
Abstract
Background:
Acupuncture is commonly used in treating insomnia in China, and clinical studies have shown that acupuncture may have a beneficial effect on insomnia compared with Western medication.
Methods:
We included randomized controlled trials on acupuncture for insomnia. We searched PubMed, the Cochrane Library (2008 Issue 3), China Network Knowledge Infrastructure (CNKI), Chinese Scientific Journal Database (VIP), and Wan Fang Database. All searches ended in December 2008. Two authors extracted data and assessed the trials' quality independently. RevMan 5.0.17 software was used for data analysis with effect estimate presented as relative risk (RR) and mean difference (MD) with a 95% confidence interval (CI).
Results:
Forty-six (46) randomized trials involving 3811 patients were included, and the methodological quality of trials was generally fair in terms of randomization, blinding, and intention-to-treat analysis. Meta-analyses showed a beneficial effect of acupuncture compared with no treatment (MD −3.28, 95% CI −6.10 to −0.46, p = 0.02; 4 trials) and real acupressure compared with sham acupressure (MD −2.94, 95% CI −5.77 to −0.11, p = 0.04; 2 trials) on total scores of Pittsburgh Sleep Quality Index. Acupuncture was superior to medications regarding the number of patients with total sleep duration increased for >3 hours (RR 1.53, 95% CI 1.24–1.88, p < 0.0001). However, there was no difference between acupuncture and medications in average sleep duration (MD −0.06, 95% CI −0.30–0.18, p = 0.63). Acupuncture plus medications showed better effect than medications alone on total sleep duration (MD 1.09, 95% CI 0.56–1.61, p < 0.0001). Similarly, acupuncture plus herbs was significantly better than herbs alone on increase of sleep rates (RR 1.67, 95% CI 1.12–2.50, p = 0.01). There were no serious adverse effects with related to acupuncture treatment in the included trials.
Conclusions:
Acupuncture appears to be effective in treatment of insomnia. However, further large, rigorous designed trials are warranted.
Introduction
Insomnia can be treated with medications, herbal therapy, and psychologic or physical therapy. The commonly used medications include hypnotic sedative agents, such as zaleplon and benzodiazepines, but they may cause adverse effects such as damage of memory, drug resistance, dependency, and addiction. 3 Nondrug therapy including acupuncture is commonly used by patients with insomnia. The mechanism of acupuncture treatment may be regulating yin and yang to reinforce health and eliminate the pathogenic, thus improving sleep. 4 In modern medicine, acupuncture can increase the content of γ-amino butyric acid, and then enhance sleep quality. 5 We performed this systematic review to evaluate the beneficial and harmful effects of acupuncture for treatment of insomnia in randomized trials.
Methods
Inclusion criteria
Parallel randomized controlled trials (RCTs) of acupuncture compared with no treatment, placebo, or basic medical therapy in patients with insomnia were included. Combined therapy of acupuncture and other interventions compared with other interventions in RCTs was also included. Outcome measures include duration and quality of sleep, such as total sleep duration and increased sleep duration, Pittsburgh Sleep Quality Index (PSQI) scores, Index of Severity of Insomnia, Sleep Quality, and other validated scores, as well as adverse effects. Multiple publications reporting the same groups of participants were excluded. There was no limitation on language and publication type.
Identification and selection of studies
We searched China Network Knowledge Infrastructure (1979–2008), Chinese Scientific Journal Database VIP (1989–2008), Wan Fang Database (1985–2008), PubMed (1966–2008), and the Cochrane Library (Issue 3, 2008). All of the searches ended at December 2008. The search terms included “acupuncture,” “acupressure,” “acupoint,” “electroacupuncture,” or “meridian” combined with “insomnia,” “sleepless,” or “dysomnia.” Two authors (H.J. Cao and H. Li) selected studies for eligibility and checked against the inclusion criteria independently.
Data extraction and quality assessment
Two authors (H.J. Cao and H. Li) extracted the data from the included trials independently. Quality of the included trials was evaluated according to the following categories 6 : Category A (good): studies have the least biases and their results are considered valid. These studies are likely to consist of (1) clear description of the population, setting, interventions, and comparison groups; (2) appropriate measurement of outcomes; (3) appropriate statistical and analytical methods; (4) no reporting errors; (5) less than 20% dropouts; (6) clear reporting of dropouts; and (7) appropriate consideration and adjustment for potential confounders. Category B (fair): studies are susceptible to some degrees of biases that are not sufficient to invalidate the results. These studies may have suboptimal adjustments for potential confounders and may also lack certain information that is needed to assess limitations and potential problems. Category C (poor): studies have significant biases that may invalidate the results. These studies either do not consider potential confounders or do not make adjustments for them appropriately. These studies may have critical flaw in design, analysis, and/or reporting, missing information, and/or discrepancies in reporting.
Data analysis
Data were summarized using relative risk (RR) with 95% confidence intervals (CI) for binary outcomes or mean difference (MD) with 95% CI for continuous outcomes. Revman5.0.17 software was used for data analyses. Meta-analysis was used if the trials had a good homogeneity on study design, participants, interventions, control, and outcome measures. Publication bias was explored by funnel plot analysis.
Results
Description of studies
After primary searches from seven databases, 1956 citations were identified, and the majority were excluded due to obvious ineligibility, and full text papers of 67 studies were retrieved. Forty-six (46) RCTs were included in this review (Fig. 1), 7 –47 and among them, five trials were unpublished and were from graduate student dissertations. * There were 21 studies including 16 RCTs excluded from this review due to multiple publications, non-RCT design, data unavailable, or not meeting one of the inclusion criteria. 48 –68 The characteristics of included trials are listed in Table 1, and the reasons for excluded studies are listed in Table 2.
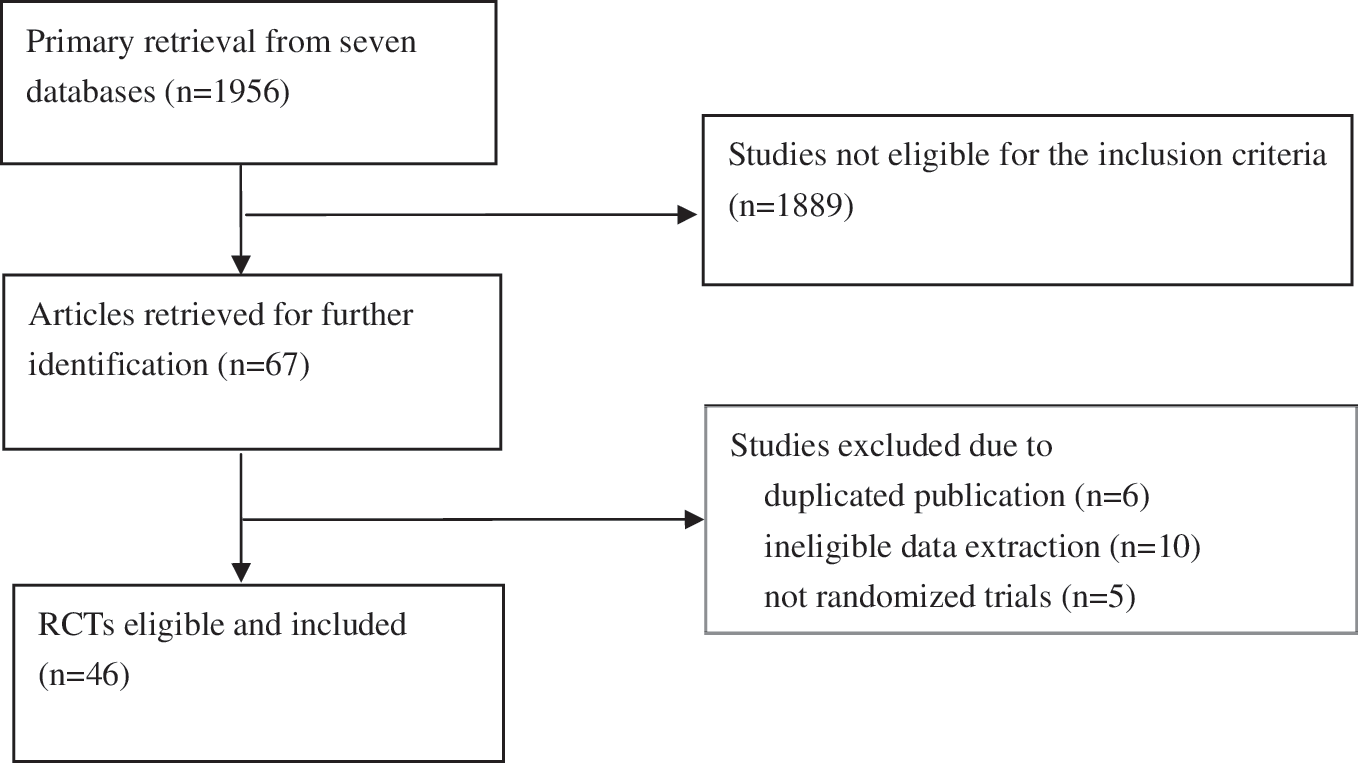
The process of study selection. RCTs, randomized controlled trials.
CCMD, Chinese Classification of Mental Disease; CCMD-2, second version of CCMD; CCMD-3, third version of CCMD; ICD-10, 10th version of International Classification of Disease.
The selection of the acupoints according to syndrome differentiation.
The 46 trials involved a total of 3811 patients with insomnia, of whom 2882 were patients with primary insomnia, 220 were insomnia patients with poststroke, 179 with depression, 60 in remittent stage with schizophrenia, 166 with cervical spondylosis, 100 with drug addiction, and 204 with end-stage renal disease. There was a wide variation in the age of subjects (13–85 years) and disease duration (10 days–40 years). Thirty-three (33) trials specified six diagnostic criteria, including four national criteria in China, one criterion from the United States, and one international classification of disease (ICD). The interventions included acupuncture (body, auricular acupuncture, electroacupuncture, acupressure, and acupoint injection), acupuncture plus conventional medication, or herbal medicine. The controls included no treatment, sham acupuncture, medication, or herbal medicine. The acupoints used were not fixed, the number of acupoints selected ranged from 2 to 20, and the total treatment duration ranged from 2 days to 10 weeks. The top 10 commonly used body acupoints and top 5 auricular acupoints are presented in Figures 2 and 3 Ten (10) of the 46 trials used the scores (PSQI) as the outcome measure and 12 kinds of scores were used for sleep measurement. Thirty-three (33) trials used four classes to evaluate treatment effects including cure, markedly effective, effective, and ineffective according to the degree of overall symptom improvement.
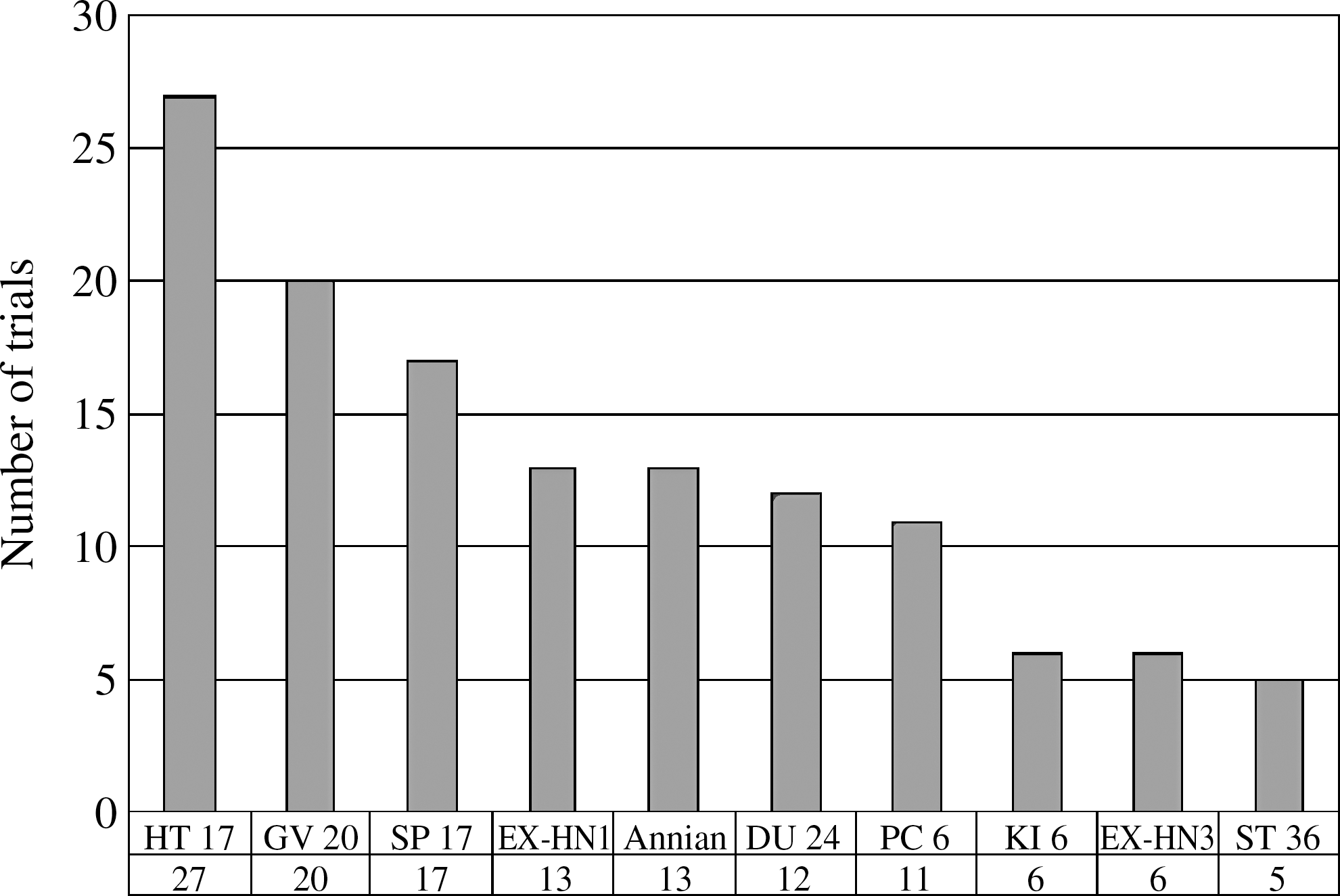
Top 10 points used for meridian acupuncture treatment.
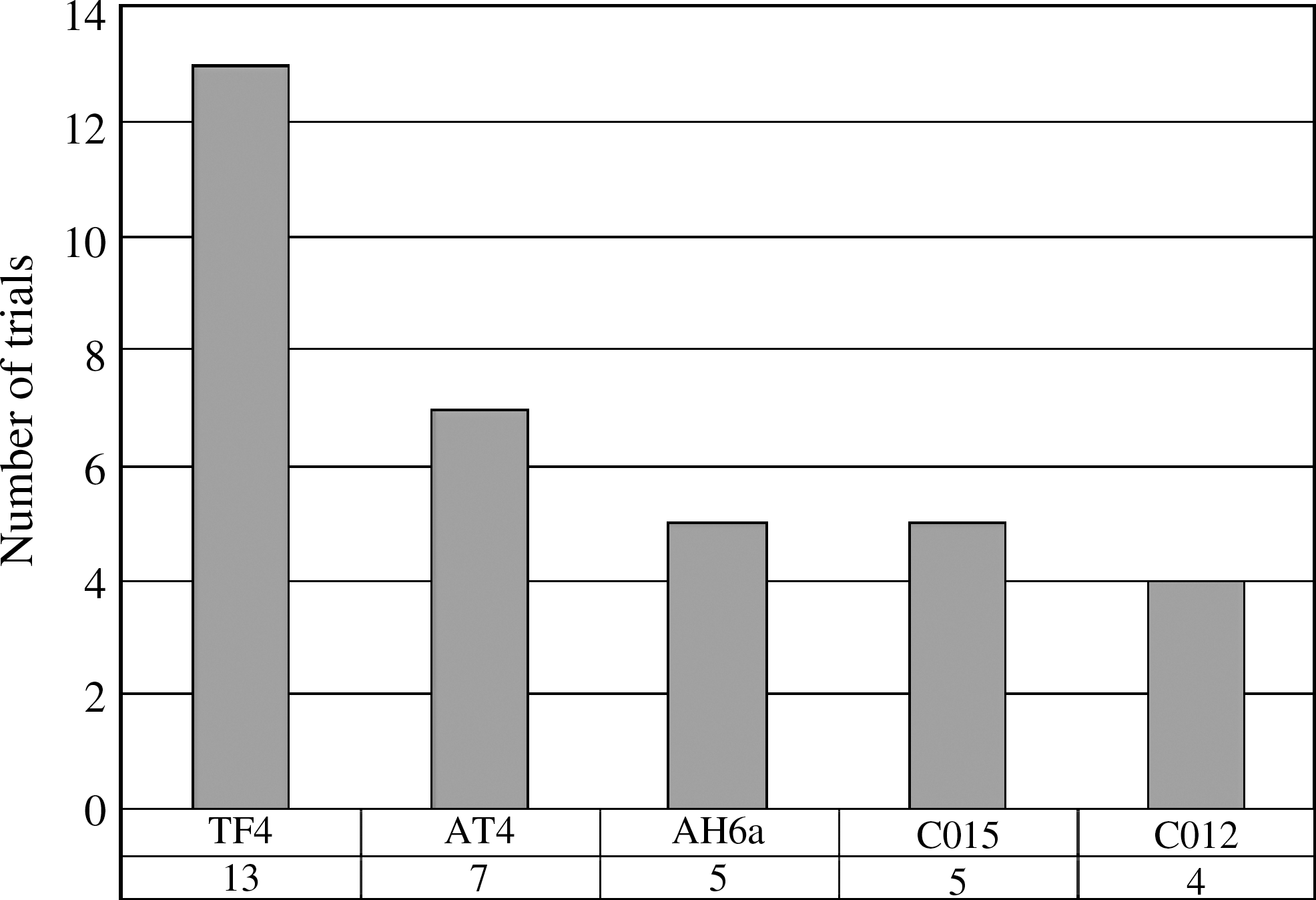
Top five points for auricular acupuncture treatment.
Methodological quality
The majority of the included trials were assessed to be of generally fair methodological quality. According to our predefined quality assessment criteria, seven trials (15.22%) were evaluated as good (A), and the remaining as fair (B). The sample size varied from 22 to 182 participants, with an average of 35 patients in each group. Only 1 of the 46 trials 40 reported sample size calculation that used Sample Power software, essential for ensuring adequate statistical power of 82%. Fourteen (14) trials described the randomization procedure, using random number table, drawing, or coin tossing. Three trials 37,41 (Luo L 2005, unpublished data) used envelope as the method for allocation concealment. Eight trials 7,27,35,39,42 (Huang X 2000; Kou J 2003; Zhang Q 2006, unpublished data) employed a blinding procedure: four of them used patient blinding, three used assessor blinding, and one trial provide no information on blinding. There was high potential to have bias caused by belief of the subjects and the measurers in the remaining 38 trials. Nine (9) of the 46 trials reported the number of dropouts 7,15,17,27,35,36,41 (Kou J 2003; Luo L 2005, unpublished data), six trials 7,8,16,35,36,40 (Huang X 2000, unpublished data) mentioned follow-up, and none of them used intention to treat method. The reporting quality of 46 trials according to Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) varied among different trials (Table 3).
Effect estimates (Table 4)
Acupuncture versus no treatment
Five (5) trials 7,33,35,36,46 compared acupuncture with no treatment. Data from the no-treatment group was divided in half when compared with the other two interventional groups to avoid duplicated use in a three-arm trial 40 in the meta-analysis. The result showed that acupressure was significantly better than no treatment on improving the total scores of PSQI (MD −3.28, 95% CI −6.10 to −0.46, p = 0.02).
TEAS, transcutaneous electrical acupoint stimulation; CI, confidence interval; PSQI, Pittsburgh Sleep Quality Index; MD, mean difference; RR, relative risk; SDS, Self-rating Depression Scale; SQ, sleep quality; ARS, Asberg Rating Scale; LSEQ, Leeds Sleep Evaluation Questionnaire; SRSS, Self-Rating Sleep Scale; HAMA, Hamilton Anxiety Scale.
Real acupuncture versus sham acupuncture
Three trials 7,19,35 compared real versus sham acupuncture or acupressure, respectively. The result of meta-analysis showed that real acupuncture was more effective than sham acupuncture on improving total scores of PSQI (MD −2.94, 95% CI −5.77 to −0.11, p = 0.04).
Acupuncture versus Western medication
Twenty-six (26) trials compared acupuncture with Western medications. Most meta-analyses showed positive effect of acupuncture in treatment of insomnia, but one meta-analysis 16,41 reported no difference between acupuncture and drugs on improving sleep duration evaluated by patients (MD −0.06, 95% CI −0.30 to 0.18, p = 0.63), one pooled results 15 (Luo W 2006, unpublished data) showed no difference between acupuncture and trazodone on improving total scores of the Self-rating depression scale (SDS; MD −0.02, 95% CI −0.34 to 0.30, p = 0.90), and also another one trial 30 reported no significant difference (MD −1.55, 95% CI −4.25 to 1.15, p = 0.26) between electroacupuncture and clonazepam on improving the scores of Hamilton Anxiety Scale.
Acupuncture plus other interventions versus other interventions
Seven trials compared acupuncture plus Western medications versus medications. Meta-analysis of two trials 8,20 showed significant difference between acupuncture plus medications compared with the same medications on increasing the total sleep duration by hour (MD 1.09, 95% CI 0.56–1.61, p < 0.0001). Other results of meta-analysis were consistent that acupuncture plus medications had a much more therapeutic effect than medications alone.
Four trials 13,27,28,34 compared acupuncture plus herbal medicine with herbal medicine. Only one trial 28 showed there was no significant difference between the combination therapy and herbal group on increasing the numbers of patients whose total sleeping time increased for more than 3 hours (RR 1.30, 95% CI 0.93–1.82, p = 0.13). However, the meta-analyses showed a positive effect of acupuncture plus herbal medicine compared with herbal medicine on increasing the numbers of patients with sleep rates that increased by more than 60% (RR 1.67, 95% CI 1.12–2.50, p = 0.01).
Meta-analysis of 10 trials showed a better effect of acupuncture than medications for the outcome of the number of patients whose total sleep duration increased for more than 3 hours (RR 1.53; 95% CI 1.24–1.88; p < 0.0001; 10 trials).
A funnel plot analysis of the 10 trials was generated, and it showed a significant asymmetry (Fig. 4).
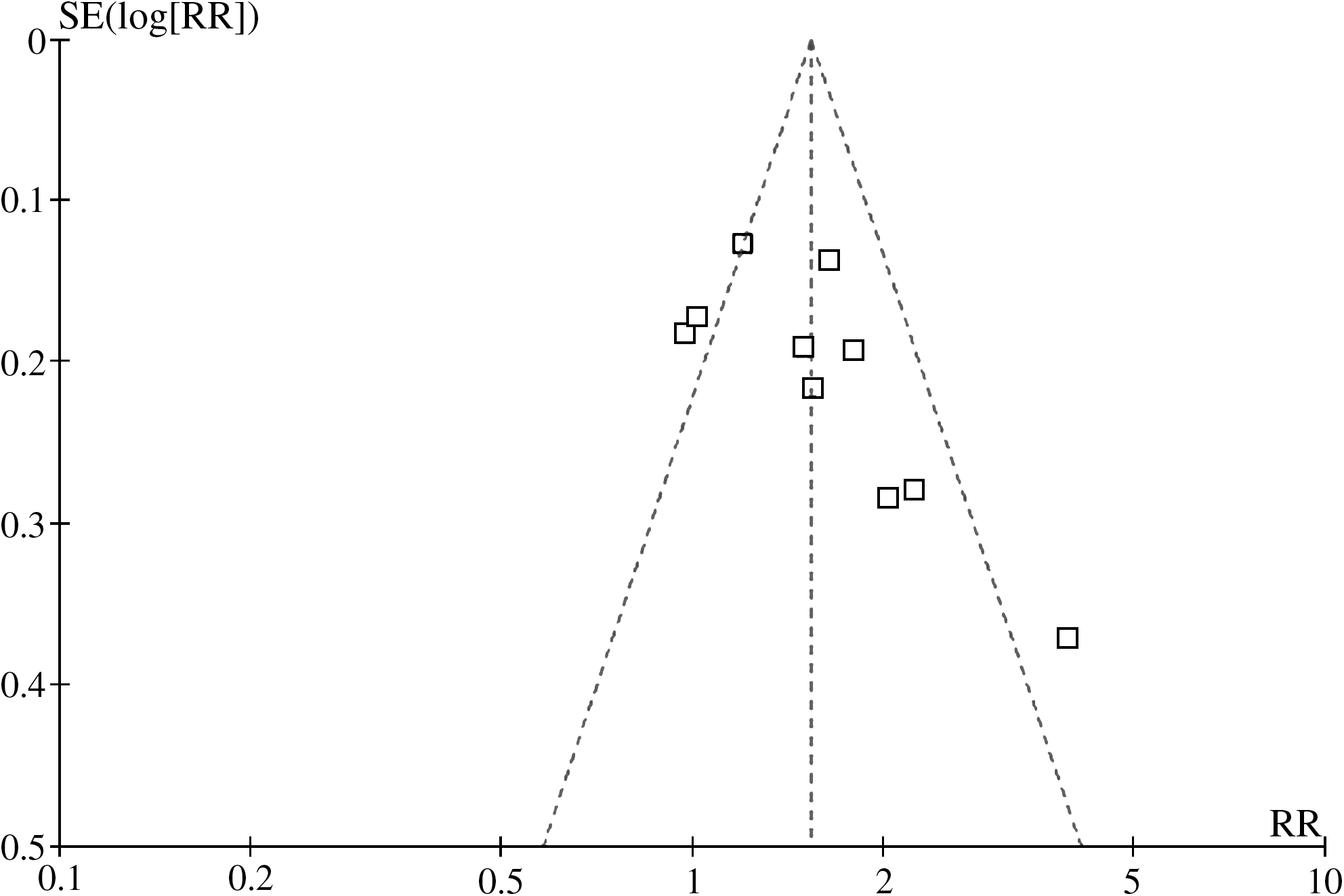
Funnel plot of 10 randomized controlled trials for the outcome of number of patients with sleeping time increased over 3 hours. SE, standard error; RR, relative risk.
Adverse effect
Outcome of adverse effect with relation to acupuncture was described in 12 trials; only 3 of them reported minor adverse effect in the acupuncture group. Two (2) trials 16 (Kou J, 2003, unpublished data) reported no adverse effect observed in the acupuncture group. Another trial 15 reported mild headache (1 case), and lassitude (1 case) in the acupuncture group (n = 28), whereas there was dizziness (3 cases), constipation (3 cases), dry mouth (2 cases), palpitation (1 case), and oscitation (1 case) in the trazodone group (n = 27).
Two (2) trials 15,28 evaluated the scores of the adverse effect rating scale. The result showed that acupuncture was safer than trazodone (MD −3.12, 95% CI −4.92 to −1.32, p = 0.0007).
Discussion
Based on the results of meta-analyses, the majority showed that compared with no treatment, sham acupuncture, or medications, acupuncture was significantly better on improving parameters in sleep quality and duration, and the combination of acupuncture and other interventions appears more effective than those interventions alone, though it was possible that the beneficial effect from acupuncture is overvalued because of the small sample size, flawed methodology of the included trials and the short follow-up duration.
There are several limitations in this review. First, the quality of the included studies is generally fair, which means the existence of moderate risk of bias. Because of inadequate reporting of randomization and blinding in the majority of trials, it was possible that there was performance bias and detection bias due to patients and researchers being aware of the therapeutic interventions for the subjective outcome measures. Intention-to-treat analysis was not applied in data analyses in the trials. The funnel plot asymmetry suggests the possibility of publication bias and small, low-quality trials. In addition, there is probably language bias because 43 of 46 included trials were published in Chinese, and 3 were published in English, but conducted in Taiwan and Korea. Vickers 69 found that some Asian countries including China publish unusually high proportions of positive results, for which publication bias is a possible explanation. Second, 22 trials used Chinese diagnostic criteria of insomnia, 1 trial used U.S. criterion, and 6 trials used an ICD, but there were no specified diagnostic criteria for insomnia in the remaining trials. The participants are quite heterogeneous in terms of type of insomnia, such as in elderly with an average age of 81 years, or in heroin addicts with dyssomnia after detoxification. Third, there were different acupunctures used in the trials, which included acupuncture as a unique treatment in 18 trials, and acupuncture combined with other treatments in 28 trials. Twenty (20) trials selected the acupoints according to syndrome differentiation based on Chinese medicine theory, and 26 trials used fixed acupoints throughout the treatment. According to STRICTA, all of the 46 trials reported the style of acupuncture, rationale for treatment, points used, number of treatment sessions, frequency of treatment, and other interventions, but only about 50% of trials reported needling techniques such as the depth of insertion, responses elicited, needle stimulation and needle type, and less than 30% of trials mentioned the details of control intervention and practitioner's background. Controls were also heterogeneous in these trials, including Western medications, no treatment, sham acupuncture, acupressure, or herbal medicine. The treatment duration varied from 2 days to 10 weeks. Fourth, the use of composite outcome measures in 34 trials to evaluate overall improvement of symptoms limits the generalization of the findings. The classification of cure—markedly effective, effective, or ineffective—is not internationally recognized, and it is hard to interpret the effect. We suggest future trials to comply with international standards in the evaluation of treatment effect. Although there is no major statistical heterogeneity among the data analyses, we realized that the clinical heterogeneity would be very significant due to the variations in study quality, participants, intervention, control, and outcome measures. The interpretation of the positive findings from the meta-analyses needs to be incorporated with the clinical characteristics of the included trials and evidence strength. Therefore, the conclusion of the beneficial effect of acupuncture for insomnia needs to be confirmed in large and rigorously designed RCTs.
Our latest searches identified three systematic reviews of acupuncture for insomnia. One (1) Cochrane review published in 2007 included only 7 randomized trials published in English, and it concluded that current evidence was not sufficient to support the use of any form of acupuncture for the treatment of insomnia. 70 Another systematic review published in Chinese in 2005 included only 6 Chinese trials with low quality, and had a similar conclusion. 71 The most recent review published in 2009 72 included 12 clinical trials (including 3 randomized trials) and 18 case series. However, the authors were not able to access Chinese databases and quite a lot of studies published in Chinese were missed. This review by Huang and colleagues described the TCM diagnosis for insomnia and acupuncture treatment, which is considered relevant to clinical practice. We conducted comprehensive searches in both English and Chinese databases, and included 46 randomized trials. Our review suggests that acupuncture improves sleep quality and increases sleep duration. However, the beneficial findings of this systematic review still are not conclusive due to the limitations of the methodological quality of the included trials. Further rigorous trials are warranted.
Most of the existing trials are small and there is a moderate risk of bias. Further high-quality studies with larger sample size are needed to confirm the effectiveness of acupuncture in treating insomnia. Randomization methods need to be clearly described and fully reported. Although blinding of the acupuncturists might be very difficult, blinding of patients and outcome assessors should be attempted as far as possible to minimize performance and assessment biases. Analysis of outcomes based on intention-to-treat principle is important. Since insomnia is a highly heterogeneous disease with different etiology and severity, acupuncture is likely to have different effects on different subgroups of patients. Therefore, future clinical trials should be focused on particular subgroups or include a very large sample size to delineate the effect of acupuncture on different types of patients or different treatment techniques. In addition, well-defined diagnostic or classified criteria such as ICD-10 or the third version of Chinese Classification of Mental Disease should be employed to make a precise clinical diagnosis of insomnia, and hence increase the comparability between trials. Reporting of trials should follow the Consolidated Standards of Reporting Trials 73 to explicitly explain the process of the treatment, so that the clinicians or other researchers can possibly use this process. Because the acupuncturist's technical competence may influence the therapeutic effect, we suggest that researchers describe the detailed treatment and that trials be conducted by qualified, well-trained acupuncturist in future studies according to STRICTA. 74 Since insomnia may wax and wane with or without treatment, a longer follow-up period with serial measurement of outcomes is important to determine the effectiveness and long-term effect of acupuncture.
Footnotes
Acknowledgments
H.J. Cao and J.P. Liu were supported by a grant from the National Basic Research Program of China (“973” Program, no. 2006CB504602) and the 111 Project (B08006). J.P. Liu was supported in part by grant number R24 AT001293 from the National Center for Complementary and Alternative Medicine (NCCAM) of the U.S. National Institutes of Health. We also thank medical student Zhanguo Xie for his help in identifying articles for this review.
Disclosure Statement
No competing financial interests exist.
*
Huang XQ, Dong GR. Clinical study of acupuncture with combining Yin-Yang or Qi-Blood points on treatment of insomnia [in Chinese]. Dissertation for the master degree from Heilongjiang University of Traditional Chinese Medicine. 2000;
Kou JY, Sun YZ. Clinical observation of effect of acupuncture with Tiaozang Anshen method on Treatment of Insomnia [in Chinese]. Dissertation for the master degree from Heilongjiang University of Traditional Chinese Medicine. 2003;
Luo L, Yu SG. Effect of rolling acupuncture on treatment of insomnia [in Chinese]. Dissertation for the master degree from Chengdu University of Traditional Chinese Medicine. 2005;
Luo WZ, Lai XS. Clinical study of therapeutic effect of acupuncture with Jieyutiaoshen method on treatment of insomnia with depressive disorder [in Chinese]. Dissertation for the master degree from Guangzhou University of Traditional Chinese Medicine. 2006;
Zhang Q, Dong GR. Study of therapeutic effect of acupuncture with combining Yin-Yang or Qi-Blood points method on treatment of insomnia and its effect on polysomnography [in Chinese]. Dissertation for the master degree from Heilongjiang University of Traditional Chinese Medicine. 2006;