
Abstract
Objective:
We aim to study the efficacy of acupuncture versus sham acupuncture in children with autism spectrum disorder.
Methods:
A single-blind randomized control trial was conducted in 50 children. These children were randomly assigned to the treatment group with tongue acupuncture (40 sessions over 8 weeks) or the control group (sham tongue acupuncture to nonacupoints in the tongue).
Results:
There was improvement in both the treatment and control groups in all assessed measures but more so in the treatment than in the control group: (1) eye–hand coordination, performance, and practical reasoning of Griffiths Mental Developmental Scale; (2) sensory-motor, social, affectual, language, and total score of Ritvo-Freeman Real Life Scale; (3) Comprehension Language age in the Reynell Language Developmental Scale; and (4) Total Score and Mental Age in Symbolic Play Test. The only statistically significant improvement in the treatment as compared to the control group was seen in self-care and cognition domains of the Functional Independence Measure for children.
Conclusions:
We had demonstrated that a short course of acupuncture had efficacy in improving various developmental and behavioral aspects of children with autism. The long-term efficacy in functional gain needs to be further explored.
Introduction
Acupuncture had been practiced in China for over 2 millennia. In Traditional Chinese acupuncture, nearly 400 acupoints on the body surface are interrelated to various functions. The surface acupoints were linked through 14 meridians to various organs or viscera of the human body. 12 The approach in Traditional Chinese Medicine (TCM) is a “holistic” approach with a philosophical background of balancing the yin and yang. The main objective of TCM was to improve health of body and mind by deblocking the flow of qi in the body. The pathophysiologic basis of TCM aimed to improve energy or body-flow or qi (de qui in Chinese]. The effect of acupuncture had been proven in animal and human studies to be due to direct neural stimulation, changes in neurotransmitters such as endorphin, immunological markers, or endocrinological signals. Thus, acupuncture is especially effective in chronic disorders, especially neurological ones. 12 In 2008, a cohort study in Hong Kong surveyed that about 40% of children with autism spectrum disorder (ASD) reported previous use of complementary and alternative medicine, with acupuncture being the most common form. 13
Tongue acupuncture is based on one of the most ancient medical books in China, The Yellow Emperor, and the idea that the tongue is the intersection site of all 14 meridians in the human body. Furthermore, according to The Yellow Emperor, the tongue is regarded as the window for diagnosis as it has rich nerve and blood supplies. Tongue acupuncture (TAC) was invented by Dr. J.G. Sun (one of the authors) based on experience in treating chronic neurological diseases. We postulate that there are acupoints in the tongue linked to the 14 meridians. The physiologic effect might be based on resignaling or potentiation of neural receptors through repeated stimulation. As the tongue is close to the brainstem and cerebellum, we postulate that stimulating tongue acupoints might augment the neural pathways connected to the motor/somatosensory cortex, resulting in improvement in motor function. We had demonstrated clinical efficacy of acupuncturing the surface or base of the tongue in specific acupoints in improving various functional modalities in patients with chronic neurological disorders such as stroke, cerebral palsy, drooling problems, and ASD. 14 –41
In our experience, the TCM approach for autism is more holistic. Autism is part of a spectrum with lower intelligence, and the approach to autism is considered as lower intelligence due to “Heart meridian and Kidney meridian yin–yang imbalance,” resulting in communication problems and “Liver meridian yin–yang imbalance” leading to behavioral problems.
Our objective is to use a different approach in management of autism and to use an evidence-based approach to assess the efficacy of alternative medicine in improving the functional status of these children.
The objective is to study the efficacy of a short intensive course of acupuncture versus sham acupuncture in improving the overall functional status of children with autism.
Methodology
A total of 50 autism children were recruited. The male to female ratio is 7.3:1. The age ranged between 3 and 11 years. All children had a comprehensive neurological and developmental evaluation by the first author. The diagnosis of autism was made according to the criteria of the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) 42 and Autism Diagnostic Interview-Revised. 43 Children with associated neurological disorders or epilepsy were excluded.
All the children and parents were observed in an assessment setting and a semistructured diagnostic interview with the parents were made. The diagnosis of autism was made if it satisfied a score greater than 30 in the Childhood Autism Rating Scale (CARS). 44 The range of possible scores was 0–60. For CARS, those with higher values were more severe in the degree of autism.
The children were randomized into two groups: control group (C) versus tongue acupuncture treatment group (T). The control group received sham acupuncture only. In both groups, the conventional educational and behavior model for autistic children was continued.
Assessment and Treatment
All 50 children continued their conventional autism program as it is unethical to deprive them of the usual training while recruited into the study. Randomization was achieved by computer generation of C or T group by an independent statistician. Twenty-five children were randomly assigned to receive tongue acupuncture. The parents and assessors were blind to allocation into the C or T group. The outcome measures were performed by independent trained research assistants who were blinded to the treatment or control group. The acupuncturist responsible for providing intervention and sham acupuncture in this study was not blind to the study.
The clinical and demographic characteristic of C and T groups is shown in Table 1. The children were matched by mental age, social class, severity of autism using CARS score, and functional status using the Functional Independence measure of children (WeeFIM®). 45,46 There was no statistically significant difference in the demographic measures, severity of autism (graded by CARS, Ritvo-Freeman Real Life Scale), general developmental profile (Griffiths Mental Developmental Scale), language profile (Reynell Language Developmental Scale, Symbolic Play Test) and functional independence level (using WeeFIM).
SD, standard deviation; y, years; m, months.
All children in both groups were assessed before acupuncture (week 0) and after acupuncture (week 9).
Assessment tools
The following outcome measures were used before and after treatment in both T and C. Griffiths Mental Developmental Scale (GMDS)—six subscales (Locomotor, Personal-Social, Hearing & Speech, Eye–Hand coordination, Performance, Practical reasoning).
47
Ritvo-Freeman Real Life Scale (RFRLS)—Sensory-Motor, Social, Affectual, Sensory Response, Language.
48
Reynell Language Developmental Scale (RLDS)—Comprehension score, Comprehension Age, Expression score, Expression Age.
49
Symbolic Play Test (SPT)—total score and Mental Age.
50
Functional Independence Measure for children (WeeFIM)—three domains of mobility, self-care, and cognition. WeeFIM consisted of 18 questions concerning on the Functional Independence Measure for children. The scores are from 1 to 7, with 0 meaning complete dependence and 7 meaning total independence. The total score is 126 (18 items × 7).
45,46
Methods
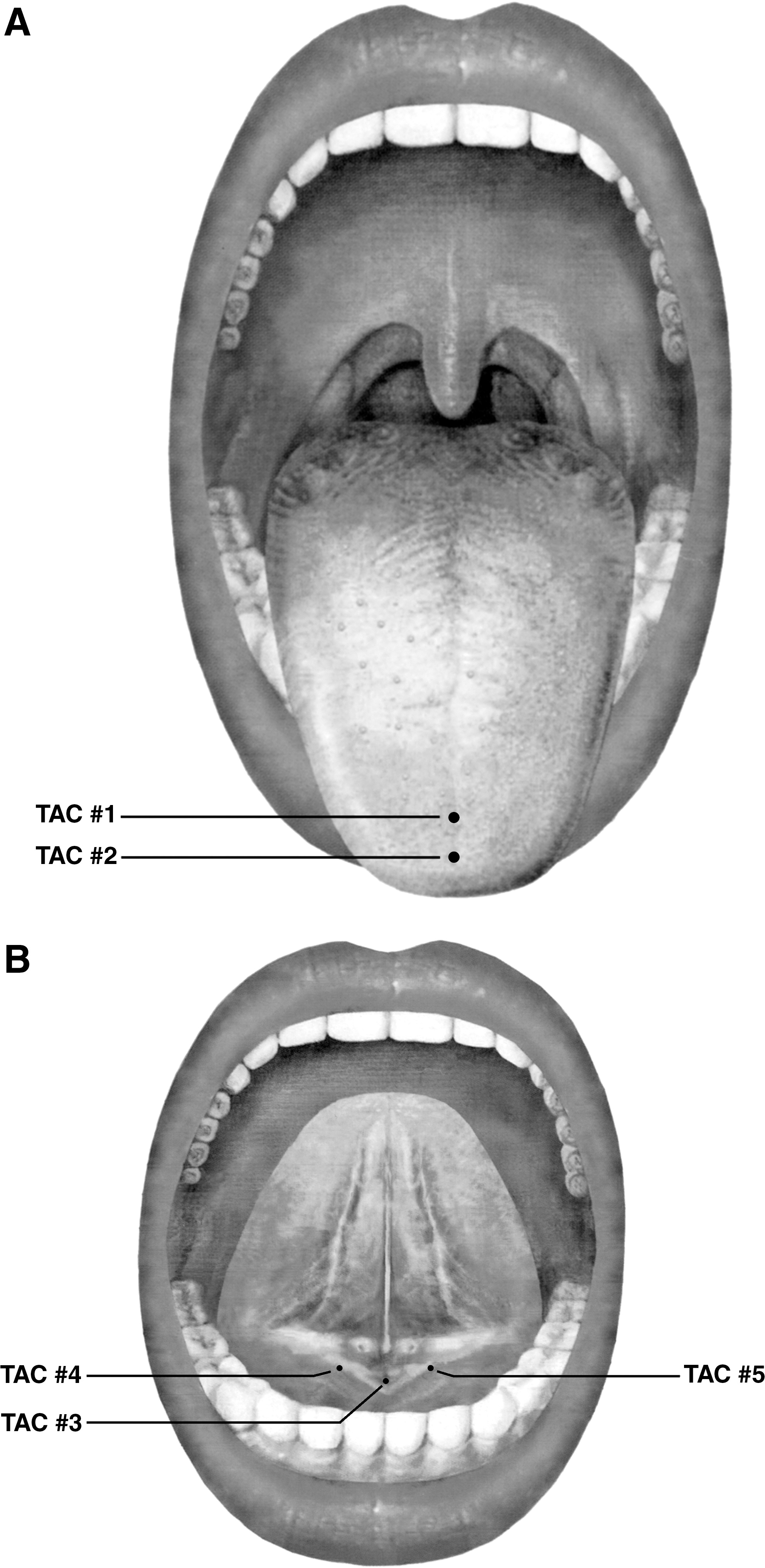
TAC consisted of a total course of 40 sessions, with 5 sessions per week over 8 weeks. TAC was applied to 5 specific acupoints on the tongue daily by Dr. Sun using a sterile disposable 0.3 × 4-cm acupuncture needle (made in China; HWA–TO).
TAC was applied to five specific acupoints on the tongue daily using a sterile disposable 0.3 × 4-cm acupuncture needle (made in China; HWA–TO). Two (2) acupoints at the center of the tongue surface (TAC #1 = Run Ze’ [1 cm from the tongue tip] and TAC #2 = Guan Zhu” [0.5 cm from tongue tip]) and three acupoints at the bottom of the tongue (i.e., sublingual region) (TAC #3 = Tian Men” [center of tongue base] and TAC #4 and TAC #5 = Di You' [0.5 cm from tongue base on both sides]) were punctured. The tongue surface TAC #1 was punctured by a1-cm depth obliquely and TAC #2 about 0.3-cm depth obliquely. The bottom of the tongue TAC #3 was punctured perpendicularly by 0.5–1-cm depth and TAC #4 and #5 by 0.5-cm depth perpendicularly (Fig. 1A and B).
(
The total acupuncture procedure lasted for <15 seconds. No sedation was required. The child sat on the mother's lap with the head tilted around 45 degrees upward. Sterile gauze was used to pick up and station the tongue with the examiner's left hand. The child was encouraged to open up his/her mouth, which was the usual mouth posture of those with persistent drooling. Quick and accurate insertion into five acupoints was performed with the examiner's right hand. Most children tolerated the procedure well.
Sham Acupuncture
This was performed with a sterile acupuncture needle in five sham points in the tongue. The five points are same as those used in the C. The procedure was same as in the C. The only difference is the practitioner is using the rough end of the acupuncture needle to touch the five points in stead of using the sharp end to puncture into the tongue. The parents, children, assessors, and school teachers were blind to whether the treatment given was real or sham.
A total of 40 sessions (daily sessions) for a total course of 8 weeks were administered. The children attended our Tongue Acupuncture Research Clinic on an ambulatory basis. They were discharged immediately after the acupuncture session.
Side-Effects
The children will be monitored for side-effects and the parents were asked to report on any change. A questionnaire on any side-effect was administered after the course of TAC treatment.
Statistical Analysis
All data were collected before the codes of treatment were broken. The data were analyzed with the Wilcoxon Rank Sum Test. P values for all statistical tests were two-tailed.
Ethical Approval
This study was approved by the Ethics Committee of the Faculty of Medicine of the University of Hong Kong. The parents were informed about the methodology and written consent was obtained.
Results
1. Griffiths Mental Developmental Scale (GMDS; Table 2)
Both C and T groups have statistically significant improvement after treatment in the following features: Locomotor (p-value = 0.004 and 0.022 in C and T groups, respectively), Personal-Social (p-value < 0.0005 in both groups), Hearing & Speech (p-value < 0.0005 in C group and p-value = 0.001 in T group), Eye & Hand Coordination (p-value = 0.005 and <0.0005 in C and T groups, respectively), Performance (p-value = 0.001 and <0.0005 respectively), Practical Reasoning (p-value = 0.008 and 0.002, respectively), and Total (p-value < 0.0005 in both groups).
Significant difference within groups.
Bold p-values showed more improvement in Treatment than Control group.
SD, standard deviation; y, years; m, months.
2. Ritvo-Freeman Real Life Scale (RFRLS; Table 2)
The C group had statistically significant improvement after treatment in the following features: Affectual (p-value = 0.03), Sensory Responses (p-value < 0.0005), Language (p-value = 0.001), and Total (p-value = 0.032). The T group has statistically significant improvement after treatment in the following features: Sensory Motor (p-value = 0.013), Affectual (p-value < 0.0005), Sensory Responses (p-value =0.007), Language (p-value < 0.0005), and Total (p-value <0.0005).
3. Reynell Language Developmental Scale (RLDS) (Table 2)
The C group had statistically significant improvement after treatment in the following features: Comprehension Score (p-value = 0.007), Expression Score (p-value <0.0005), and Expression Age (p-value = 0.001). The T group had statistically significant improvement after treatment in the following features: Comprehension Score (p-value =0.007), Comprehension Age (p-value < 0.0005), Expression Score (p-value < 0.0005), and Expression Age (p-value =0.001).
4. Symbolic Play Test (Table 2)
The C and T groups have statistically significant improvement after treatment in the following features: Score (p-value = 0.004 and p-value < 0.0005 in C and T groups, respectively) and Mental Age (p-value = 0.004 and p-value < 0.0005 in the C and T groups, respectively).
5. WeeFIM (total score) (Table 2)
The C group has statistically significant improvement after treatment in the following features: Self-Care (p-value =0.009), Mobility (p-value = 0.009), and Total (p-value = 0.002). The T group has statistically significant improvement after treatment in the following features: Self-Care (p-value< 0.0005), Mobility (p-value < 0.0005), Cognition (p-value< 0.0005), and Total (p-value < 0.0005).
The T group has statistically significant improvement compared with the C group in the following features: Self-Care (p-value < 0.0005); Cognition (p-value = 0.006), and Total (p-value < 0.0005).
WeeFIM (Functional Quotient)
The C group has statistically significant improvement after treatment in the following features: Self-Care (p-value = 0.01) and Total (p-value = 0.011). The T group has statistically significant improvement after treatment in the following features: Self-Care (p-value < 0.0005), Mobility (p-value = 0.005), Cognition (p-value < 0.0005), and Total (p-value < 0.0005). The T group has statistically significant improvement as compared with the C group in the following features: Self-Care (p-value = 0.007); Cognition (p-value < 0.0005), and Total (p-value < 0.0005).
Comparison of difference in scoring of treatment and control groups (Table 3)
Thus, there was improvement in both T and C groups, with all assessed measures (1-4); however, more so in the T than C group, as shown by the bolded p-values in Table 2: in GMDS (eye–hand coordination, performance, and practical reasoning); RFRLS (sensory-motor, social, affectual, and language); RLDS (Comprehension Score and Comprehension Age); Symbolic Play Test (Total Score and Mental Age).
Significant difference between Control and Treatment groups, m, months; y, years.
However, only the WeeFIM scores and functional quotient (self-care and cognition) showed a statistically significant difference between the T and C groups.
Side-effects
None of the children developed any side-effects. Initial crying for fear and possible minor pain occurred in the first few sessions. However, most children adapted easily and tolerated the technique well. There was no default in both groups.
Discussion
In this pilot study of assessing the efficacy of alternative medicine (acupuncture) in children with autism, we have demonstrated by integrating TCM philosophy with Western scientific methodology by using a randomized controlled trial using real versus sham acupuncture that there was improvement in various functional status in children with autism in both treatment and sham acupuncture groups, including language, fine motor, performance, social, and cognition.
As children with autism have heterogeneous manifestations in core symptoms such as language, social communication, and repetitive or ritualistic behavior, and it is quite difficult to repeatedly reassess their progress with weekly assessment and long-term follow-up, we have thus decided to perform baseline (pre-) and postacupuncture assessment immediately after the 8-week course to observe for any immediate effect. Our aim was to observe whether there is any efficacy of an intensive course of acupuncture in improving symptoms of autism. Whether any effect observed will be sustained or even carry on for a longer term will require another research study to prove long-term efficacy. We are performing this pilot study with preselected tongue acupoints as a pilot study as we are the first pioneer group to study the tongue as a microsystem in acupuncture.
We had also demonstrated in another randomized controlled trial using a positron emission tomography scan of the brain as one of the outcome measures for acupuncture versus no-acupuncture that there was improvement in some core features in autism. 38
In this study, though both treatment and control groups showed a significant improvement in all the assessed measures used including developmental (GMDS), behavioral (RFRLS), language (RLDS), and mental age (Symbolic Play Test), we found that those enrolled for real acupuncture had significantly improved total scores and functional quotient in WeeFIM. Though there had not been a validated outcome measure for use in interventional or therapeutic studies specific for autism, one of the outcome measures selected in this study (apart from the profile of cognition, language, social) might have explained the significant difference as WeeFIM is a functional score for children and acupuncture had been long used as a holistic medicine to improve function for both health and disease.
The fact that both real and sham acupuncture groups showed improvement in all outcome measures using the same 5 acupoints though there is no actual needle puncturing in the sham group might be explained by the partial effect of possible touching of the acupoints of surrounding sites also producing a similar clinical effect. This might explain the “placebo effect,” which has been harshly criticized for so-called clinical efficacy in most acupuncture research. For future studies, we might use nontouching of acupoints in the sham group, as children with autism are usually unaware of whether they were punctured or not.
As we are the first researchers in performing pilot studies of the efficacy of acupuncture in chronic neurological diseases in children (e.g., cerebral palsy, drooling, autism) using randomized controlled trials, 49 –54 we hope that our selection of acupoints both for the tongue or body (Fig. 1A and B) can serve as a basis for launching worldwide multicenter trials for the integration of acupuncture similar to drug trials for treating autism.
In a recent systemic review on the physiologic rationale of acupuncture from clinical trials, 55 many acupuncture trials failed to offer a meaningful rationale for acupuncture. Proposing a rationale can help other investigators to develop and test a causal hypothesis, choose an appropriate control, and rule out placebo effects. We hypothesize that autism is due to imbalance of the Heart, Kidney, and Liver meridians according to TCM theory and our selection of acupoints had been based on this assumption. However, as the basic path physiology and underlying causes for autism is unknown, we can only postulate that there might be derangement of neurochemical mechanism, and that acupuncture might be able to restore the derangement by linking up various neuroarchitectures.
Acupuncture is basically a skill learned through years of experience and practice like any surgical techniques, by personal trial and error. Thus, it is difficult to standardize acupuncture skills across centers in conducting multicenter trials. Moreover, the often used research acupuncture techniques such as electrical acupuncture or laser acupuncture techniques, though relatively better standardized as to the frequency used, might not be good research technique as the positive versus negative stimulation of the relevant acupoints are essential to demonstrate any efficacy in the TCM concept. However, if we could prove that acupuncture can serve as an adjunctive treatment modality to Western medicine in the field of multidisciplinary management of chronic neurological disorders, it might be possible to use portable bioacupuncture machines to specific body acupoints with standardization of intensity and frequency of electrical acupuncture in order to assess intermediate and even longer-term efficacy of other acupuncture techniques. Of course, the selection of acupoints is critical in assessing any subtle and yet positive outcome.
It is difficult to launch multicenter trials with any interventional skills like acupuncture because the standardization of the technique and experience with handling autistic children are essential. Thus, for future studies of efficacy of acupuncture for autism, one can target subgroups of ASD with core features or other specific features such as attention, cognition, hyperactivity, and aggressiveness with specific targeted outcome measures. Otherwise, one should target a particular subgroup at a selected mental age range, meanwhile, using sophisticated tests for assessing abstract thinking, mind-reading or even using neuropsychological tests, provided the children were cooperative enough to complete the battery of tests. However, this might be unrealistic in autistic children with lower mentality. One can then target high-functioning autism or even Asperger syndrome. However, as early intervention might improve the developmental trajectory of autism children, one can also aim at starting acupuncture at an earlier age as soon as possible after the diagnosis, which is around 2–3 years, to augment the Western interventional model of training.
For future studies, we planned to include some other tests to assess the efficacy of improvement of neuropsychological perspective such as attention, because analysis of reports from schoolteachers in this cohort showed improvement in curiosity and imagination for some of those who received real acupuncture, although this was too subjective to analyze in a randomized controlled trial. Moreover, conventional tests for assessing outcome of autism might have their own limitations, as there is a lack of outcome measures developed or validated for therapeutic trials in alternative medicine in disorders such as autism. Thus, we still think that using an integrated treatment model for autism is feasible, with acupuncture augmenting early intervention and using a Western model of outcome measures to assess for short-tem and long-term efficacy.
In the present study, conventional outcome measures used for children with neurodevelopmental disorders were selected with the hope of analyzing the functional outcome according to the holistic concept of alternative medicine. There was no other choice because it was really difficult to get these autistic children to comply or sit down to be assessed with repeated sophisticated test batteries. Thus, it was not possible to repeatedly reassess these two groups of children for a longer duration of follow-up to assess for sustainability of acupuncture.
In the future, with the encouraging result of these pilot evidence-based studies using acupuncture, we should aim at studying acupuncture as a novel pharmacotherapy for modulating neurotransmitters or neurochemicals in these children. The mechanism of action with animal models could be proven. Unfortunately, there is no single animal model for all the core features of autism to test this hypothesis, though acupuncture had been a relatively “noninvasive” therapeutic technique used by veterinarians for animals such as the rabbit, dog, cat, cow, sheep, and horses in pain and also in animal models for proving the endorphin theory.
The aim should now be at focused and targeted features of ASD and possibly to document efficacy with targeted subgroups with different mental ages. Currently, the authors are also conducting repeated courses of acupuncture for the pilot autism cases. The authors observed overall improvement in intellectual, social, and communication abilities in these children rather than just pure behavioral improvement. In future research, the authors still need to assess other parameters, such as factors contributing to efficacy, and intermediate and long-term efficacy.
Footnotes
Acknowledgments
We wish to thank the nursing team of Children's Habilitation Institute of the Duchess of Kent Children's Hospital, and Wilfred Wong, M.Med.Sc. for statistical analysis.
This article had been presented at the following meeting: 2007 Annual Conference of the Society for Acupuncture Research: The Status and Future of Acupuncture Research: 10 Years Post-NIH Consensus Conference 2007 (November 9–11) at University of Maryland at Baltimore, Baltimore, MD.
Disclosure Statement
No competing financial interests exist.
This randomized controlled trial was registered with the Clinical