
Abstract
The COVID-19 pandemic has caused an overload on the health care system on a global scale. Because the disease affects the respiratory system, patients may require ventilator equipment for breathing, and consequently, numerous tracheal intubations have been performed. The video laryngoscope is a medical device that aids this procedure. It is used by anesthesiologists to visualize the anatomical structures of the larynx during tube insertion. Unfortunately, many hospitals worldwide are unable to afford sufficient units of this medical device. To satisfy the high demand, low-cost alternatives employing three-dimensional (3D) printing techniques have been developed for health care professional's use. With the intention of ensuring the efficiency, reproducibility, and security of the 3D-printed laryngoscope, this article presents a novel model with versions for pediatric and adult use, which was developed under the supervision of a medical team. The mechanical performance of 3D-printed prototypes (of the proposed models) was evaluated using mechanical assays, and the results indicated a satisfactory safety factor.
Introduction
Our academic laboratory has been focused on computer-aided design (CAD) and three-dimensional (3D) printing for Research and Outreach, developing biological and molecular haptic artifacts for educational purposes, patient-specific computed tomography models, and medical devices such as intraoral positioners for radiotherapy treatment since 2018.
We agree with the arguments listed by Powell et al., 1 who enumerated fundamental conditions that impact readiness to adapt to critical challenges during the COVID-19 crisis, such as the immediate manufacturing capacity of 3D printing, a reliable network of physicians with real-time understanding and exposure to clinical needs, and design/manufacturing abilities. The pandemic made us consider how we could redirect our skills and leverage our knowledge to address the requirements of our institution, region, state, and country.
In terms of the digital value chain for the development and fabrication of components for 3D printing, the ISO document “ISO 17296-4:2016 Additive manufacturing—General principles—Overview of data processing” 2 recommends that data-sharing methods could include the file type, ideal settings for 3D building (with safety and guarantee of reproducibility), and description of the application of the created artifact.
According to Ivanov and Das, 3 low-frequency high-impact (LFHI) episodes pose a significant risk to supply chains (SCs). The repercussion of such events that cascade through an SC is named “ripple effect.” 4 Severe acute respiratory syndrome (SARS)-CoV-2 pandemic outbreaks are a special class of LFHI SC risks. In contrast to geographically centered events, such as natural/industrial catastrophes, a pandemic is not restricted to a specific region or limited to a precise and immutable chronological framework. Different components of a SC are affected sequentially or consecutively; manufacturing, distribution centers, logistics, and markets can become disabled within overlapping time windows. To mitigate the consequences of the ripple effect, many nations are investing in strategies based on Manufacturing 4.0.
Open Access is in synergy with the goals of the World Health Organization meeting at Geneva in February 2020. After the validation of the medicine and nursing professionals (which guarantees the enhancement of ergonomic and functional aspects of the designed devices), we will make the files available (on the university platform for free download) to be printed anywhere in the world.
According to Salmi et al., 5 three ISO/ASTM 3D-printing processes have been employed to fabricate items for mitigating the effects of the COVID-19 pandemic: photopolymerization, material extrusion (ME), and powder bed fusion. The authors mention that ME technology is frequently used to fabricate products that are not medically approved, considering that the results might not exhibit an incontestable performance, substantially, relied on: (1) the impossibility of submitting devices printed through extrusion of melted material to autoclaving and (2) the presence of crevices between sequential polymeric layers, which can favor biofilm growth. To overcome these obstacles, Salmi et al. 5 suggested sterilization with 96% isopropyl alcohol for 5 min.
As an alternative, the authors state that it would be beneficial to invest in materials approved for medical use. Most digital manufacturing laboratories in developing countries (1) use predominantly ME (through a process in which melted material is selectively dispensed through a nozzle, allowing 3D construction on a build platform) and (2) adopt the terminology recommended by ISO/ASTM 52900. 6 Thus, it is imperative to maximize investments and interests in fields where it is possible to investigate the potential and limits of ME to produce medical devices.
In this work, we report how our laboratory started to produce low-cost laryngoscopes, which can be coupled to digital cameras, facilitating the intubation process in patients affected by COVID-19. The most significant challenges in the treatment of COVID-19 patients are bilateral pneumonia and acute respiratory distress syndrome. The video laryngoscope facilitates visualization of the glottis and tracheal intubation, particularly in difficult cases. The device reduces the amount of time needed to perform the maneuver and consequently the probability of contamination. Hence, in pandemics, it is imperative to enhance access to this medical device using additive manufacturing.
Chepelev et al. 7 from the University of Ottawa reported that their hospital failed to purchase enough laryngoscope blades from the manufacturer, necessitating local production. Owing to medical compatibility and sterilization requirements, they used PolyJet Connex3 Object500 with the MED610 material, the SUP705 Supplementary Video S1, and a glossy finish (Stratasys, Rehovot, Israel). The expensive 3D printer used by Chepelev et al. 7 has outstanding performance (high resolution) and allows the utilization of materials that can be properly exposed to an autoclave without affecting the product parameters/properties. However, as citizens of Brazil (with deep social inequalities), when we face exorbitantly priced machinery, the words of the historian Harari 8 echoes in our minds: “Humanity needs to make a choice. Will we travel down the route of disunity, or will we adopt the path of global solidarity?”
The anesthesia department at our university reported the need to fabricate inexpensive laryngoscopes that can be replicated anywhere in the world. Initially, it was believed that the printing of the file shared by the AirAngel Blade™ project would satisfy the expectations of physicians. However, we developed an innovative model (inspired by the AirAngel Blade) to overcome the challenges presented by anesthesiologists. Our prototypes (pediatric and adult) have many structural modifications that enhance the performance of medical devices.
The combination of a 3D-printed blade with electronic cameras makes it possible to produce low-cost video laryngoscopes, which can improve patient safety, particularly in vulnerable populations, and democratize access to this medical device. Therefore, 3D printing has played an important role in the current pandemic. As Harari 8 said, “Every crisis is also an opportunity. We hope that the current epidemic will help humankind realize the acute danger posed by global disunity.” Thus, we intend to share our AM files, with the aim of obtaining victory against “not only the coronavirus, but against all future epidemics and crises that might assail humankind in the 21st century.” 8
Materials and Methods
Ethical approval for this study was obtained from Irmandade Santa Casa de Misericórdia de Porto Alegre Ethics Committee (Number: 58735522.8.0000.5335).
This study consists of the development of a 3D-printed video laryngoscope, based on the comparison between commercial versions and 3D-printable models available online. 9 A novel design was developed to adapt basic materials that can be purchased through the Internet, considering the recommendations from an expert team of anesthesiologists.
Adult and pediatric models (inspired by the AirAngel Blade prototype) were designed to satisfy the performance requirements of the medical device, reducing the time of intubation and thus theoretically minimizing the exposure of the health care frontline to viral particles dispersed in the hospital environment.
The main innovative aspects of Laboratory of Innovation, Prototyping, Creative, and Inclusive Education (LIPECIN) laryngoscopes are as follows: (1) the presence of a sinuous groove ensuring the existence of a prehensile structure that prevents the rotation of the boroscopic camera; (2) the ergonomic blade handle facilitating the management of the artifact; (3) the displacement of the digital camera to the left, considering that the technical maneuvers for intubation of the trachea are performed on the right side; and (4) the removal of obstacles on the right side, which can hinder the passage of the tracheal tube toward the trachea.
The novelty of this work is the possibility of fabricating laryngoscopes (with quality and validation) with affordable computer numerical control machines (desktop 3D printers) for emergency use during a pandemic. All studies related to AM were performed at LIPECIN, Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), and the mechanical assays were conducted at Universidade Federal do Rio Grande do Sul (UFRGS). For digital modeling, the CAD and computer-aided engineering software Fusion 360® (Autodesk, Inc.) was used.
The code for printing the digital file (in G-code extension) was prepared using the Cura® 4.5 software (Ultimaker Company), and the basic parameters were set to correspond to the expected mechanical efficiency and surface superiority, avoiding irregularities and undesirable crevices. Subsequently, the code was exported to fusion deposition-based equipment (Ultimaker® 2+; Ultimaker Company), and polylactic acid was applied as the material (BASF Natural Ultrafuse® PRO1 PLA 3D Printer Filament, 2.85 mm).
Simulations and training with senior research assistants and resident physicians were performed at the Center of Simulation of UFCSPA. After the training and approval of disposal, microbiological essays, clinical trials, and applications shall be performed.
Modeling
The laryngoscope consists of two main parts: a handle and a blade. In addition, there are detailed component specifications for this medical device, such as a camera holder, flange, groove, and tip. For the design of these models and identification of components, studies involving similar products, such as the AirAngel Blade and C-MAC® laryngoscopes, were analyzed, and the designations addressed served as guidelines for the modeling of the current prototypes. 10
As part of the studies, meetings with senior anesthesiologists and resident physicians (users of the equipment) were organized for discussions regarding usability. During these meetings, the available laryngoscopes and the proposed model were manipulated and tested at the Center of Realistic Simulation of UFCSPA.
For the process of modeling, a CAD tool like Fusion 360 (Autodesk, Inc.) is considered a suitable choice for providing the following: (1) easy geometric manipulation; (2) dimensional accuracy; (3) an iterative shape generation process; (4) time and cost reduction compared to other methods of prototyping; and (5) integration with AM systems. 11 The following improvements were considered for the design of the model (Fig. 1):
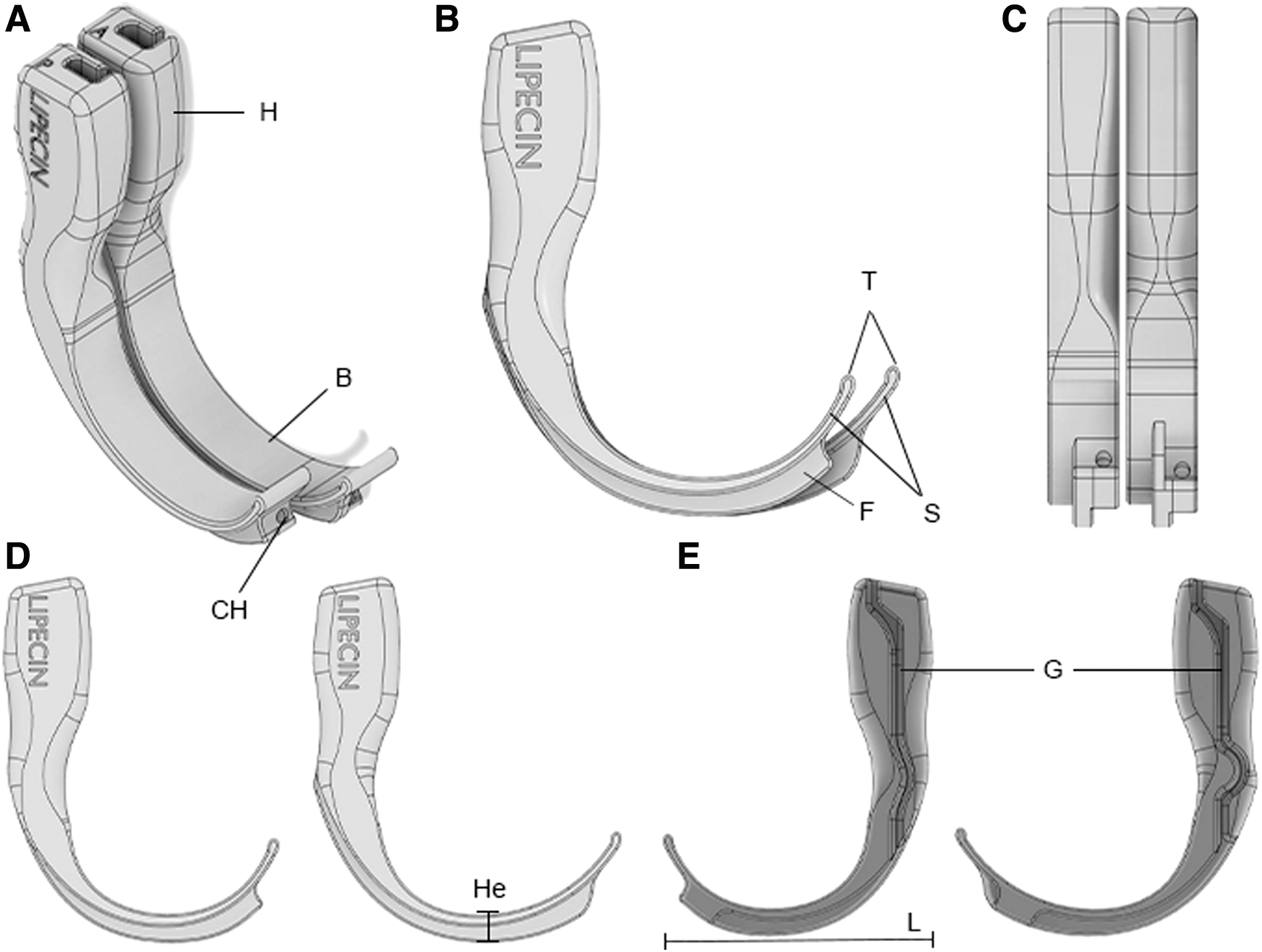
Comparison between adult and pediatric laryngoscopes.
The handle was designed with an ergonomic curvature, stimulating a gentle prehensile movement and enhancing the comfort of the anesthesiologist.
An improved and innovative method for fixing the camera without additional components was developed, ensuring that the laryngoscope could be made from a single piece. The sinuous trajectory of the groove avoids the detachment of the wire from the handle, blocking any eventual camera rotation.
Compared with the previous prototypes, the blade height was reduced, requiring less aperture from the mandible for insertion of the device.
The tight camera holder prevents the wire from sliding toward the patient's glottis, mitigating potential injuries.
Iterative design process
In this section, we describe in detail the iterative design process of the medical device, including the created versions, feedback from the medical team, and improvements. The first laryngoscopes (AirAngel Blade models) were printed in April. Initially, the group of anesthesiologists who work with us as collaborators (and are co-authors of this work) was only interested in printing the available models. However, during the attempt to attach the boroscopic camera, we felt the need to reduce the diameter of the camera holder located on the tongue/spatula, as it would easily slide beyond the beak/tip through the patient's glottis/larynx during the insertion of the device into the oral cavity, increasing the risk of injury and making intubation difficult owing to the chances of obstruction.
First, we have asked Bryan Archpru (who was responding for the AirAngel™ project in United States) whether the laryngoscope blade license would let others remix, adapt, and build upon his work for noncommercial purposes. We wish to modify only one aspect (diameter of the holder) of the file to facilitate camera anchorage. However, as the simulation processes were conducted with prototypes that mimic human anatomy, it was clear that the AirAngel Blade model would not satisfy the expectations of our anesthesiology collaborators. Therefore, we decided to design something entirely innovative based on the suggestions made by the medical team.
Herein, we describe chronologically (from May to July 2020) the iterative modifications made to the artifact until it was adequate to achieve the performance expectations of the COVID-19 frontline: (1) translocation of the digital camera coupling from the left side to the right side, facilitating the observation of the upper airways; (2) conspicuous reduction of the blade height (Fig. 1D) as an effort to mitigate all types of mechanical stresses during the introduction of the equipment in sedated patients, contributing to a successful intubation, without any chance of sequel/physical damage.
New tests were performed at the simulation center, but the virtual camera was still rotating at the linear groove along the handle and blade. The medical team mentioned that, in addition to our focus on patient safety and comfort, it would be interesting to consider the anatomical plasticity of the physician: the doctor's hands must properly hold the object, making it easier to insert the cannula into the patient. Therefore, elongation of the handle would maximize the maneuverability of the artifact.
Thus, the following changes took place in May 2020: (3) the application of a sinuosity in the groove in which the camera would remain static/immobile without the possibility of rotation (allowing the amplification of speed and safety during the intubation process) and (4) an increase in the length of the handle, which became curvilinear, enhancing the ergonomic properties of the artifact. (5) We created two models for adult and pediatric purposes in the months of May and June, with the identification of the objects with the letters P (pediatric) and A (adult). They differed with regard to the length of the blade and the tongue (Fig. 1B), providing equal capabilities for safe intubation in adults and children.
We attempted to carve our laboratory logo on the handle, which was represented by a 3D printer extruding a DNA molecule. (6) However, after some 3D printings, we abandoned this idea, opting to identify our prototypes only with a subtle impression of the word LIPECIN, avoiding additional crevices that could favor the deposition of biofilms owing to the difficulty of proper cleaning (keeping in mind the eventual evolution of the project toward multiple-use devices instead of single-use devices).
In June and July, we decided to perform 3D printing exclusively with pigment-free plastics (BASF Natural Ultrafuse PRO1 PLA 3D Printer Filament, 2.85 mm). We observed that certain pigments linked to the thermoplastic can putatively interfere with the quality of deposition of layers.
Manufacture
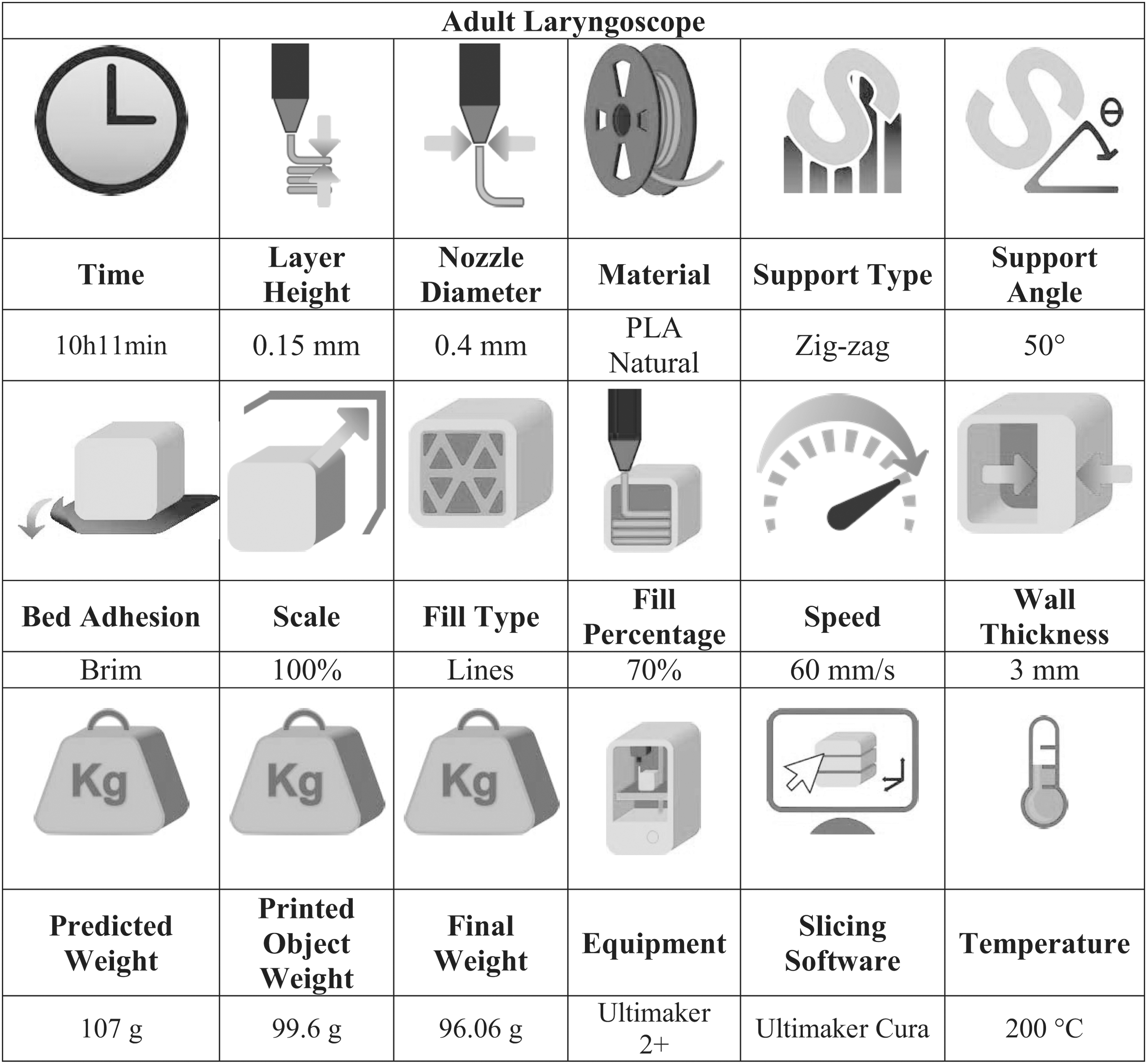
After the models were established, the files were exported to the slicing software Cura 4.5 (Ultimaker Company), as shown in Figure 2. This stage is fundamental for 3D printing, because all the manufacturing parameters determine the quality of final products. Currently, there is a transcription in the G-Code for the interpretation of the equipment. It is essential to use the configurations described in Tables 1 and 2 to assure the reproducibility, excellence, and safety of the prototypes, considering the public dissemination of these medical devices. 12
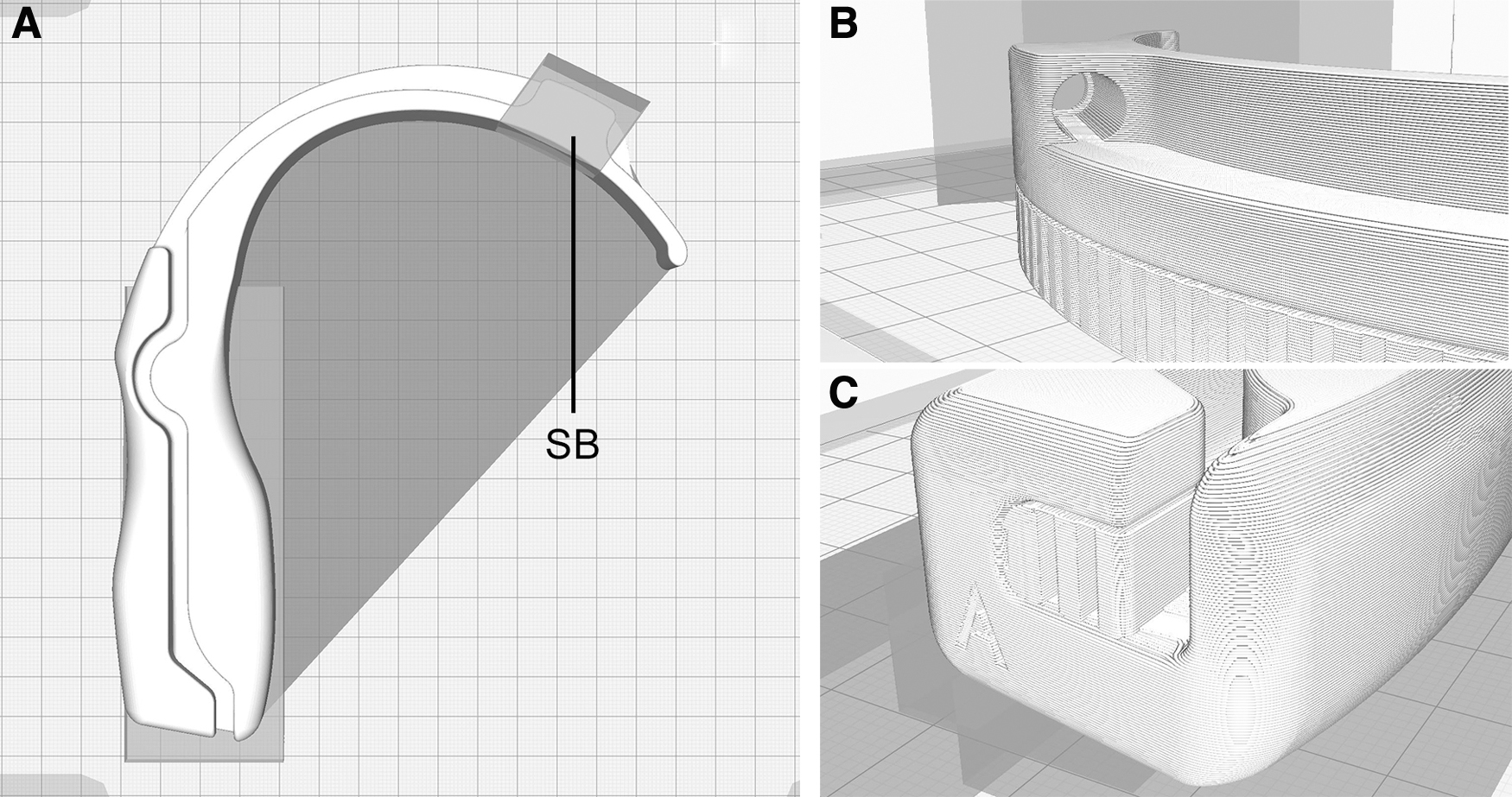
Inclusion of support blockers is related to smooth construction of the laryngoscope blades.
Optimal Set of Parameters for Fused Filament Fabrication and Characteristics of the Adult Laryngoscope
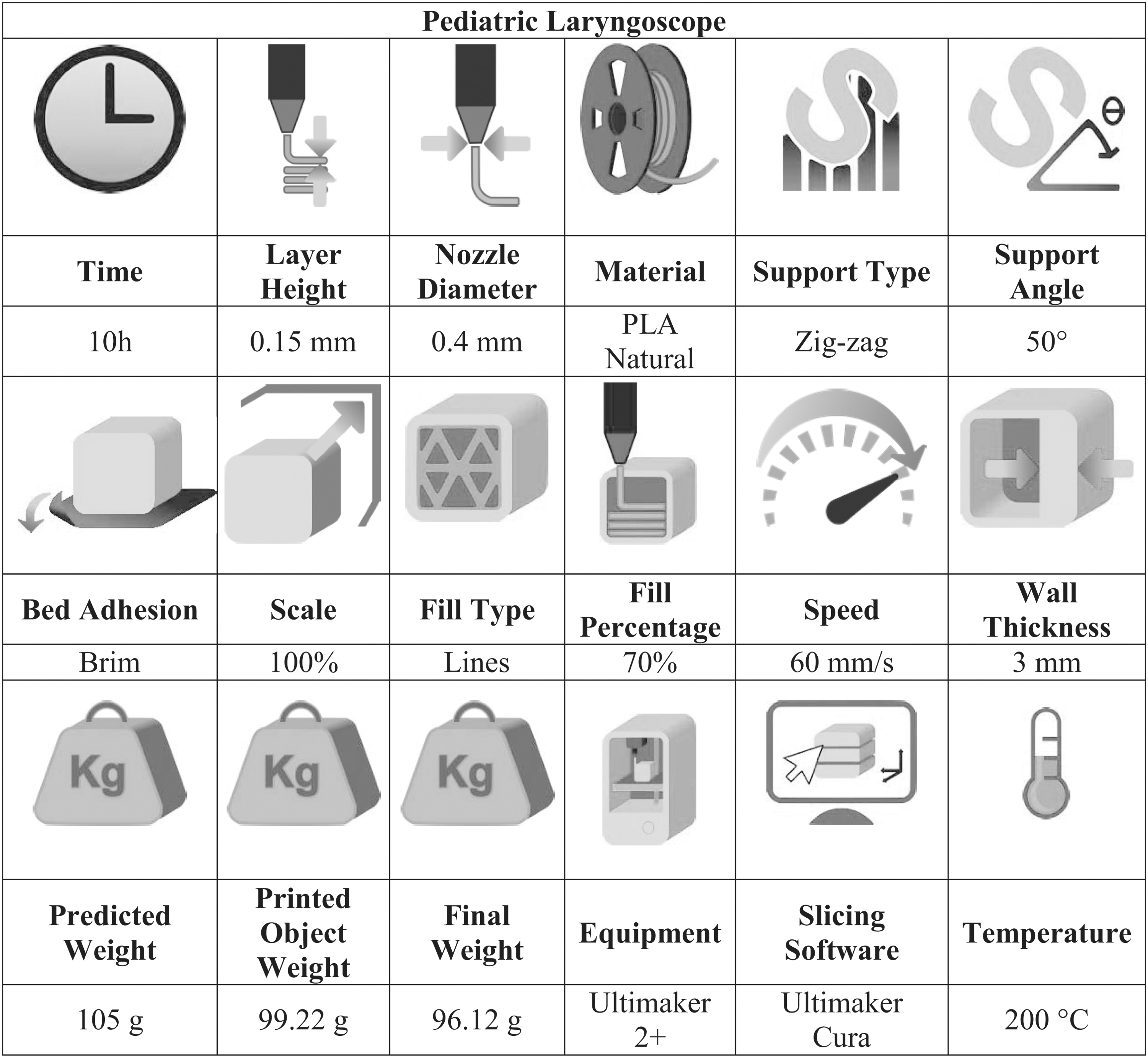
Optimal Set of Parameters for Fused Filament Fabrication and Characteristics of the Pediatric Laryngoscope
The addition of support structures in Cura maximizes the probability of a successful 3D printing process. However, automatically inserted support structures can be a hindrance and even result in ineffectual or unsightly artifacts. Hence, in this study, we found strong evidence that the inclusion of support blockers (Fig. 2A) is related to the smooth construction of laryngoscope parts.
Samples and testing
Twenty samples were printed until the final design and functionality was approved by the anesthesiologist's team. We then tested the resistance of six printed laryngoscopes to mechanical examination at the Physical Metallurgy Laboratory (UFRGS).
Traction assays (Fig. 5A, B) considering axial displacements were performed using a Materials Testing System (MTS) machine (810 MTS, Eden Prairie, MN). The tests were performed in triplicate to accurately estimate the resistance of the object, for both the adult and pediatric models. The conditions of the printed samples during the mechanical assays were as follows: (1) insertion of a pin in the handle, allowing rotation on its own axis, and (2) assembly of a clasp on the distal end of the blade, allowing it to slide in a direction perpendicular to the traction force.
The handles were drilled 10 mm from the superior surface, in the distal axle, to traverse a 10-mm-diameter pin, which was used to attach the samples to the device. The distal end was fixed to the test machine using grips. This configuration permitted free movement of the specimens, which allowed them to align with the distal axle naturally when the tests began. The samples were subjected to tensile loading in the distal axle direction; thus, a tensile force was induced on the distal end of the blade, which was expected to be the fracture region during the tests, because it was the thinnest region of the specimens. The test speed was 10 mm/min in the MTS servo-hydraulic machine. Owing to the pandemic situation and the urban mobility restrictions in Brazil, the tests were conducted in a single visit to the resistance analysis laboratory.
Application
A smartphone is needed to obtain images from the external camera through a USB connection. The application used in the first set of tests was CameraFi2 (Vault Micro, Inc.), which allows the smartphone to visualize, take pictures, and record videos. During the first video laryngoscope simulation, the absence of a tool to turn the camera virtually without manual rotation was reported, and for this reason, the app was replaced.
In the following simulations (Fig. 4), trials were performed using On The Go View (Team Force Enterprise). This software has various features, for example, 90° or 180° rotation in both directions, vertical/horizontal image reflection, resolution amplification and brightness, contrast, shade, saturation, and distinctness setup. Therefore, an application with the previously described features is recommended to mitigate the difficulties in visualizing anatomical structures.
Results
3D printing
The process parameters are essential factors for achieving successful 3D printing (Fig. 3). Therefore, this work recommends a layer height of 0.15 mm, fill of 70%, and wall thickness of 3 mm. The Cura software predicted weights of 107 g for the adult laryngoscope and 105 g for the pediatric laryngoscope, including the Supplementary Video S1. The printed artifact (newly built at the plate) and the final prototype (after removal of the support) weighed 99.6 and 96.06 g, respectively, for the Adult Model, and 99.22 and 96.12 g, respectively, for the pediatric model.
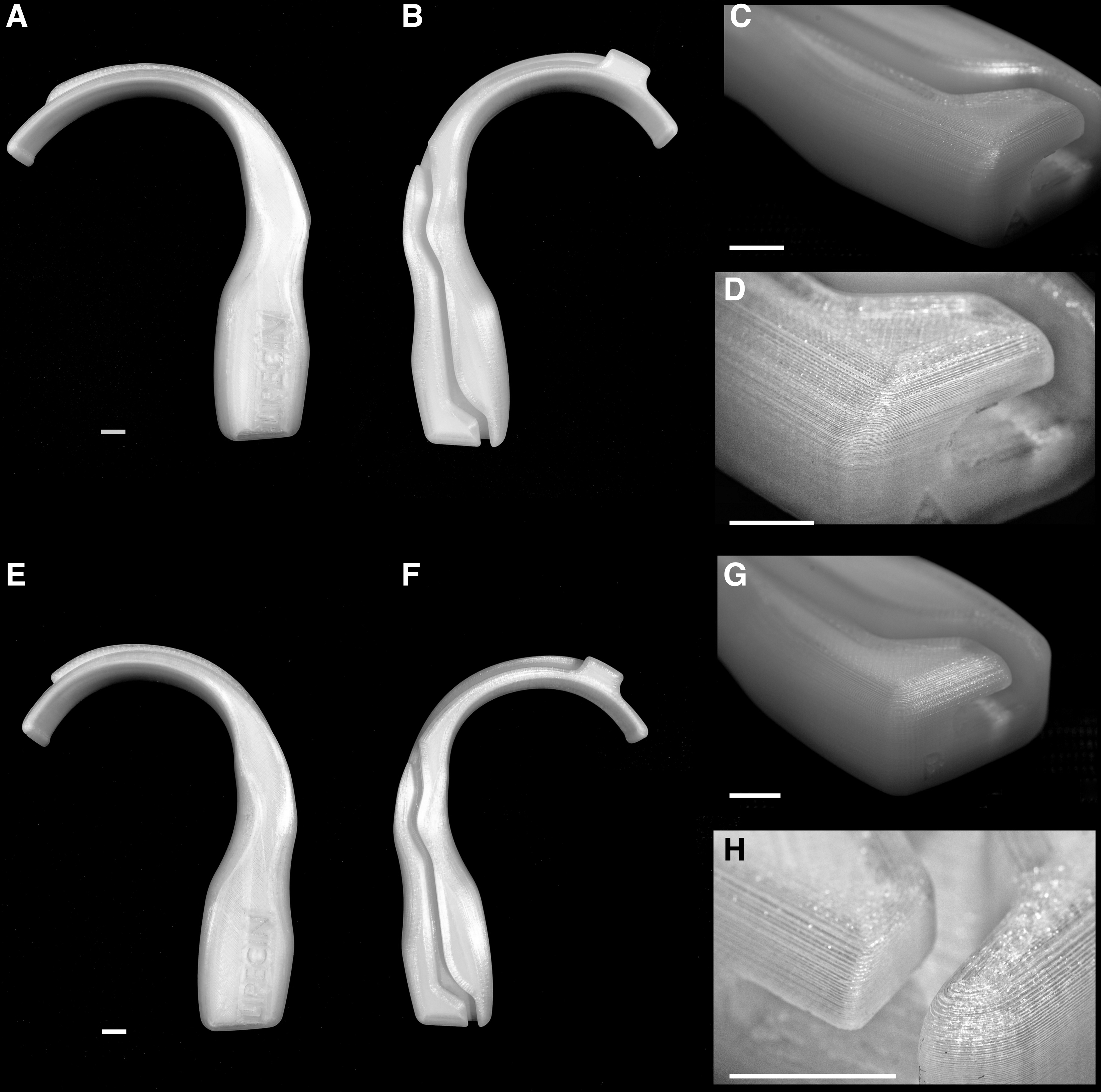
Tridimensional printed laryngoscopes (scale bar represents 10 mm).
The AM occurred in a controlled environment, with an average temperature of 25.8°C and air humidity of 47%. Support structures generally leave marks at print touch points. These must be post-processed to achieve a smooth finish. Regularly, we used pliers and physical abrasion for support removal instead of chemical solutions. The stereolithography files and process parameters can be downloaded freely using this link.
Stress–strain traction assays
Pediatric blades presented higher axial force values until failure, that is, 476.27 N (ranging from 461.10 to 494.83 N), whereas adult blades resisted 404.27 N (ranging from 391.37 to 415.17 N) (Fig. 4). There was no fragile failure in any device under the applied force (Fig. 5C). All blades underwent a flow process after reaching the peak load and were loosened from the device used to fix them, as flow streaks were observed in all blades (Fig. 5D).
Table 3 shows the average of the force measures applied to the adult and pediatric samples, which were 404.26 and 476.27 N, respectively. The coefficient of variation, that is, the ratio of the standard deviation to the mean, was calculated to verify the variability of results. The results indicated a low variability of 2.43% for the adult model and 2.94% for the pediatric model.
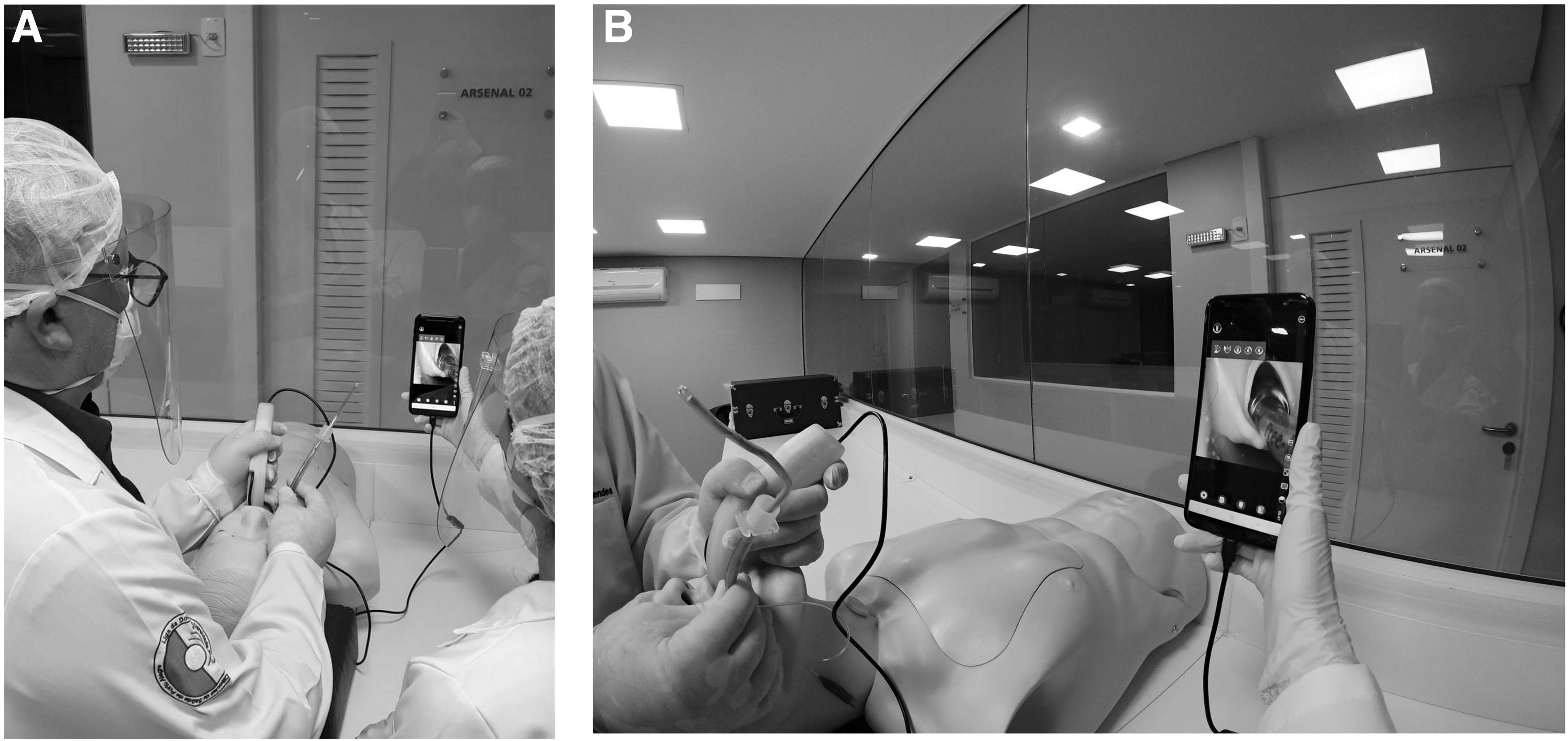
Management of the video laryngoscope in a simulation setting.
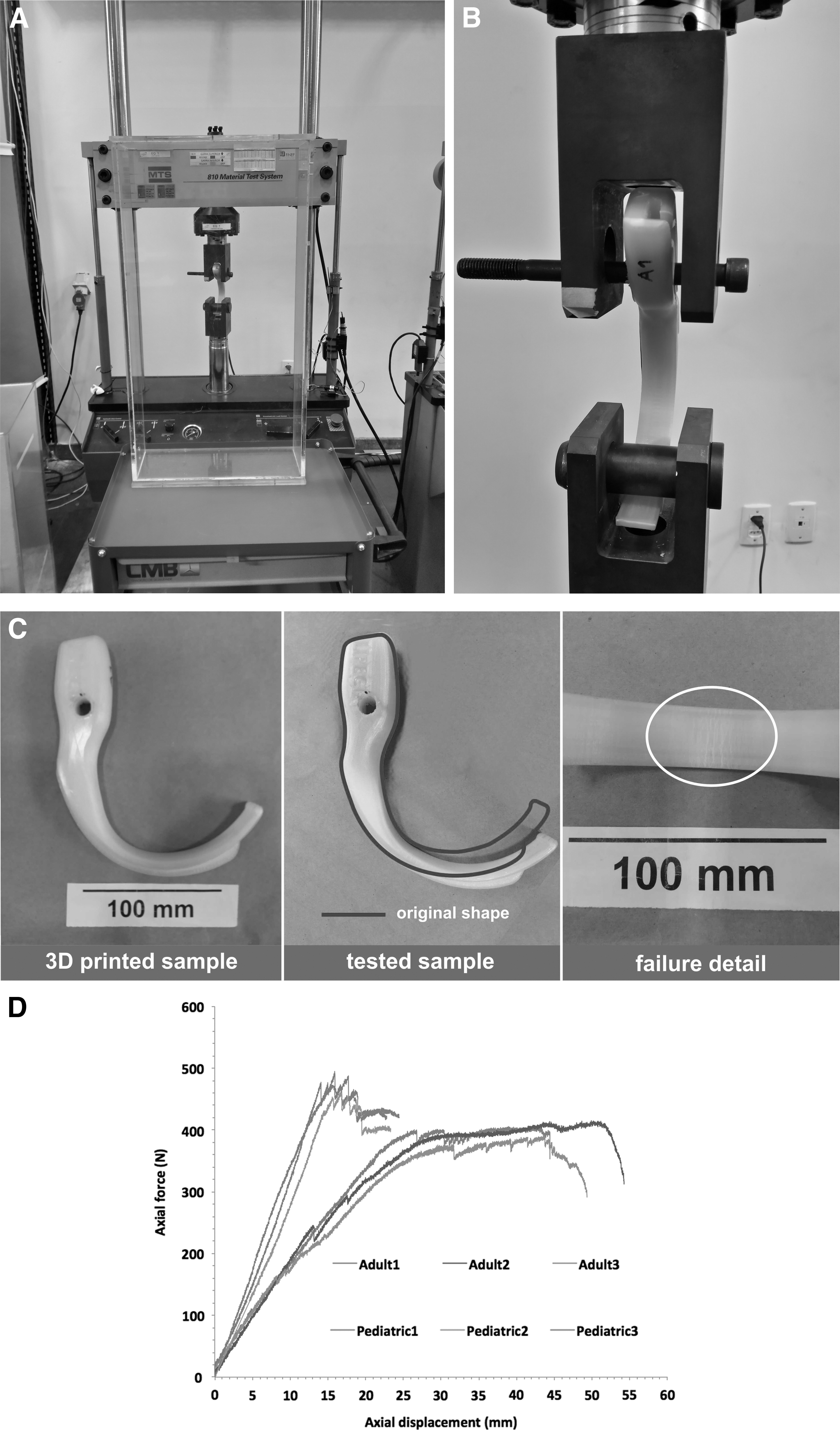
Mechanical essays.
Resistance Force Variability
CV, coefficient of variation; SD, standard deviation.
Training with senior anesthesiologists and resident physicians
Before the final tests in humans, the model was tested by senior anesthesiologists and resident physicians at the simulation center, with medical mannequins mimicking adult and pediatric anatomies. The laryngoscope proved to be suitable for both dimensional and shape aspects, enabling visualization of the airway anatomical structures. Compared with conventional models, the use of the 3D-printed artifact did not require any atypical effort from the anesthesiologist, because the blade comfortably slid into the mannequins' oral cavities and pharynxes. Furthermore, the application was demonstrated to be appropriate, as it provided the necessary configurations for obtaining the optimal image of the borescope camera. No failure resulting from the dissociation between the camera and the laryngoscope was reported.
Discussion
This article presents the manufacturing, design improvement, and evaluation of 3D-printed laryngoscopes, which are considered important tools for preventing the spread of infection in hospitals during SARS-CoV-2 pandemics.
Coronavirus disease 2019 (COVID-19) represents a risk to health care professionals. Thousands of people on the frontline have already been infected. The principle of “zero occupational infection” remains an achievable goal that all health systems must pursue in the face of a possible pandemic. 13
Singapore learned important lessons during the SARS outbreak in 2003. Forty-one percent of the 238 probable SARS cases in Singapore occurred among health care professionals. Therefore, hospital restraint efforts were implemented to curb the intrahospital transmission of SARS. These measures prevented unrestricted viral spread in hospitals, but put health care professionals in danger. 13 Similar to SARS, current evidence indicates that COVID-19 is transmitted primarily through respiratory droplets/aerosols. More than 3000 medical teams were infected in China in late February 2020. 14
Patients with COVID-19 may suffer myocardial injury and multiple organ failure, which causes hemodynamic instability coinciding with low oxygen saturation. 15 Patients have low serum oxygen levels, particularly those who are seriously ill. This makes intubation a major challenge, and rapid sequence induction is recommended. 15
Video laryngoscopes have significantly improved airway management and perioperative safety in most modern medical facilities. However, current models available on the market may have exorbitant prices, making them inaccessible in many locations around the world. Alternatively, new technologies arising from the Fourth Industrial Revolution (among them, we emphasize 3D printing) allow the manufacture of small products at affordable costs. The combination of 3D-printed components with electronic products, comprising an accessible medical device, can improve patient safety for the most vulnerable populations. Therefore, the proposed option is effective for pandemic situations. This solution was widely disseminated by AirAngel Blade and has been tested and published by other researchers.9,11,16,17
It is easy to find information on the use of 3D-printed video laryngoscopes. Unfortunately, accessible platforms that provide (1) standard printable blades and specific information about (2) which process parameters should be adopted, (3) which devices are compatible, and (4) how to integrate all the data are scarce. AirAngel Blade and LIPECIN, allowing free download of stereolithography files, are in consensus about the importance of democratization of AM during one of the most difficult periods in recent history.
Owing to cost restrictions, there are limited opportunities for training with video laryngoscopy in developing countries. The simplicity of use, high utility, and reliability of video laryngoscopes make them an appropriate technology for anesthesiologists in all configurations. Thus, the authors conducted this study with the purpose of publishing all the required information to perform a video laryngoscopy free of charge and making it accessible to medical teams worldwide. However, it is essential to state that we have overcome the first challenges of a slightly more complex trajectory. In the last few months, we prototyped, tested, and improved the artifact, in addition to investigating and ensuring the mechanical resistance to traction (through mechanical tests).
The prototypes will be used initially for clinical training with mannequins in a scenario of high demand for professionals who perform intubations. Owing to the worldwide pandemic situation and our open-source policy, the files for the construction of the device will be freely available worldwide to other medical training teams.
We are in the early stages of the submission process for the approval of the equipment and material by the Brazilian Health Regulatory Agency (ANVISA), aiming for at least authorization for single use. Therefore, future studies should focus on microbiological tests to validate the sterilization processes and determine the useful life of the equipment without evidence of polymeric degradation, as well as clinical trials.
However, considering the urgency of the sanitary situation, we decided not to wait for time-consuming bureaucratic approval to make our blade model and our related findings available. In this difficult pandemic scenario and in the future, we hope that by bringing our achievements to the public, other medical training programs can benefit. The process parameters used to produce the laryngoscopes gave rise to a tenfold security factor, considering the maximum forces typically applied during intubation. 18
Conclusions
A new design for printable laryngoscopes (with ideal 3D printing parameters) was developed and proved to afford efficient, low-cost (considering raw materials estimated between four and five dollars) and safe products. The artifacts attend to ergonomic factors for both anesthesiologist and patient, and mechanical essays evince that the printing parameters successfully provide the required resistance for clinical use. Therefore, for its features and facility of manufacture, it is an accessible alternative that, once available online and clinically tested, could be widespread for hospitals.
We believe that the recommendation for single use is prudent, but some tests will be carried out using 96% isopropyl alcohol, seeking to corroborate the existing data in the literature about the sterilization efficiency of this method. As an endorsement of a mindset change, we share all files to be manufactured anywhere in the globe, even though we are still in pre-clinical tests in Brazil. It is essential to spread the design of our products to the whole world, as many nations are struggling to save lives of countless patients who require intubation, reducing the probabilities of contamination of the medical frontline and minimizing potential injuries to the anatomical structures that can, unfortunately, occur during insertion of the cannulas without the accurate visualization that a video laryngoscope provides.
Footnotes
Acknowledgments
The authors would like to acknowledge UFCSPA for the Scholarships for Eduard Santos de Braga, Luis Fernando Marcelino Braga, and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for Doctorate Scholarship given to Andreia Gomes Aires. We thank Diego Pissaia Ramires for the valuable articulation work between the university and the hospital within the scope of the Innovation Center. The authors are also grateful for the allocation of artifacts in the LIPECIN platform, conducted by Patrick Carvalho Cabreira. We express gratitude to Luciano Amaro Junqueira Valerio, for his precise photographs, Simone Orlandi Introíni as photo editor, and, finally, all anesthesiology's staff for their valuable suggestions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.