
Abstract


Introduction
Beginning in 1999, the Institute for Applied Dermatology (IAD), in Kerala's Northernmost City of Kasaragod, started developing new treatments for skin care, integrating traditional Ayurvedic practices with biomedicine. Some years later in 2004, the Global Programme for the Elimination of Lymphatic Filariasis recommended exploring local health traditions of skin care in the management of LF. 2 In particular, Ryan discussed a low-cost treatment paradigm using traditional Indian medicines and yoga, suitable for rural communities. 3 At that time, IAD had already been engaged in such a program for a number of years, and was looking for collaborators. This led to an exchange and incorporation of Ryan's recommendations into our work. Subsequently, he closely mentored the whole program. Results obtained 4 were very promising (see Figure above Introduction), stimulating editorials in two journals. 5,6 The degree of reduction in lymphedema so obtained, illustrated in the Figure above the Introduction, represents a significant advance in treatment success.
Methods
Patients with LF are examined by a team of biomedical, Ayurvedic, and yoga medicine experts, who assess both patient and pathology from all three perspectives. Status of limb and skin are recorded photographically, and baseline limb volume measured. As per our recent article, 7 dosha constitution and specific pathological imbalances are determined to select herbalized oils and solutions to be administered. All patients attended two counseling sessions (baseline and admission counseling) before being inducted into the treatment. A counselor spends at least 1 hour during each counseling session educating the patient that the treatment is for life and that they need to spend at least 1½ hours daily for the treatment.
Patients are hospitalized for 2 weeks' initial treatment, so they and a family member can be trained in all details of home treatment. Involving another family member in the therapy procedures is an aspect of the program worth particular mention. It brings several benefits: being empowered to assist encourages him or her to feel involved in the loved one's recovery; it improves patient cooperation in the lengthy procedures; and it reintegrates patients with their family and friends, helping resolve many of LF's social issues.
Patients are advised to keep their foot or feet elevated as much as possible, in the hospital and after they return home. Skin care measures include soap and water wash by the family member, and Ayurvedic herbal phanta solution to improve skin health. Associated entry points caused by fungal intertrigo, eczema, or infected ulcers receive appropriate biomedical treatment.
Lymph drainage is effected by a combination of yoga exercises (Fig. 1) and Indian manual lymph drainage (IMLD). Nine yoga exercises (asanas) and six special breathing techniques (pranayamas) are practiced before IMLD, and eight asanas and six pranayamas afterward. IMLD involves inguinal and popliteal lymph node drainage, followed by non-oil massage (unmardhana), and then oil massage in the opposite direction to hair growth (udhwarthana). Choice of oil is patient specific and depends on dosha (primary life forces) imbalance (vikriti—local skin pathology). 7 For patients with kapha (one of the three primary life forces, which is represented by characteristics such as Oily, Cool, Heavy, Slow, Sticky, and Stability) dosha imbalances, nalpamaradi thailam was used for massage. This herbalized oil was prepared by boiling sesame oil with the paste of nalpamara as described in traditional texts. 8 Nalpamara is a mnemonic used for four latex-producing plants. They are Ficus arnottiana stem bark (plaksa), F. bengalensis stem bark (nyagrodha) (Fig. 2), F. religiosa stem bark (aswatha), and F. glomerata stem bark (udumbara). Other plant ingredients in this oil are Terminalia chebula fruit without seeds (haritaki), T. bellirica fruit without seeds (vibhitaki), and Emblica officinalis fruit without seeds (amalaki), Santalum album stem (chandana), Vetiveria zizanioides root (sevya), and Saussurea lappa C.B. Clarke root (kusta). An alternative oil used is pinda thailam, made from the Madhuka indica flower (Madhuka), bee's wax (madhuchchista), Shorea robusta gum resin (sarja rasa), and Hemidesmus indicus root (sariva). Finally, patients presenting with firm, nonpitting lymphedema that records little or no change in girth measurements following overnight elevation (also called organized limbs in the sense that the term is used in wound healing for phenomena such as angiogenesis and fibrosis) are given sarshapa thailam, an oil extracted from Brassica campestris seed (sarshapa). It has kaphamedohara action 9 (i.e., it helps to relieve hardening [caused by vitiation of kapha dosha and medo dhathu]). Medo dhathu is comparable to adipose tissue. In organized limbs, increased deposition of adipose tissues are often observed.

A patient with lymphedema performing yoga exercises (gomukha asana) at home. (Photo by Duncan Murray).

Ficus bengalensis (nyagrodha) tree bearing hypanthodium inflorescence. The bark of this tree is used in nalpamaradi oil used for Indian manual lymph drainage. (Photo by Guruprasad Aggithaya).
At this point, patients with hardened limbs showing nonpitting edema (organized limbs) receive Ayurvedic heat treatment of the affected limb (Ekanga swedana, Fig. 3) during the initial 14 days of hospitalization. In this medically supervised procedure, herbalized steam is passed through a pipe directly to the area concerned (Nadi sweda). An additional layer of oil used for massage (udhwarthana) is applied over the area before spraying the herbalized steam. Ayurveda classifies some 13 varieties of swedana or induced sweating treatment. In this procedure, a mixture of roots of 10 herbs (dasha mula) is boiled in water. The herbs used in this mixture are Aegle marmelos root (bilwa), Clerodendrum phlomidis root (agnimantha), Oroxylum indicum root (syonaka), Gmelina arborea root (kasmari), Radermachera xylocarpa root (patala), Flemingia macrophylla root (salaparni), Desmodium velutinum root (prshni parni), Solanum anguivi root (bruhati), Solanum surattense root (kantakari), and Tribulus terrestris root (gokshura).

An Ayurvedic doctor performing induced sweating treatment after Indian manual lymph drainage. This is a supervised procedure given only in the hospital. (Photo by Duncan Murray).
Finally, long stretch compression bandages are applied, followed by post-IMLD yoga. Compression bandages were not used traditionally in Ayurvedic medicine for lymphedema. They are a later addition to the treatment imported from lymphology and physiotherapy disciplines during the process of developing an integrative protocol.
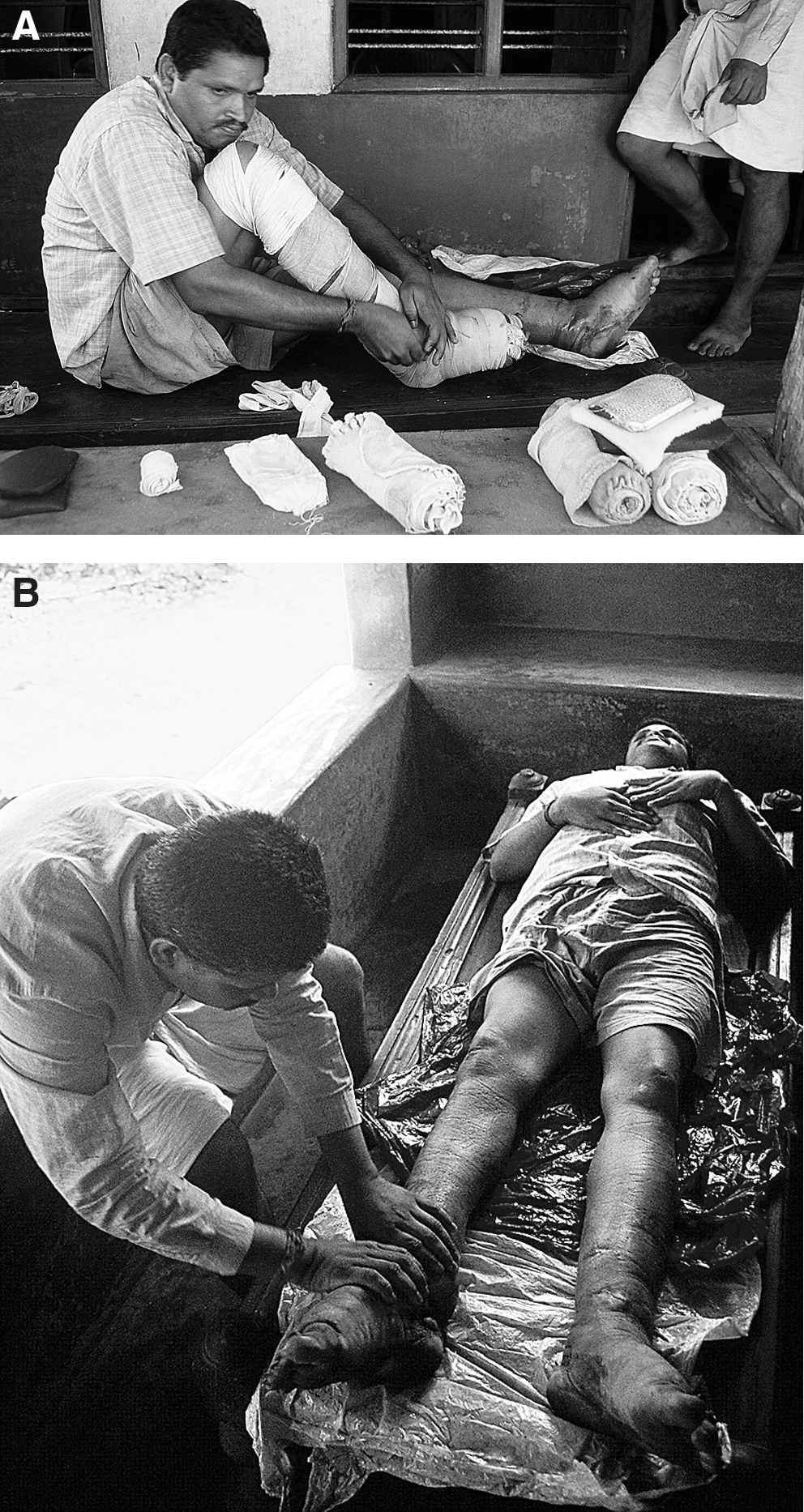
On returning home, patients are asked to perform these procedures in the above sequence daily. This should present no problem, since “treatment methods are designed to fit any environment, academic, medical center, or remote village. In addition, treatment components are easily provided after brief training, culturally sensitive, capable of widespread compliance, and cheap.” 5 Bandages are the most expensive components of the entire treatment (Fig. 4A and B). Patients are prescribed two Ayurvedic skin care medicines to be taken orally for 6 months, namely, maha manjistadi kashayam (MMQ) and kanchanara guggulu (KG). MMQ is an herbal decoction that has 46 ingredients. The major herbs used are Rubia cordifolia Linn root (manjista) and Cyperus rotundus Linn root (musta). KG is in tablet form, containing 11 ingredients; the major ones are Bauhinia variegata stem bark (kanchanara twak) and Commiphora mukul gum resin (guggulu). As is usual with Ayurvedic prescriptions, patients are asked to observe dietary restrictions while on the medication. 4 In general, the restricted dietary items were slow to digest (guru ahara), sour items (amla), nonvegetarian food, milk, and milk products.
Follow-up appointments are scheduled 1 month and 3 months after discharge. Patients demonstrate treatment components being performed at home, including all yoga exercises to help perfect the procedures. All outcome measures are recorded each time. The overall treatment program thus consists of: 14 days' initial treatment with training either as outpatient or inpatient as appropriate. Oral medications/diet restrictions for the initial 6 months. Yoga, compression, and massage need to be continued for life.
Four hundred and sixty-seven (467) patients having lymphedema of one or both lower limbs (512 limbs) of any duration with ability to withstand the variety of yoga exercises were recruited for the integrative treatment over the period October 2003–June 2008. Patients presenting with acute dermatolymphangioadenitis were excluded. Our Institutional Ethics Committee gave the clearance for the study in 2004. The Ayurvedic doctor recruited the patients for the study and selected the Ayurvedic herbal medicines used for each patient as explained in Narahari et al. 7 Patients came from eight different provinces of India, often traveling more than 1 day to reach Kasaragod. The study was conducted in the outpatient department and a private hospital in Kasaragod where IAD admits its patients needing inpatient care. Twenty-six (26) patients were irregular for follow-up.
Outcome measures used for assessments
In addition to limb volume changes, lymphedema results in changes in skin color, thickness, and quality, and secondary infections. All these are assessed: skin color, skinfold thickness, degree of warting, number of entry points for secondary infections, frequency of inflammatory (“fever”) episodes, and extent of antibiotic consumption. Limb volume changes are measured by water volume displacement (the “gold standard”), supplemented by circumference measures at eight points along the limb: metatarsal, midfoot, ankle, end of calf, maximum calf bulk, patellar region, midthigh, and maximum bulk on standing.
Results obtained following two-step cluster analysis are shown in Figure 5. It is an automatic analysis done by SPSS 16 (SPSS Inc., Chicago, IL) when it considers that data available are large and sufficient. The “two-step cluster analysis” procedure is an exploratory tool designed to reveal natural groupings (or clusters) within a dataset that would otherwise not be apparent. The algorithm employed by this procedure has several desirable features that differentiate it from traditional clustering techniques: SPSS 16 classified data revealed 343 limbs as small; 146 limbs as large; 23 limbs as “outlier cluster” (medical records are maintained as number of limbs). We have not yet recognized a treatment failure in these 512 lymphedematous limbs as long as patients are cooperative with the treatment program. The adverse events observed included contact dermatitis to nalpamaradi oil used for IMLD in five limbs. About 10% of patients developed scattered sterile pustules over the massaged limbs. Repeated-measurements analysis of variance showed the volume reduction of 22.3% on 14th day, 30.8% on 45th day, and 41.6% on 90th day of treatment for large limbs; for small limbs it was 11.1%, 24.3%, and 31.8%, respectively. All patients have improved, but previous surgery compromises treatment outcome. Improvement depends on compliance, but since patient cooperation is a prerequisite for acceptance on the program, it tends to be good because of repeated counseling sessions.

Two-step cluster analysis of reduction in total volume by water displacement method for small and large limbs during the initial 3 months of treatment. Upper segmented curve represents large limbs and lower segmented curve represents small limbs.
LF is a common tropical disease. The efficacy of these Ayurvedic treatments now has a strong evidence base, making them the subject of discussion internationally. For example, the Canadian health department has discussed this treatment for the benefit of their lymphedema patients' group. 10
Footnotes
Acknowledgments
We would like to acknowledge the mentoring work of Professor Terence J Ryan, Emeritus professor of dermatology, University of Oxford Medical School, UK in helping guide treatment protocols. We would also like to thank Kerala State council for science, technology, and environment, Thiruvananthapuram for their financial assistance for this study; Dr. K. Muralidharan, senior scientist and statistician, Central Plantation Crops Research Institute, Kasaragod for assisting in developing the patient data base over SPSS 16 and its analysis; and Alex Hankey, Ph.D., for his editorial assistance.