, such as TMJ anchors, due to its associated cost.
Conclusion
Although complications associated with surgical treatment are reported, this choice for the treatment for intracapsular fractures seems to be a reasonable option when the patient shows functional, occlusal, or aesthetic alterations, especially when having dental and systemic characteristics that do not restrict the adoption of the surgical treatment. Clinical and radiological studies point to the positive functional results of the surgical treatment of intracapsular fractures associated with the anatomical repositioning of the articular disc, which is often displaced, avoiding TMJ dysfunctions and ankylosis. The use of the surgical maneuvers proposed by AO/ASIF was paramount and of excellent value for the resolution of the clinical case discussed herein.
Footnotes
None declared.