
Abstract
Background:
Falls and fall-related injuries are a major public health concern, a financial challenge for health care providers, and critical issues for older adults. Poor balance and limited mobility are major risk factors for falls.
Objective:
The purpose of this study was to examine effects of Feldenkrais exercises in improving balance, mobility, and balance confidence in older adults.
Methods:
Participants (N = 47, mean age 75.6) were randomly assigned to a Feldenkrais group (FG, n = 25) or to a control group (CG, n = 22). The FG group attended a 5-week Feldenkrais program, 60 minutes three times per week, while the CG group was a waitlist control. The outcome measures were balance (tandem stance), mobility (Timed Up and Go), gait characteristics (GAITRite Walkway System), balance confidence (Balance Confidence Scale; ABC), and fear of falling (Falls Efficacy Scale). Pre- and post-tests were conducted.
Results:
After completion of the program, balance (p = 0.030) and mobility (p = 0.042) increased while fear of falling (p = 0.042) decreased significantly for the FG group. No other significant changes were observed. However, participants of the FG group showed improvements in balance confidence (p = 0.054) and mobility while performing concurrently a cognitive task (p = 0.067).
Conclusions:
These results indicate that Feldenkrais exercises are an effective way to improve balance and mobility, and thus offer an alternative method to help offset age-related declines in mobility and reduce the risk of falling among community-dwelling older adults. A long-term follow-up study of balance and mobility is warranted. Further research is needed to identify whether Feldenkrais exercises may impact cognitive processes.
Introduction
A variety of environmental, physical, and behavioral risk factors for falls have been identified. Many of these risk factors are associated with age-related changes, such as loss of muscle mass, degenerative transformations of the musculoskeletal system, or the onset of chronic diseases and their aftereffects. 6 –12 Poor balance, limited mobility, and fear of falling are frequently mentioned as major risk factors for falls. 6,7,13,14 Maintaining balance and mobility is critical for older adults to sustain independent living and to avoid falls. 15,16
Balance training and exercise programs have been shown to facilitate improvement in balance and mobility. 17 –21 However, the low exercise participation rates of older adults in these programs indicates that many older adults are not attracted to these programs, especially if fear of falling is an issue. 22 –25 Thus, there is a continuing need to identify interventions that can attract older adults who are not inclined to participate in conventional exercise programs and that can improve balance and mobility as well as reduce falls, and fear of falling.
In recent years, the interest in mind–body interventions for older adults increased due to the noninvasive approach and the potential health benefits of these exercise strategies 26 –28 One option in the search for new intervention approaches is the Feldenkrais Method (FM). The FM is a mind–body exercise that involves gentle movements carried out in a quiet, noncompetitive environment. Two major techniques are used in FM activities, Awareness Through Movement (ATM) and Functional Integration (FI). Both approaches focus on mind–body relationships and involve a setting in which the teacher guides the individual through a variety of sequences of movements. In the former (ATM), individuals learn through verbally guided movement while in the latter (FI), individuals learn through the experience of manipulation which involves gentle, noninvasive touch. Most Feldenkrais interventions that examined gait, balance, as well as a variety of well-being factors have reported favorable outcomes. 29 –32 However, most of these studies involved small sample sizes, lacked appropriate control groups, and were conducted with special populations (e.g., patients with Parkinson's disease, multiple sclerosis, etc.). In addition, the length of the interventions along with the frequency and duration of sessions were not always reported and varied widely (e.g., a single 30-minute session to 30 sessions within 13 weeks). Thus, although most Feldenkrais studies have reported positive outcomes, it is not clear that these findings can be generalized to other populations (e.g., older adults, healthy individuals). The purpose of this study was to examine the effects of a five-week Feldenkrais Awareness Through Movement (ATM) intervention on balance, balance confidence, gait, and mobility in community-dwelling older adults.
Methods
This stratified randomized controlled trial was conducted with 47 older adults in Columbia, SC. The study included two groups: a Feldenkrais intervention (FG) and a control group (waitlist) (CG). The Feldenkrais intervention was carried out in the Arnold School of Public Health at the University of South Carolina. Participants were relatively healthy independently living older adults (age ≥65) recruited from a variety of sources including senior centers, churches, and retirement communities. The study was conducted with two cohorts (I, II) (Fig. 1).
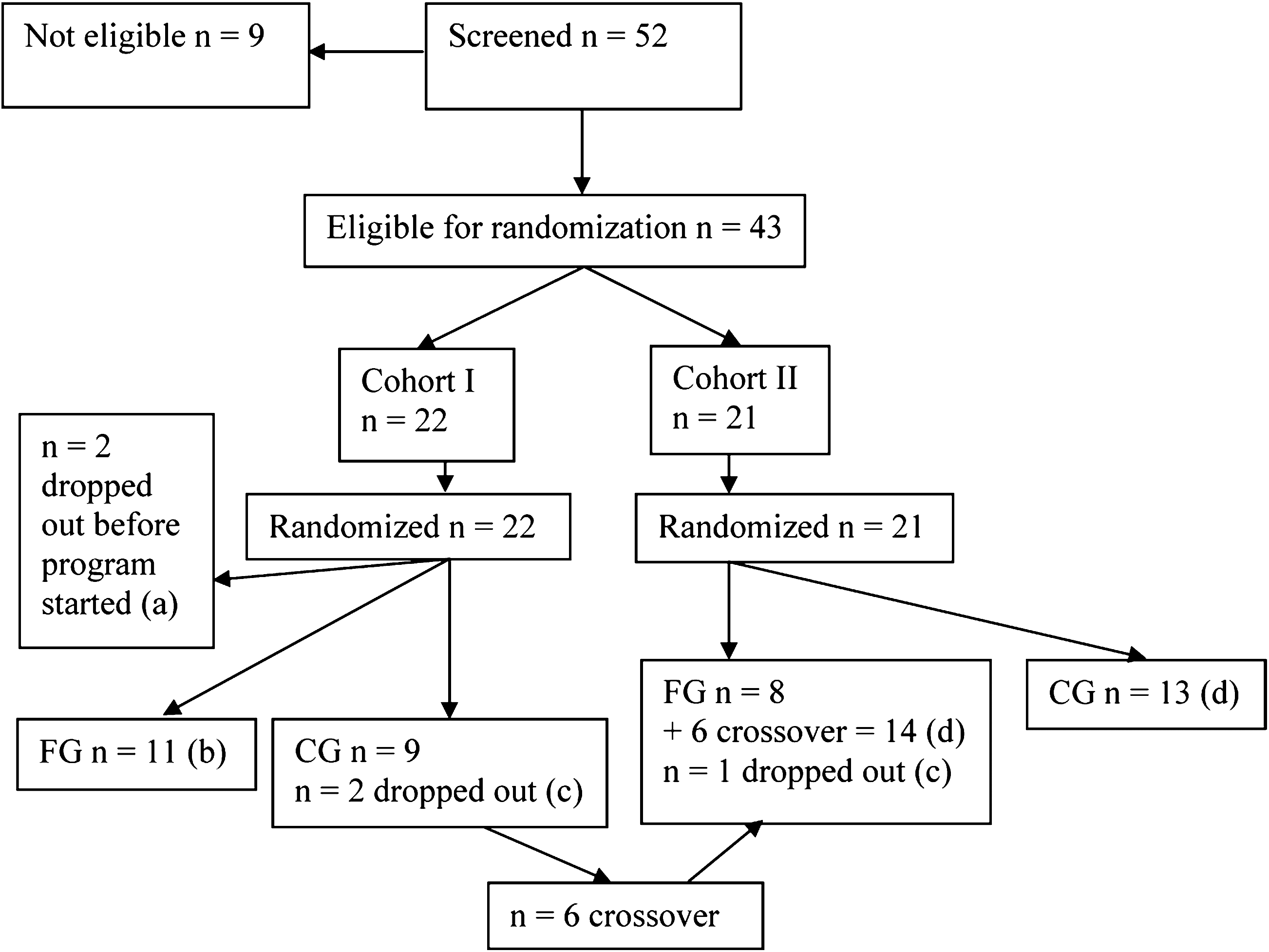
Participant flow chart. (
Procedures
Procedures of this study were approved by the Institutional Review Board of the University of South Carolina. All participants signed a written consent before screening and testing began.
Screening of participants
Participants were screened on the Mini-Mental State Examination 33 and the performance on the Timed Up and Go (TUG). 34 A short self-developed questionnaire covered general demographics and basic information about health status and physical activity behavior. The questions were derived from various sources and were based on surveys designed for older adults. 35,36 All participants provided a physician's release form prior to the pretest session.
Randomization
The screening TUG score and age were used to complete the stratified randomization of participants. In addition, persons who expressed a desire to attend the same class (couples, friends, and carpool) were allowed to do so in order to facilitate participation. Members of these units were assigned to the same treatment.
Pre- and post-testing
During the 1-hour pre- and post-test sessions, static balance was assessed using the tandem stance, mobility using the TUG and gait characteristics using the GAITRite Walkway System. 34,37 –45 Fear of falling and balance confidence participants were assessed using the Falls Efficacy Scale (FES) and the Activities-Specific Balance Confidence Scale (ABC), respectively. 46,47 The investigator conducted the gait assessment with the GAITRite Walkway System; all other tasks and scales were administered by trained staff and are described in Table 1.
Feldenkrais intervention
One (1)-hour Feldenkrais sessions were held 3 times per week for 5 weeks (total of 15 sessions) using the technique ATM. The content of the sessions included sitting, reaching, walking, turning, transfers (lying to sitting, sitting to standing, and vice versa) and relaxation. Although the lessons were based on common Feldenkrais themes (e.g., differentiation of pelvic movements, relationship between eye organization and body movement, coordination of muscles, breathing, and exploring habits), each session focused on improving balance and mobility and was adapted to meet the needs of the participating individuals. 48,49 The investigator, a certified Feldenkrais teacher, taught all Feldenkrais classes.
Statistical Analysis
Data were analyzed using the Statistical Analysis System (SAS version 9.1 for Windows, SAS Institute, Inc., Cary, NC); α was set at 0.05 for all tests. The comparability of the two groups on sociodemographic variables, general health, exercise behavior, and function measures at baseline were examined with t-tests (continuous variables) and χ 2 analyses (dichotomous variables). An intention-to-treat approach was used for data analysis. Pearson correlation coefficients were used to examine relationships between physical performance measures (balance, mobility) and self-report measures of balance confidence and falls efficacy. The variable balance (tandem stance) was censored, because a maximal score of 30 seconds could be obtained. For these censored balance data, a survival analysis was used. In this analysis, survival time indicated the time individuals were able to maintain balance. Mixed models for repeated measurements were used to compare the other dependent variables (TUG, Timed Up and Go with an added cognitive task [TUGc], FES, ABC, and gait characteristics velocity, cadence, stride length, cycle time, step length, and step time) (Table 1). The model used a compound symmetric covariance structure for repeated measurements, and also adjusted for nonindependence of measurements for those who expressed a desire to attend the same class, and for those who crossed over from cohort I to cohort II. All models controlled for age, sex, and body–mass index (BMI).
Effect sizes (ES) were calculated for mobility (TUG and TUGc), fear of falling (FES) and balance confidence (ABC) using the equation ES = (MeanPost − MeanPre)/Standard DeviationPre. For the variable balance (tandem stance), we used the median instead of the mean to calculate the ES, since the median is more appropriate as a measure of central tendency for data that have a ceiling effect.
Results
Participants
Demographic characteristics of the 47 (mean age = 75.6) older adults who participated in the study (FG n = 25, CG n = 22) are presented in Table 2.
The number of falls refers to falls during the past 3 months.
MMSE, Mini-Mental State Examination; SD, standard deviation; BMI, body–mass index.
Health status
Initially, only 2 individuals rated their general health as fair (4.3%). All others reported their health as excellent (14.9%), very good (34.0%), or good (46.8%). A variety of chronic health conditions were reported. Arthritis (n = 26), osteoporosis/osteopenia (n = 25), heart disease/attack (n = 7), and cancer (n = 5) were the most frequently reported health conditions. Eight (8) reported having joint replacements. More than half of the participants (n = 25) were on medication for high blood pressure.
Physical activity behavior
When asked about walking and physical activity behavior, nearly half of the participants reported that they either never walked or seldom walked (44.7%). Ten (10; 21.3%) individuals reported that they walked 3–4 days and 14 (29.8%) reported walking 5–7 days in the past week.
Comparability of groups at baseline
T-tests and χ 2 analyses were conducted to compare the two groups, FG and CG, at baseline on sociodemographic variables, health status, balance, mobility, gait characteristics, fear of falls, and falls confidence. Only the mean BMI of the FG was significantly higher than that of the control group (FG: BMI 27.86; CG: BMI 24.88, p = 0.047).
Correlational analysis
Correlations between physical performance measures (balance, mobility) and self-report scales (fear of falling, balance confidence) were generally low. Relationships between tandem balance and mobility and balance confidence were slightly higher than for falls efficacy (tandem balance: r = 0.36 versus r = 0.07 respectively; mobility: r = −0.28 versus r = −0.14, respectively), but none of the correlations suggest a strong relationship between measures of physical performance and self-report measures of balance confidence or falls efficacy.
Pre–post-test comparisons
Balance
Descriptive statistics for static balance (tandem stance) are presented in Table 3. The mean time on balance increased significantly (19.92 seconds to 21.83 seconds) for the intervention group, whereas the mean time on balance decreased (22.70 seconds to 22.56 seconds) for the control group. The results from the survival analysis indicated that time on balance increased for the FG group (Fig. 2).

Survival time on balance for pre- and post-test, assessed with the tandem stance and censored at 30 seconds. From pre-test to post-test, the proportion of participants who maintained the tandem stance for 30 seconds decreased from 45.5% to 38.9% for the control group (CG), but increased from 28.0% to 47.2% for the Feldenkrais group (FG).
Improvement.
Deterioration.
FG, Feldenkrais group; CG, control group; SD, standard deviation; TUG, Timed Up and Go; TUGc, Timed Up and Go with an Added Cognitive Task.
At the pre-test, 28.0% of the FG group and 45.5% of the CG group maintained the tandem stance for 30 seconds while at the post-test, 47.2% of the FG group and 38.9% of the CG group accomplished 30 seconds in the tandem stance position. From pre-test to post-test, the proportion of participants who maintained the tandem stance for 30 seconds decreased from 45.5% to 38.9% for the CG group, but increased from 28.0% to 47.2% for the FG group. The effect size of the Feldenkrais intervention was 0.57, and the effect size of the control group was −0.41. The interaction between time (post versus pre) and group (FG versus CG) was significant (p = 0.030).
Mobility
Descriptive statistics for mobility (TUG and TUGc) are presented in Table 3. Adjusted means of the mixed models for mobility are shown in Table 4 and depicted in Figures 3 and 4. There were extremely small positive changes in mean performance time for the FG group and small negative changes for the CG.
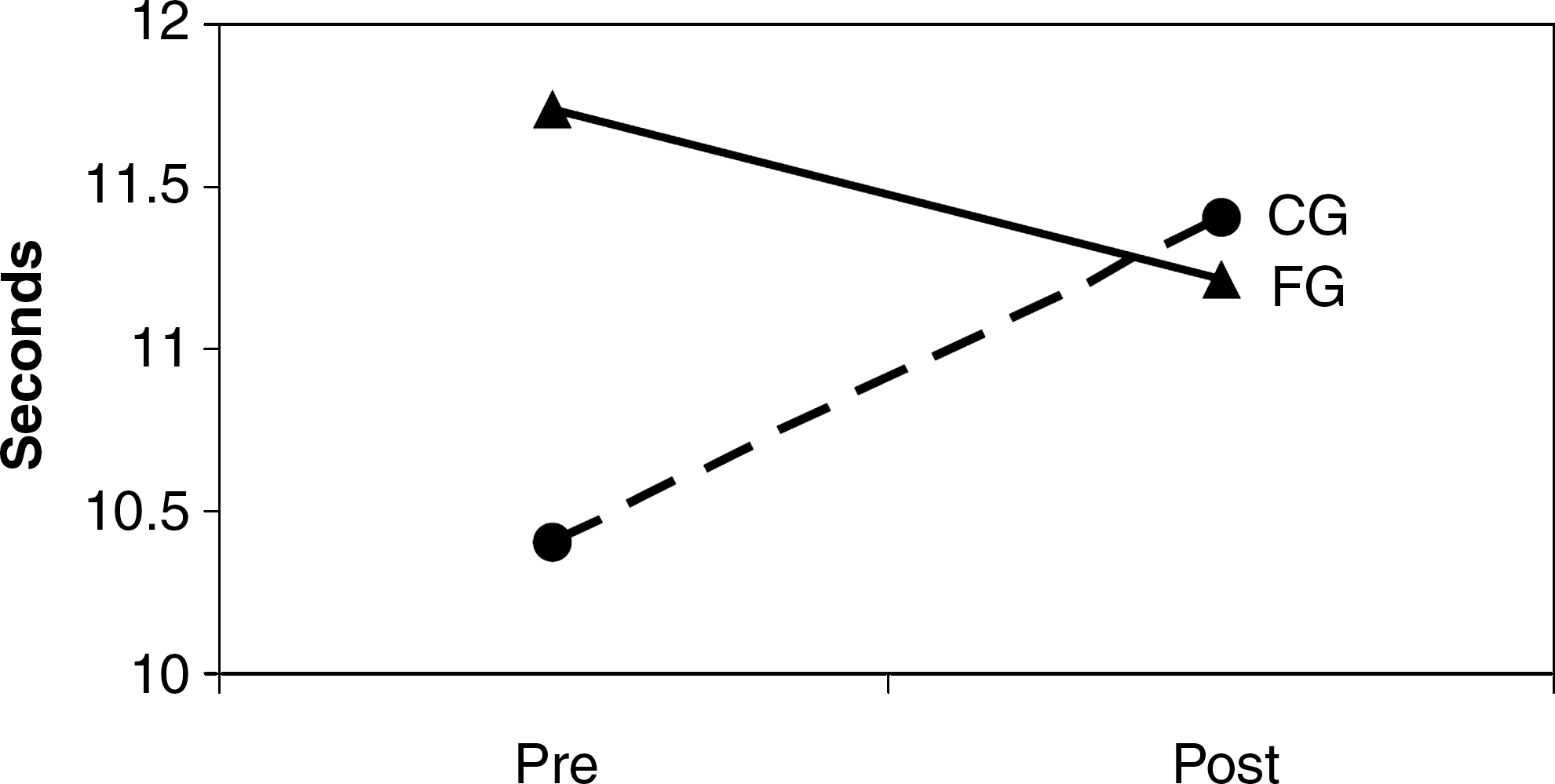
Pre-test to post-test change of the Timed Up and Go task. FG, Feldenkrais group; CG, control group.
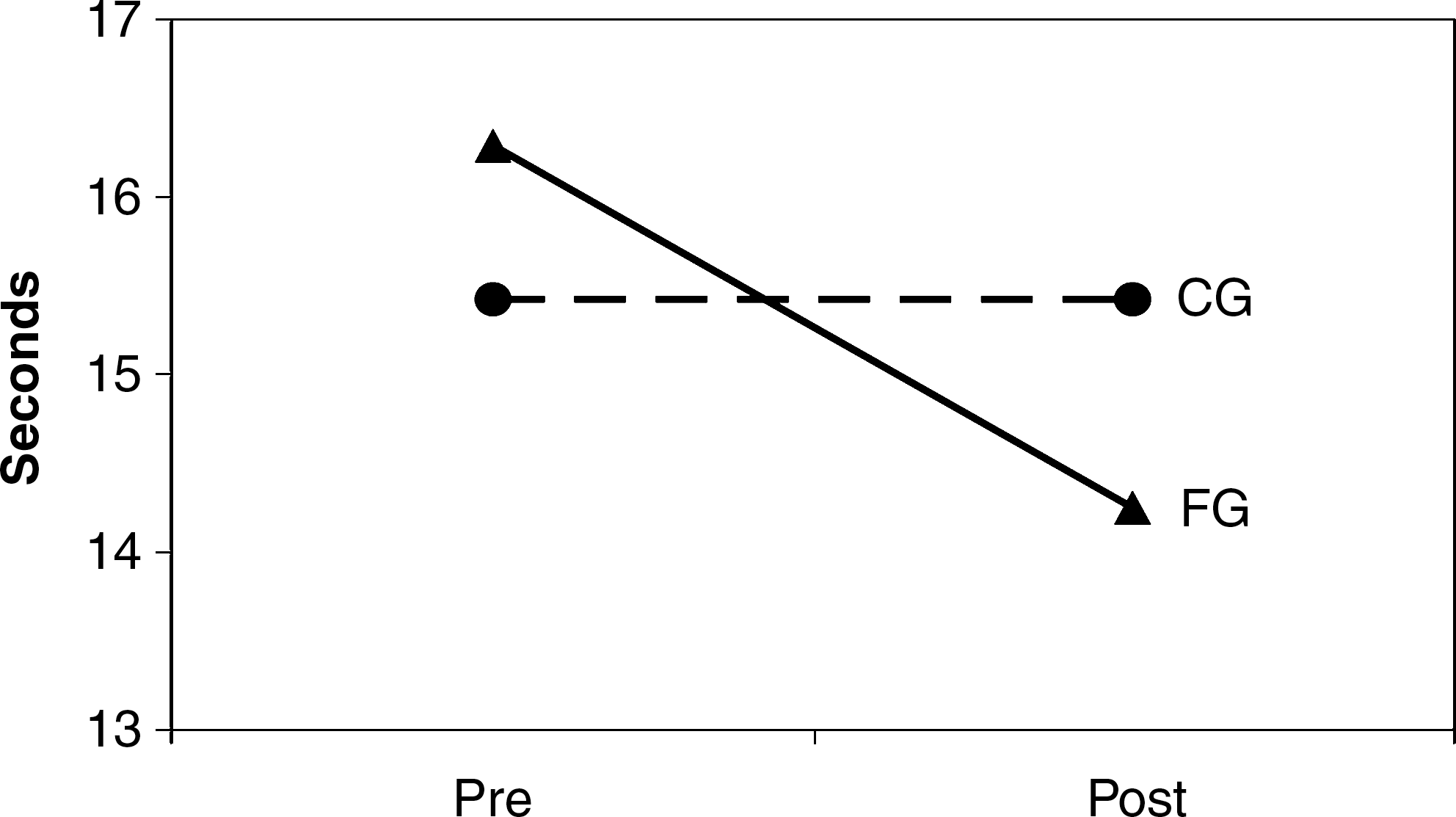
Pre-test to post-test change of the Timed Up and Go with an added cognitive task. FG, Feldenkrais group; CG, control group.
Age, sex, and body–mass index were entered into each model.
Depicts statistically significant results.
TUG, Timed Up and Go; TUGc, Timed Up and Go with an Added Cognitive Task; FES, Falls Efficacy Scale; ABC, Activities-Specific Balance Confidence Scale.
The significant Group × Time interaction for the TUG (p = 0.042) indicated that while the time to complete the TUG decreased slightly from 11.7 to 11.2 seconds in the FG group, the time to complete the TUG for the CG increased (10.4 to 11.4 seconds) (Fig. 3). Thus, the FG maintained their current level of mobility while the CG showed a decline in mobility.
Under dual task conditions (TUGc), the change in least-squares mean (adjusting for covariates) performance time was significant (p = 0.008; 16.29–14.25 seconds) for the FG group; the mean performance time of the CG did not change significantly (Fig. 4). However, the Group × Time interaction was not significant (p = 0.067). The effect size of the Feldenkrais intervention for mobility (TUG) and for mobility under dual task condition (TUGc) was 0.07 and 0.17, respectively, whereas the effect size of the control group for mobility (TUG) and for mobility under dual task condition (TUGc) was −0.39 and −0.02, respectively.
Fear of falling and balance confidence
Both groups appeared to have a measurable fear of falling at the pre-test (Table 4). For the FES, the Group × time interaction was significant (p = 0.042) (Fig. 5). After the intervention, mean scores for the FG increased significantly; no change was detected for the CG.
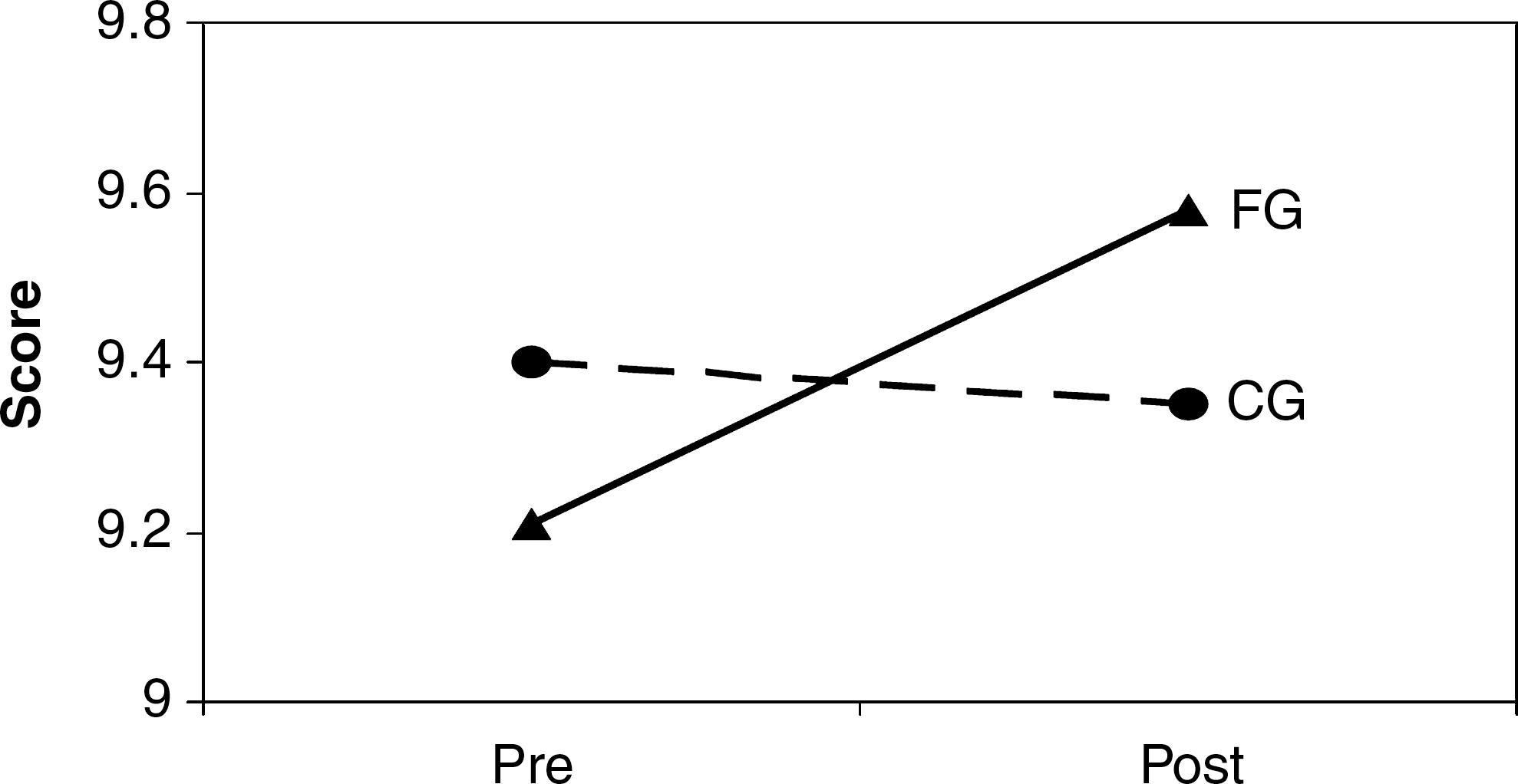
Pre-test to post-test change of the Falls Efficacy Scale (range 1 = not confident to 10 = completely confident. FG, Feldenkrais group; CG, control group.
Although the Group × Time interaction for the balance confidence scale (ABC) did not quite reach significance (p = 0.054), there was a similar pattern of change in scores for the two groups. Generally, participants in the FG group reported greater confidence in their ability to maintain balance under difficult conditions; in contrast, there was no change in the control. The effect size of the Feldenkrais intervention for fear of falling (FES) and for balance confidence (ABC) was 0.32 and 0.27, respectively. The effect size of the CG for fear of falling (FES) and for balance confidence (ABC) was −0.06 and −0.03, respectively.
Gait characteristics
In this sample, neither the FG group nor the CG group changed significantly from baseline to post-test in any gait characteristic. In the CG group, the estimated mean stride length decreased by 0.65 cm (p = 0.678), whereas in the FG group the estimated mean stride length increased by 2.07 cm (p = 0.148), but these changes were not significant. Similar changes were observed for step length in the FG group. All other changes in gait characteristics were negligible for both groups (FG and CG).
Compliance and reaction to the intervention
Compliance to the FG sessions was high. Forty-five (45; 95.7%) of the 47 participants completed the program and attended at least 12 of 15 sessions (80%). From the 24 participants in the FG group who completed an evaluation questionnaire, 92% believed or strongly believed that the Feldenkrais intervention helped to improve balance. Twenty-two (22; 92%) agreed or strongly agreed that the exercises helped to improve mobility. In addition, 23 (96%) individuals reported that their ability to get around had improved and 22 (92%) reported that they did some of the exercises at home.
Discussion
Data from the current study indicated that 15 Feldenkrais classes over 5 weeks led to significant improvements in balance and mobility but no change in gait characteristics. Additionally, there was a reduction in fear of falling and an increase in balance confidence.
The significant improvement in tandem balance observed in the intervention group is in agreement with outcomes of earlier Feldenkrais studies, two case studies and a small randomized controlled trial (N = 12), that reported positive changes in balance in persons with Parkinson's disease and multiple sclerosis. 31,32,50 Overall, a much larger proportion of the FG group achieved the maximum time of 30 seconds in the tandem stance than was true for the control group. Since a high proportion (47.2%) of participants maintained the tandem stance for 30 seconds after completion of the Feldenkrais program, future research may need to consider increasing the maximal time for the tandem balance to avoid a ceiling effect. The change in balance (ES = 0.57) had a much greater effect than the changes observed in mobility (ES = 0.07) and mobility under dual task conditions (ES = 0.17).
The significant Group × Time interaction for mobility was due more to decreases in mobility in the CG group than positive changes in the intervention group. Our data suggest that 15 Feldenkrais lessons may help to offset age-related declines in mobility that were seen in control participants. A similar pattern of change was observed in a comparable Feldenkrais study with older adults. 51 Although the Group ×time interaction of this study was not significant (p = 0.056), Vrantsidis and colleagues reported improved mobility after 16 Feldenkrais sessions while the mobility of the CG decreased. Feldenkrais exercises involve, in part, movements that focus on the center of mass in relation to the movement of the body (e.g., shifting the pelvis in different directions) and exploration of ways of getting up from a chair. These concentrated experiences may have played a role in the continued maintenance of mobility in the FG.
When participants walked and counted backwards (TUGc), there was an improvement in time in the mobility task only for the FG group. Since performance times on the TUGc were generally slower than on the TUG, this indicates that individuals tended to reduce the speed at which they walked to accommodate the added attentional demands of counting backwards. This slowing of performance is commonly observed in timed performances under dual task conditions. 52 –54 One explanation may be that after Feldenkrais exercises, the actions involved in performing the TUG were more automatic and thus the added “cognitive” challenge of counting backwards while walking did not affect mobility to the degree that it did prior to the intervention. If this change is real, it is important from the perspective that many of the activities that older adults are involved in carrying out everyday chores have a dual task nature (e.g., walking and carrying groceries, watching traffic and crossing a street, walking on uneven terrain, etc.). Thus, this outcome may have important practical application for older adults in terms of helping to maintain an optimum level of independence in performing various Activities of Daily Living.
The observed reduction in fear of falls (FES) and the increase in balance confidence (ABC) concur with findings of previous Feldenkrais studies. 32,51 Vrantsidis and colleagues assessed balance confidence with a Modified Falls Efficacy Scale and reported significant improvements (p = 0.003) after 16 Feldenkrais sessions, while Stephens and colleagues used the ABC scale and found improvements after 20 hours of Feldenkrais. Changes in fear of falling (ES = 0.32) had a slightly greater effect than changes in balance confidence (ES = 0.27). Although these changes are small, the reduction in fear of falls may have a significant impact on the physical activity behavior of individuals; previous research has shown that fear of falls contributes to inactivity among older adults. 24,55,56
The current study is the only one to examine gait in healthy older adults in a Feldenkrais intervention using the GAITRite system. In this sample, neither the FG group nor the CG group changed significantly from baseline to post-test in any gait characteristics. These findings run contrary to results of a recent study that reported significant improved gait speed in community-dwelling older adults after 16 Feldenkrais lessons. 51 Further investigation is needed to clarify the inconsistencies in potential gait changes of community-dwelling older adults after practicing Feldenkrais.
Compliance to the program was good. Factors that might have contributed to this adherence include the limited and straightforward time commitment of 5 weeks as well as the highly motivated group of older adults involved. The feedback from participants also indicated that they enjoyed the Feldenkrais program and felt that the exercises were helpful to them in improving balance and mobility. This positive attitude toward the program may have also played a role in the strong adherence to the program.
Assumptions can be made about changes in the risk of falls, since risk factors that are related to falls (e.g., poor balance) improved after completion of the Feldenkrais program. However, given the short time frame of 5 weeks between pre- and post-test and the absence of follow-up measures, we cannot be certain that the program contributed to a reduction in the number of falls among FG group participants. The lack of follow-up measures makes it impossible to know whether improvements in balance and mobility were sustained. Future studies should include long-term follow-ups to examine potential long-term benefits of the Feldenkrais intervention. We must also consider the potential limitation due to the lack of opportunity for social interaction in the CG group, as participants never met in any form of group activity. Future research should consider the addition of a social support group that is involved in some form of organized group activities.
Despite the limitations of this study, our data indicate that Feldenkrais exercises result in positive changes in balance, mobility, fear of falls, and balance confidence. Future studies should administer more than 15 lessons to examine whether a higher dose leads to greater effects on the outcome variables. Further research needs to examine whether Feldenkrais programs may impact cognitive processes and can be successfully implemented in the community. In addition, further research needs to explore whether Feldenkrais can be considered a complementary strategy for populations whose balance and mobility are challenged.
Overall, results of this randomized controlled trial increased our knowledge about the effects of the FM on select functional abilities of community-dwelling older adults. This research provided important preliminary data for future Feldenkrais research projects and directions for future research.
Footnotes
Acknowledgments
This study was supported by the Esther Thelen Research and Education Fund.
Disclosure Statement
No competing financial interests exist.