
Abstract
Until recently, three-dimensional (3D) printing/additive manufacturing has not been used extensively to create medical devices intended for actual clinical use, primarily on patient safety and regulatory grounds. However, in recent years there have been advances in materials, printers, and experience, leading to increased clinical use. The aim of this study was to perform a structured systematic review of 3D-printed medical devices used directly in patient treatment. A search of 13 databases was performed to identify studies of 3D-printed medical devices, detailing fabrication technology and materials employed, clinical application, and clinical outcome. One hundred and ten papers describing one hundred and forty medical devices were identified and analyzed. A considerable increase was identified in the use of 3D printing to produce medical devices directly for clinical use in the past 3 years. This is dominated by printing of patient-specific implants and surgical guides for use in orthopedics and orthopedic oncology, but there is a trend of increased use across other clinical specialties. The prevailing material/3D-printing technology used were titanium alloy/electron beam melting for implants, and polyamide/selective laser sintering or polylactic acid/fused deposition modeling for surgical guides and instruments. A detailed analysis across medical applications by technology and materials is provided, as well as a commentary regarding regulatory aspects. In general, there is growing familiarity with, and acceptance of, 3D printing in clinical use.
Introduction
Three-dimensional (3D) printing, also referred to as additive manufacturing (AM), has been the focus of considerable interest in the field of medical applications over the past decade. 1 Such technology has been used to produce medical instruments for diagnostics, surgical instruments and guides, anatomical models for surgical planning, education and training, implants, prostheses and orthoses, tissue engineering scaffolds, tissue models, and pharmaceuticals.2–4 Initially, custom 3D printing was used primarily for education, but a remarkable growth in 3D printing of medical devices used in the direct treatment of patients is evident from published reports.1,5 SmarTech Publishing estimates that the production of 3D-printed implantable devices will experience a 29% compound annual growth through 2026. 4
In the production of medical devices, 3D printing offers several advantages over traditional subtractive manufacturing techniques. Most notable is the possibility of individual patient-specific/personalized treatment, which is especially advantageous in the context of rare diseases or uncommon anatomy. 3 3D printing also allows for high geometrical and structural complexity of designs with little influence on part-production time 6 ; cost-effective small-scale, on-demand fabrication of highly specific, customized products due to favorable unit production costs and short product lead time6–9 ; and the possibility of in-house or localized production of medical devices and fabrication in remote areas subject to supply chain limitations. 10
However, there are evident risks associated with 3D printing, including, but not limited to, potential adverse events related to bioavailability and bioactivity of component materials and microbiology safety concerns with respect to 3D-printed devices for placement inside the body. Therefore, regulatory issues regarding on-demand manufacturing of patient-specific 3D-printed medical devices are complex, challenging, and are still evolving.1,11 In 2017, the Food and Drug Administration (FDA) published draft guidelines for 3D printing of medical instruments with specifications of design, manufacturing, and device testing. 12 Zhou and Bhaduri 4 published a list of medical-device-related products that had recently been granted FDA approval.
A 2019 review of 71 articles by Culmone et al. 3 focused on 3D-printed medical instruments for examining or treating patients. However, that study excluded, among others, prostheses, orthoses and surgical guides, and medical devices were meant to stay in the body. The review also included devices in the early prototyping phase that were not tested on live patients, and were thus not necessarily subjected to requirements regarding postprocessing for removal of debris and sterilization. 3
The aim of the present study was to perform a systematic review of medical devices, as defined by the European Medical Device Regulation (EU) 2017/745 (MDR), 13 that were produced by means of 3D printing, and employed for the direct treatment of medical conditions in human patients. Specifically of interest were the device types and fields of application, 3D-printing technology and materials employed, and the clinical outcomes of device use. The review also captures references made to particular regulatory aspects of 3D printing in the selected studies.
Materials and Methods
Literature search and study selection
A systematic literature search was performed in August 2020 of the following databases: Cochrane, EBSCOhost (including Academic Search Complete, Business Source Complete, CINAHL Complete, EconLit with Full Text, MEDLINE, OmniFile Full Text Mega, and Regional Business News), EMBASE, PubMed, Science Direct, Scopus, and Web of Science.
Of interest were all article that included the following keywords: “3D print*” or “3D-print*” or “dimensional print*” or “additive manufacturer*” in the title, and “medical device*” or “instrument*”, and “patient*” or “subject*” or “case report” or “case study” in the title, abstract or keywords. If necessary, the search string was adapted to meet the search options of the specific databases. The study selection was limited to full scientific articles in the English language that described 3D printing of medical devices, and use of these devices on living human patients.
Studies performed on healthy volunteers, animals and in vitro, as well as those where 3D printing was only employed for the production of tools/molds for medical device fabrication (i.e., indirect AM) were excluded. Further excluded were reviews and overviews, papers regarding directives, regulations, and economic aspects of the use of 3D printing, studies involving anatomical models for surgical planning or training/education, 3D printing of pharmaceuticals, and descriptions of new 3D-printing materials, material properties, and physical properties of 3D-printed parts. Due to the unique technological, clinical, ethical, and regulatory considerations, studies of implants produced by means of bioprinting and organ/tissue engineering were also excluded.
The review protocol was designed according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines 14 (Fig. 1). T.K. performed the searches, and A.S. confirmed search outcomes. L.W.O.S. resolved any disagreement between T.K. and A.S.
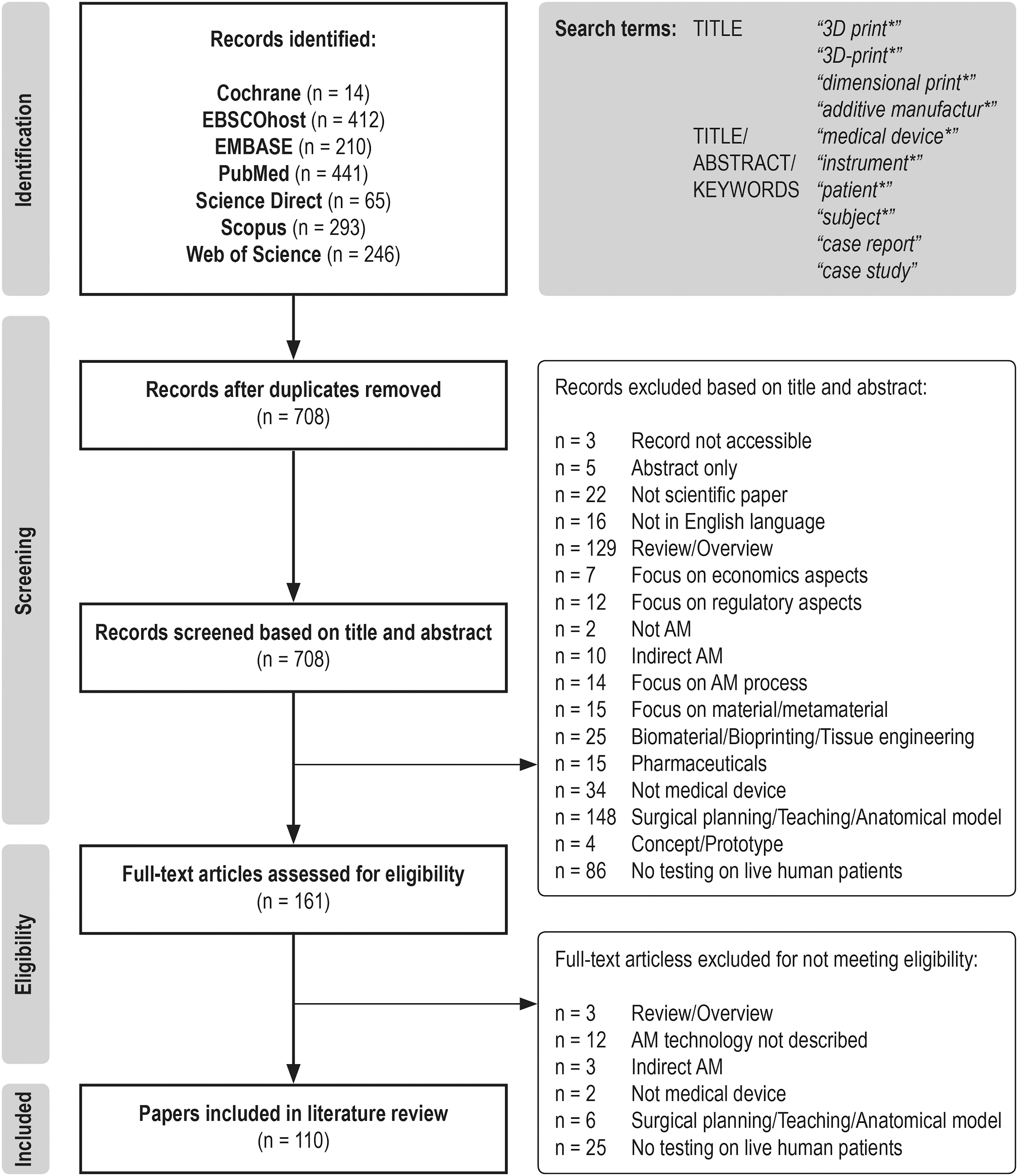
PRISMA flow diagram of literature search and study selection. PRISMA, preferred reporting items for systematic reviews and meta-analyses. Template adopted from Moher et al. 14
Data extraction and synthesis
The following data were extracted from the selected studies: (1) medical-device description and field of application, (2) 3D-printing technology and materials used for device fabrication, (3) number, sex, age, and medical condition(s) of patients treated, and (4) clinical procedure and outcome of device use. The details of regulatory approval of the devices were extracted if included in the studies. In cases where information on the 3D-printing technology used was incomplete, but sufficient detail was provided (e.g., 3D-printer name, name of the company that produced the device), the missing information was obtained online, or from the corresponding authors of the papers.
Results
Overview of research activity regarding the use of 3D printing for medical device fabrication
One hundred and ten relevant papers were identified regarding direct 3D printing of medical devices and their use in treatment of patients. In 4 papers,15–18 several individual studies were described, and in 18 papers, more than one type of medical device was fabricated; one study 19 was included in three different papers, and one 20 in two different papers. Thus, a total of 119 studies detailing 140 medical devices were reviewed.
The majority of studies were published in 2018 (36), followed by 2020 (29 to date) and 2019 (27). There were considerably fewer studies before 2018 that met the inclusion criteria (Fig. 2).

Studies of three-dimensional printed medical device use on patients by publication year.
Fields of application and medical conditions addressed by direct 3D printing of medical devices
The use of 3D printing for medical device fabrication was most prevalent in surgery, especially in orthopedics (36%) and orthopedic oncology (32%), followed by maxillofacial surgery (6%), neurosurgery (4%), and plastic surgery (1%). Among nonsurgical applications, 3D printing was used in oncology (7%), followed by orthotics (4%), immobilization (2%), and prosthetics (1%). Single cases of 3D printing were reported in abdominal, thoracic, and dental surgery, anesthesiology, gastroenterology, infectology, ophthalmology, and orthodontics (Fig. 3).
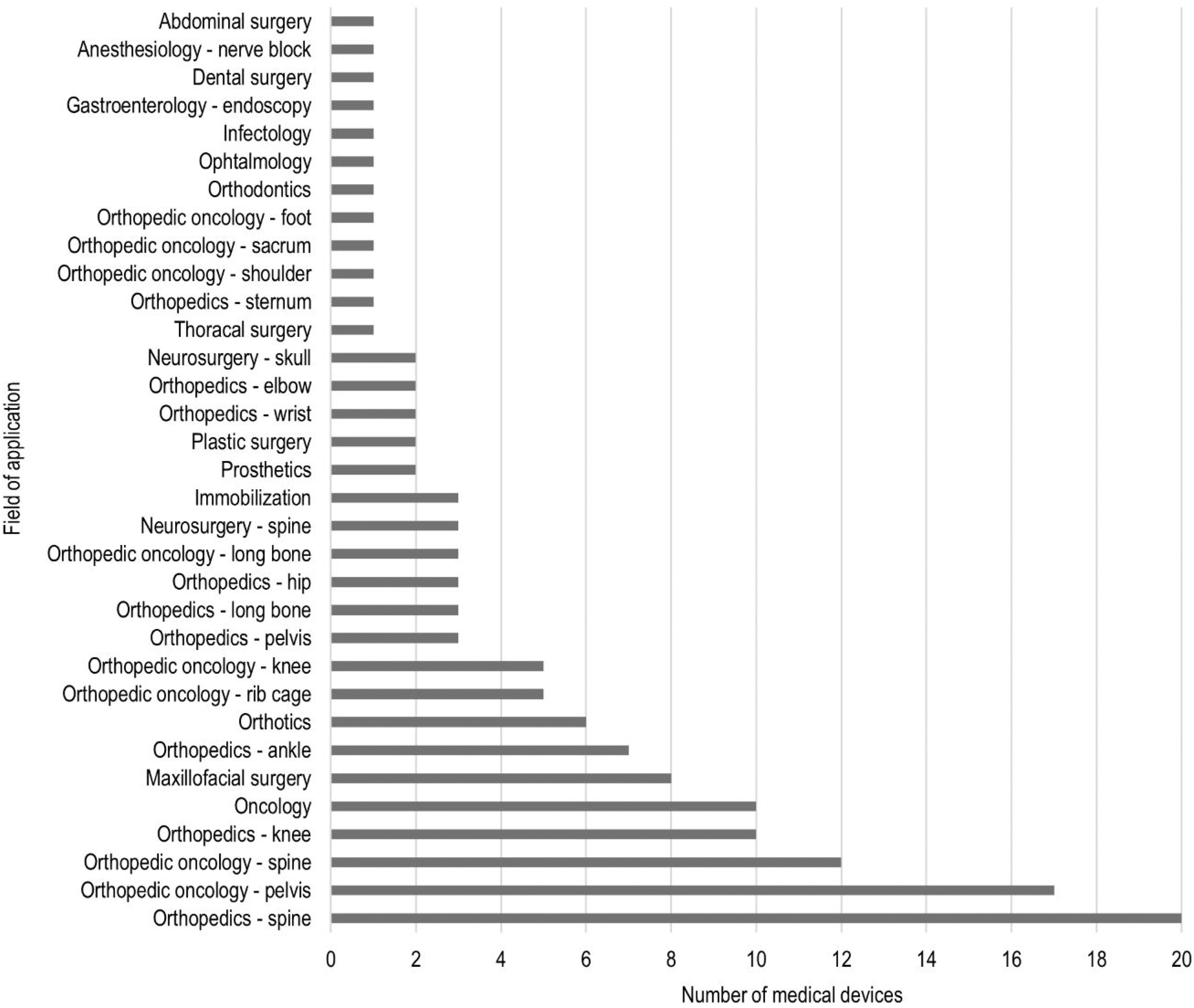
Number of studies by medical application.
The majority of participants treated with 3D-printed medical devices were orthopedic patients, predominantly undergoing spinal, knee, or pelvic/hip surgery. Patients with spinal complaints presented with congenital or degenerative conditions causing spinal instability, neurological symptoms, pain, fractures, or deformities. At the knee, patients suffered from end-stage osteoarthritis, rheumatoid arthritis, post-traumatic and postoperative osteoarthrosis; and at the pelvis/hip from pain or instability due to fracture, endoprosthesis loosening, or bone defects. Other orthopedic diagnoses were limb deformity, traumatic fracture, fragment nonunion, severe arthritis or instrument failure after fracture reduction, epiphysiodesis, avascular necrosis, femoral head osteonecrosis, and osteomyelitis.
The second most frequent use of 3D printing was in relation to pelvic/sacral and spinal tumors. Other diagnoses in orthopedic oncology were primary or secondary sternum/rib, upper and lower limb tumors. In oncology, the patients presented with small peripheral lung nodules; carcinoma or mycosis fungoides of the head; and pancreatic, liver, or breast cancer. Airway collapse due to tracheobronchomalacia was prevented in infant patients, as were complications after hypotonic perioral musculature and macroglossia. Abdominal surgery was performed to plug an enteroatmospheric fistula. In gastroenterology, endoscopic treatment was facilitated for gastric and esophageal conditions.
In maxillofacial surgery, the conditions treated were tumor-related bone defects and osteoarthritis of temporomandibular joints. In dental surgery, agenesis of mandibular premolars was treated in teenage patients. In neurosurgery, patients were treated for hydrocephalus, spinal compression, and neurogenic constipation. Heminasal deformities and unilateral microtia were treated in plastic surgery.
Immobilization was performed on patients with traumatic wrist and lower-limb fractures. Orthoses were used to alleviate plantar fasciitis, bilateral flatfoot, and impairment of hand/wrist function due to stroke or spinal cord injury. Prostheses were made for patients with traumatic index finger amputation, and for a patient after rhinectomy. In anesthesiology, a supraclavicular block was facilitated on a patient with morbid obesity. Different conditions of the cornea were treated with keratoplasty in ophthalmology, and a nasal swab was used to diagnose SARS-CoV-2 infection. For detailed information on participants' medical conditions, see Tables 1–3.
Reviewed Studies Detailing Other Three-Dimensional-Printed Medical Devices
Reviewed Studies Detailing Three-Dimensional-Printed Implantable Devices
3D, three-dimensional; ABS, acrylonitrile butadiene styrene; Cr-Co-Mo, cobalt chromium molybdenum; DLP, digital light processing; DMLS, direct metal laser sintering; EBM, electron beam melting; EVA, ethylene vinyl acetate; FDM, fused deposition modeling; MJ, material jetting; N/A, information not provided; PA, polyamide (nylon); PCL, polycaprolactone; PEKK, polyetherketoneketone; PETG, polyethylene terephthalate glycol; PLA, polylactic acid; PMMA, polymethyl methacrylate; PPSF, polyphenylsulfone; SLA, stereolithography; SLM, selective laser melting; SLS, selective laser sintering; TES, total en bloc sacrectomy; TPU, thermoplastic polyurethane; yrs, years.
Technology employed in direct 3D printing of medical devices
In the reviewed literature, the most frequently used 3D-printing processes for medical device fabrication were electron beam melting (EBM; 29) and fused deposition modeling (FDM; 29), followed by selective laser sintering (SLS; 13), stereolithography (SLA; 9), selective laser melting (SLM; 10), and material jetting (MJ; 9); direct metal laser sintering and digital light processing (DLP) were only used twice. In 35 cases, the 3D-printing process was not specified.
The most common materials for medical devices were titanium/titanium alloy (including titanium/PoreStar composite and titanium coating; 55), polylactic acid (PLA; including PLA/polyhydroxyalkanoate [PHA] and PLACTIVE™; 19), polyamide (PA; 17), and photosensitive resin (including Dental SG and Somos® XC11122; 13). Other less used materials include acrylonitrile butadiene styrene (ABS), Acrylate resin, Agilus-60, cobalt chromium molybdenum (Cr-Co-Mo) alloy, ethylene vinyl acetate, high impact polystyrene (HIPS), MED610, polycaprolactone (PCL), polyetherketoneketone (PEKK), polyethylene terephthalate glycol (PETG), polymethyl methacrylate (PMMA), polyphenylsulfone, silicone, TangoPlus, tantalum, thermoplastic polyurethane (TPU; including NinjaFlex), and ULTEM™ 1010. In 11 cases, the material was not specified.
Overview of 3D-printed medical devices tested on patients
In the reviewed studies, 3D printing was employed to produce 57 implantable devices, 56 surgical guides, 6 radiotherapy boluses, 7 orthoses, 3 surgical templates, 3 surgical instruments, 3 immobilization devices, and 2 prostheses. A nasal swab, lenticule storage glide, and an enteral stent were also manufactured (Fig. 4). Several studies reported the use of 3D-printed anatomical models for presurgical planning, but these are beyond the scope of the present review.

Types of medical devices described in the reviewed studies.
The data extracted from the reviewed studies are provided in Table 1 for implantable devices, see Table 2 for guides, and Table 3 for other medical devices.
Reviewed Studies Detailing Three-Dimensional-Printed Cutting, Drill, and Navigation Guides
BMI, body mass index; HIPS, high impact polystyrene.
Patient-specific surgical guides and implants were the most often produced devices, with the largest number of implants in orthopedic oncology (33), and surgical guides in orthopedics (31). With the exception of a vertebral-body endoprosthesis (PEKK printed by SLS), an airway splint (PCL printed by SLS), an ankle prosthesis (Cr-Co-Mo), and an implant for pelvic reconstruction (tantalum), all implantable devices were printed in titanium or titanium alloy by using either EBM (29) or SLM (8). In two cases,20,21 the titanium endoprosthesis was coated with porous High-density Polyethylene (PoreStar) for lightweight and structural enhancement. In 16 cases, the 3D-printing process was not reported.
Virtually all titanium endoprostheses were designed to provide a roughened or porous surface at the interface with the bone to improve the chance of bone ingrowth and enhanced implant stability. In seven cases, the implants had a cage construction filled with allogenic bone graft to further facilitate osseointegration.
Surgical guides were most often manufactured using either PA (15; 9 with SLS), PLA (12; 10 with FDM), photosensitive resin (including Dental SG, Somos XC11122, Med610, and ULTEM 1010; 6 with SLA, 4 with MJ, 1 with DLP, 1 technology not specified), PETG with FDM (2), and titanium (2; 1 with SLM). In single cases, ABS P430, acrylate resin, and HIPS were printed with FDM, and PMMA with a 3D-printing technology not specified.
Of the other devices in contact with internal tissues, surgical instruments were manufactured by using PA with SLS, silicone with MJ, or photosensitive resin with unspecified 3D-printing technology; templates for auricular reconstruction were printed by using PLA with FDM, for nose contouring using MED610 with MJ, and a tooth replica using titanium alloy with SLM; an enteral stent was printed by using TPU with FDM, and a lenticule storage glide by using an unspecified material with MJ.
Most devices in contact with the face were made of flexible, elastomeric materials to ensure patients' comfort. Radiotherapy boluses were printed in TPU (NinjaFlex) with FDM, or Agilus-60 with MJ, and a nasal prosthesis in TangoPlus with MJ. Two other boluses were fabricated by using PLA with FDM, and one using PLA/PHA with FDM. A nasal swab was printed in PA with SLS. Immobilization devices, limb orthoses, and prostheses were manufactured from polymer-based materials by using DLP, FDM, or SLA. Materials and 3D-printing technology used for the production of the reviewed medical devices are presented in Table 4.
Three-Dimensional-Printing Technology and Materials by Medical Device Type
The current authors are unfamiliar with these combinations of materials and technologies.
In the field of facial prosthetics, 3D printing was primarily used for fabrication of molds, as opposed to direct manufacturing of prostheses, due to the poor mechanical properties of the available 3D-printing materials (e.g., TangoPlus) compared with the benchmark silicone. 120
Implantable airway splints were manufactured by using PCL, a biocompatible polyester that is bioresorbable after 2–3 years.19,22 The choice of material was of key importance in this procedure, as the conformational change due to material degradation over time in combination with an open cylindrical design allowed for accommodation of airway growth in infant patients who received the splint.
Clinical procedures and outcomes involving 3D-printed medical devices
All medical devices included in this review were used to directly treat patients. The number of participants in the studies ranged from 1 to 496 (1–16 for female only, 1–5 for male only, and 2–496 for both sexes). Forty-two studies were performed on single patients.
In orthopedics, orthopedic oncology, and maxillofacial surgery, the patients were treated with tumor/bone resection by using personalized surgical guides, and reconstruction of bone deficits and/or deformities with custom osteosynthetic material or endoprostheses. In all cases of orthopedic implants, satisfactory osseointegration and precise compatibility with the target bone surface, or off-the-shelf implantable devices was observed. It was noted that maximizing the contact area between the implant and bone improves stability and lessens postoperative pain. 44
Additively-manufactured devices were also used for invasive and noninvasive immobilization of extremities in the treatment of bone fractures. In neurosurgery, 3D-printed instruments were used to facilitate the insertion of therapeutic devices to target location (i.e., ventricular catheter for hydrocephalus treatment, puncture for brainstem hematoma drainage, electrodes for sacral neuromodulation), and to localize the point of skin incision in lumbar microsurgery. Tailored endoscopic caps increased the ease and decreased the duration of endoscopic procedures. In abdominal surgery, an enteral stent was used to plug an enteroatmospheric fistula. In thoracic surgery, airway splints relieved the (extra)pulmonary complications due to tracheobronchomalacia. In oncology, patient-specific navigational guides were used to quickly and safely localize small percutaneous lung nodules in cancer screening.
Esthetically superior outcomes and reduced operative times were achieved with template use in plastic surgery for heminasal reconstruction and auricle reconstruction. Artificial tooth sockets were successfully prepared with the use of donor tooth replicas before autotransplantation in dental surgery, resulting in decreased extraalveolar and procedural times. Reduced surgical time and eliminated complications related to tissue preparation were also noted with the use of a smart storage glide for preservation, transport, and insertion of lenticules in keratoplasty. Additively manufactured nasal swabs were equally successful in diagnosing COVID-19 infections as conventional swabs, while being preferred by the majority of participants.
All invasive devices and the nasal swab were sterilized before use, either chemically (ethylene oxide, hydrogen peroxide), with low-temperature plasma sterilization, moist heat (autoclave), or cobalt-60 irradiation.
In general, invasive medical procedures using 3D-printed devices were successfully performed with favorable short- and long-term outcomes. For implantable devices, very few cases of failure (e.g., fracture, loosening, movement, subsidence) were reported up to 108 months postsurgery.
However, specific complications were reported in 15 studies. These included 1 case (of 51) of sacroiliac-joint-fusion implant malposition 38 ; 2 cases (of 6) of subsidence of patient-specific PEKK prostheses for vertebral-body replacement, possibly due to mispositioning of the prosthesis at implantation 28 ; 1 (of 13) clinically relevant vertebral-body implant subsidence into the adjacent vertebral body. 31
Also reported were 2 cases (of 11) of hip dislocation with patient-specific hemipelvic prostheses 54 ; 2 cases (of 12) of unsatisfactory knee range of movement with the use of intercalary prostheses for joint-preserving intercalary tumor resection 58 ; 3 cases (of 10) of sacral endoprosthesis failure due to screw breakage 46 ; 1 (of 9) aMace® Acetabular Revision System failure 49 ; 4 (of 568) titanium-coated knee baseplate failures due to aseptic loosening 59 ; significantly higher rates of loosening of a modified anatomic template for pelvic reconstruction compared with the conventional approach 51 ; 1 (of 15) early deep infection and one nonunion with patient-specific ankle implant cages 63 ; limited shoulder and elbow range of motion with total humeral endoprosthesis, a dislocation of partial humerus endoprosthesis, and a distal radius implant dislocation during growth in a teenage patient; 18 and undercorrection in corrective osteotomies of long bones with patient-specific cutting and drill guides. 68
In 15 infants receiving airway splints, one death was possibly associated with splint displacement. 22 One (of 188) resection jig error caused a larger resection than planned, 69 and 1 (of 10) significant deviation from the planned screw trajectory was noted due to a drill guide being split by rough handling. 83
Regarding less invasive medical devices, patient-specific boluses were produced with superior density uniformity, and successfully used for controlled dose distribution in radiotherapy. Moreover, a patient-specific palatal plate ensured better fit and longer time to displacement without the use of adhesive cream. 121 Limb orthoses and prostheses improved patients' conditions to varying degrees; nonetheless, high patient satisfaction scores 119 and larger motivation for rehabilitation training 118 were reported.
Twenty-six studies were performed with control groups of patients undergoing similar procedures performed with conventional techniques. Of these, 13 were in orthopedics,51,67,70,73,74,77,78,86,88,91,97–99 4 in orthopedic oncology,46,67,86,114 and 3 in orthotics,75,113,118 and single studies were in anesthesiology, 82 gastroenterology, 73 maxillofacial surgery, 116 neurosurgery, 100 oncology, 98 and plastic surgery. 101 In comparison with conventional approaches, the use of 3D-printed patient-specific implants and guides leads to increased accuracy of the procedure, reduced operating time, lower radiation exposure, comparable or smaller intra-operative blood loss, smaller number of surgical errors, comparable or improved quality of outcomes, less postoperative drainage volume, and fewer postoperative complications.
Lador et al. 16 reported that a titanium lattice structure created significantly less radiologic interference when compared with other implants, allowing for better adjuvant radiation therapy and local disease recurrence monitoring. On the other hand, Chatain and Finn 43 pointed out that a titanium sacral implant for pelvic reconstruction in orthopedic oncology may be suboptimal when follow-up imaging is needed due to extensive radiological metal artifact. Surgical guides facilitated preoperative planning and simplified the operative procedure, which was highly accurate and consistent with the plan. Positive feedback from patients was noted in several studies. One study reported high satisfaction rates among patients up to 60 months postsurgery, and up to 83% of these patients expressed the willingness to have the procedure again if needed. 38
Regulatory aspects of 3D-printed medical device use
In 29 studies, medical devices were manufactured by the following certified companies: Anatomics (Melbourne, Australia),15,21,29,35,37,39,41 4WEB Medical (Frisco, TX),16,61–63 AK Medical (Beijing, China),32,42,56 Medacta International (Castel San Pietro, Switzerland),85,88 3D Systems, 43 Beijing ThousandMed Innovation Technology (Beijing, China), 100 Bodyarch (China), 113 DePuy Synthes (West Chester, PA), 24 Instrumentaria (Sesvete, Croatia), 18 Mobelife NV (Materialise, Leuven, Belgium), 49 Medicrea (Rillieux la Pape, France), 28 Newclip Technics (France), 71 Ossis (Christchurch, New Zealand), 52 Stryker Orthopaedics (Mahwah, NJ), 59 Thytec Shanghai (Shanghai, China), 58 Wright Medical Group (Arlington, TN), 69 and Metaklinik (Metaklinik.com). 124 One study used titanium implants iFuse-3D™ (SI-BONE), cleared by the US FDA in 2017 for sacroiliac joint fusion, 38 and another used off-the-shelf implants Medussa-PL (Medyssey) for lumbar interbody fusion. 40 In these cases, additional approval for the use of the devices was not required.
Seven studies addressed regulatory aspects of 3D-printed medical device use directly. One study on spine-stabilization endoprostheses detailed the process of ensuring compliance with the EU Medical Device Regulation, including the required procedural blueprint and a technical file with a thorough description of all steps and procedures. 30 A patient-specific titanium truss cage received compassionate use approval by an institutional review board for a single-time use to avoid below-knee amputation. 62 Similarly, a patient-specific endoprosthesis in a case of sacral chordoma received FDA approval via the emergency and compassionate use of unapproved devices. 43 The authors in that study noted the long duration from surgeon request to implantation (4 months) due to the complexity of implant concept modeling and the FDA approval process. 43
A study of implantable airway splints for pediatric patients reported that to receive the splint, the compliance of each patient with the criteria for the FDA Emergency Use Exemption was verified by an impartial third-party physician. 19 By virtue of the FDA guidelines, investigational devices were restricted to a limited number of uses before the formal regulatory approval process had to be pursued, thus limiting the initial number of patients recruited to 3. One tantalum patient-specific implant was designed under the parameters of “Personalized Additive Manufactured Medical Device Technical Censoring Guidelines” by the Center for Medical Device Evaluation of China. 48 According to the authors of the study, a needle guide for in-plane ultrasound-guided nerve blocks falls under the FDA designation of a medical device Class I, and its use in their hospital did not require registration with the FDA, investigational device exemption, or Institutional Review Board approval, because it was not for sale, or used in a study or experiment. 89 Finally, one study reported using a non-FDA approved endoprosthesis. 31
Discussion
Dominant and emerging fields of application of 3D printing for medical device production
The largely dominant fields of 3D-printing application in medicine are orthopedics and orthopedic oncology, with increasing numbers of studies on patient-specific surgical guides and/or implants published since 2015. Often, the simultaneous use of both is reported, and medical-device companies that produce patient-specific implants typically offer corresponding cutting/drill guides to avoid mismatch between the size of the implants and defects after resection.
The emerging use of 3D printing is for patient- and/or procedure-specific medical devices to facilitate precision procedures in neurosurgery and oncology,91,92,94,95,100 and ensure planned dose distribution in radiotherapy.17,99,107–109
Technology use trends in medical-device production
Certain trends regarding the use of materials and 3D-printing processes were identified. Based on the reviewed studies, the most common material for 3D-printed implants is titanium alloy (Ti-6Al-4V), known for its excellent biocompatibility, biological inertness, favorable strength-to-density ratio, and superior corrosion resistance. 125 It is of note that the final strength of titanium parts varies depending on the design and printing technology used, and it is not a priori guaranteed. 44
The vast majority of implants were printed using EBM. A few studies preferred SLM due to the higher accuracy and superior mechanical properties of the printed parts. 23 Nevertheless, additional heat treatment is needed after SLM to eliminate high residual stresses, 125 and the surface roughness resulting from EBM represents an advantage for medical applications where tissue incorporation is desired. 126 Technical difficulties were noted during the insertion of rough-surface implants without causing neural or cartilage tissue injury, 40 and a possible risk of infection with the development of biofilm on titanium was also reported. 63
Single-use surgical guides and instruments were mainly printed in biocompatible polymer-based materials that are less costly and more accessible. Medical-grade PA was the material of choice due to its high production strength and accuracy, temperature-, corrosion-, and deformation-resistance, and resistance to breakage. 70 Among the noteworthy 3D-printing-related adverse events during surgery were splitting of an SLA-printed resin drill guide 83 and an FDM-printed PLA cutting guide 76 by rough handling, and an unplanned over-resection due to a jammed sliding mechanism in an SLS-printed PA resection jig. 69 For retractors, PC was found to be too brittle, whereas resin models were much sturdier and capable of withstanding pressurized steam sterilization without deformation. 104
For noninvasive devices that did not require sterilization, the choice of material depended on their specific use. Radiotherapy boluses in prolonged contact with facial skin were fabricated in soft, flexible materials (e.g., Agilus-60, NinjaFlex) to ensure comfort during therapy, and conformality to complex anatomy. 107 It was also important that the boluses were printed at 100% infill to create a solid, homogeneous object with radiological properties resembling those of water. 17 In orthotics, resistance to breakage was one of the key requirements, thus PLA (FDM) was found to be most appropriate.
Advantages and drawbacks of the use of 3D printing for medical device fabrication
The use of 3D printing for medical-device production was consistently viewed as advantageous across the reviewed studies. Generally reported were increased procedure accuracy, reduced duration, and improved quality of outcomes compared with traditional approaches. An important advantage of medical-device personalization is also the possibility of solving rare, unconventional medical problems.33,127 In several studies, patient-specific guides were described as easy to use, even by less-experienced operators; and an additional benefit was in orthopedic oncology, where they provided the possibility of close, but tumor-free margin resection while preserving the native joints. 58
Although the benefits of 3D-printing for medical-device fabrication have been addressed in previous reviews, certain economic and clinical concerns were also expressed in the reviewed studies that need mentioning. Among the most common were the cost and duration of patient-specific device production, especially when outsourced to specialized commercial entities.23,28,29,39,49,62,63,72,76 The price of 3D-printed implants is estimated to be two- to five-times higher compared with conventional implants,28,128,129 and additional costs include preoperative virtual planning, device design, and the production of trials or implant variations.
Outsourcing is virtually inevitable for titanium implants due to their complex structure and the high cost of EBM machines. However, studies involving relatively simple devices printed in polymer-based materials also reported notably lower cost compared with conventional devices,76,104 and successful in-house design and fabrication by medical staff.23,76,110
Longer waiting periods for custom implantable devices may predispose patients to malignant changes, disease progression, or anatomical alterations, which can complicate implantation.21,31,43 Manufacturing times would also need to improve to include acute cases 41 or contingency use. Cases of overnight production of medical devices for urgent interventions have already been reported,130,131 and it is expected that increased use and technological improvement will reduce production time. 21
The majority of concerns expressed in the reviewed studies were related to patient-specific implants and surgical guides. Two important drawbacks of patient-specific prostheses were the possibility of defect/implant mismatch, and the difficulty of implant removal due to bone-tissue ingrowth. The custom form of the prostheses demands complete commitment toward the preoperative resection plan, which is not always feasible due to unexpected differences between computer-reproduced and actual anatomy.31,42 Very limited possibilities of intraoperative implant modification may cause the need to modify the operative procedure.42–44 To avoid this, some authors chose to prepare several sizes of implants for intraoperative selection.16,30,32,33,46
However, patient-specific devices are considered “custom” by the FDA, and they can only be produced in fewer than 5 units per year. 1 In instances when several iterations of the same device are produced for a single patient, the unused devices must be returned to the manufacturer and/or destroyed, which has to be certified by the physician. 132
The second drawback regarding implants refers specifically to their porous structure that facilitates osseointegration. Although good incorporation is a desirable outcome, it may complicate implant removal in the case of hardware failure, requiring additional bone resection around the implant.63,133 On the other hand, Wei et al. 45 reported that due to bone ingrowth into a sacral endoprosthesis, instrument failure at 8 months of follow-up did not impair the quality of life and ambulation.
Regarding patient-specific cutting/drill guides, one of the main problems reported was the need for soft tissues to be completely removed to make the guides fit the boney anatomy, which can increase intraoperative blood loss and operation time.78,83 Any slight relative activity during operation, unplanned breakage of bony landmarks, or unexpected anatomical features can cause discrepancies between the presurgical simulation and the actual procedure,83,88 and may even prevent the surgical procedure from being performed. 86 Finally, with resection guides, the depth of osteotomy can be difficult to estimate, potentially leading to extensive cartilage damage. 68
Regulatory aspects of 3D printing of medical devices
At present, all medical devices, including those that are 3D printed, must conform to the same regulatory frameworks to be used legally. The regulations vary across different countries and were reviewed in previous papers for the United States,11,134 the European Union (EU),11,134 Japan, 134 and Australia. 11 Nevertheless, the potentially personalized nature and decentralized manufacturing of 3D-printed devices present unique legislative challenges, especially in cases that do not allow for lengthy processes of obtaining regulatory approval.
For example, the standard FDA approval of Class III medical devices is a lengthy process that can take 3–7 years, and it requires preclinical laboratory and animal testing, and clinical trials. 1 This can present substantial barriers especially when rare, life-threatening, or severely debilitating medical conditions need to be treated urgently. For these cases, specific pathways are established for expanded access to unapproved medical devices. 1
In the United States, the majority of 3D-printed medical devices are cleared by the FDA under the emergency circumstances or via the conventional 510 (k) pathway, 2 including many of those produced by the medical companies listed in this review. The expanded access programs for rapid approval of products that have not yet received FDA approval include Emergency Use, Compassionate Use, Continued Access, and Treatment Investigational Device Exemption. 134 Companies such as Ossis offer individual applications for patients to receive a compassionate use approved medical device. 135
In the EU, exceptional use of non-CE marked medical devices can be authorized according to the MDR on a case-by-case basis at the request of a medical consultant and/or device manufacturer. 13 Both the United States and EU regulations also include a specific exemption for custom-made devices.1,11
Most of the studies that reported the use of approved devices outsourced their design and fabrication to established medical companies, and in only three cases, the approval was acquired via compassionate or emergency use exemption.19,43,62 Almost three-quarters of the studies did not detail regulatory aspects, or only described obtaining permission to use the device from an internal review board.
Interestingly, the use of custom device exemption was only reported in one European study. 30 In the FDA regulations, such an exemption applies to devices that are designed to treat individual patients' unique pathology/physiology, and thus they necessarily deviate from an otherwise applicable performance standard such that investigations would be impractical. They are also not generally available for commercial distribution from a manufacturer, importer, or distributor. 1 It has been acknowledged in previous papers that the clinical and regulatory issues regarding custom 3D-printed medical devices were complex and evolving, especially to prevent their uncontrolled use and human experimentation.1,136
Limitations
Some studies of other medical devices were excluded from this review, as they did not meet our inclusion criteria regarding the data provided on 3D-printing technology or patient testing, or because they employed indirect AM. Also excluded from this study are papers addressing anatomical modeling for surgical planning, which is now quite well reported in the literature. The authors also note that there might be inconsistencies regarding the employed materials and technologies in the previous studies that we were unable to clarify.
Conclusions
The use of 3D-printed medical devices in the direct treatment of patients has increased considerably since 2015. This review identified 110 papers reporting on 140 medical devices, the technological aspects of their fabrication, and their use and clinical outcomes in several medical fields. Metal and nonmetal 3D printing in orthopedics and orthopedic oncology were the most common applications, and this was led by established companies with regulatory procedures. There is an emerging trend toward the use of nonmetal 3D printing in medicine for patient-specific and precision devices in neurosurgery and oncology.
Regarding implantable devices, the most used material was titanium alloy and the most commonly chosen 3D-printing technology EBM. For surgical guides and instruments, polymer-based materials were most often used, notably medical-grade PA with SLS, and PLA with FDM. Noninvasive devices that did not require sterilization were mostly printed by using FDM, and the choice of material depended on the device's specific use.
Several advantages of 3D-printed medical devices were consistently reported across the reviewed studies, including the possibility of solving rare, unconventional medical problems, increased procedure ease and accuracy, reduced duration, and improved outcomes. Among the most commonly reported drawbacks of 3D printing were high cost and relatively long manufacturing times, particularly the latter regarding the management of progressive diseases and emergencies. For patient-specific prostheses and surgical guides, the most frequent concern was that the actual procedure needed to precisely match the preoperative plan, which cannot always be achieved due to unpredictable intraoperative situations.
Approximately a quarter of the studies outsourced the device design and fabrication to certified medical device companies, and in almost three-quarters, permission to use the device was obtained from an internal review board. There is a need to further support rapid regulatory and ethics review approaches to optimize the potential for use of 3D printing in medicine, in particular for time-critical clinical challenges.
Footnotes
Authorship Confirmation Statement
T.K. performed the systematic search, extracted the data, and led to the writing of the article. A.S. was the second reviewer and contributed to the study design and article writing. K.J.O.S. contributed to the study design and the writing of the article. C.M. contributed to the analysis of the literature and the writing of the article from a manufacturing perspective. C.P.D. contributed to the analysis of the literature and the writing of the article from a medical perspective. L.W.O.S. contributed to the study design, oversight of the search and analysis, the structure of the article, and the writing.
Acknowledgments
None other than the funding bodies that are detailed next.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This publication has emanated from research supported by Science Foundation Ireland (SFI) under Grant Numbers SFI 16/RC/3918 and SFI 20/COV/0031, co-funded by the European Regional Development Fund.