
Abstract
Background and purpose:
Integrated rehabilitation (IR) in patients with stroke with respect to death rate and feasibility, initiated as a reduced death rate, was observed in patients with angina pectoris receiving IR.
Design:
A case–control study included 73 consecutive patients with ischemic stroke. Death rates were compared with those of the general Danish population matched for age, gender, and observation period, as well as data from the community-based Copenhagen Stroke Study.
Interventions:
IR was conducted in an outpatient clinic, by professionals as well as by the patient: the former as a specific acupuncture treatment, the latter as a comprehensive biofeedback guided stress management program including diets, physical- and relaxation exercise, Chinese health philosophy, cognitive and mindfulness-related exercises, and specific biofeedback guided acupressure.
Results:
The 4½-year accumulated risk of death was 11.6% (95 confidence limits: 3.2%–20.0%) for the 73 patients with stroke treated with IR, compared to 18.4% for the general Danish population matched for sex, age, and time period. The corresponding figures for patients receiving conventional stroke treatment were 43.2% (95 confidence limits: 39.7%– 46.7%), and 20.0% for the general Danish population matched for sex, age, and time period.
Conclusions:
IR was found to be feasible for patients with stroke as a complementary treatment to conventional stroke treatment, and added no risk of dying when compared to Danish stroke patients receiving conventional medical treatment. The results invite further testing in a randomized trial.
Introduction
In previous studies, we found that integrated rehabilitation (IR) seemed to help patients with ischemic heart disease with respect to risk of death, quality of life, and health care expenses. 14 –17 IR demands a substantial effort by the patient, implying ambulatory treatment and education with an ongoing daily effort. The primary aim of the present study was to examine whether IR could be conducted in patients with stroke without major side-effects. The secondary aim was to elucidate the effect of IR on cardiovascular disease in a broader sense. This may be achieved by pooling data from two consecutive trials using the same design and intervention. The trials included patients with two different cardiovascular diseases, angina pectoris, and stroke, which are characterized by having similar risk factors.
Materials and Methods
Design and outcome measures
The report is based on data from a clinical database, which included 91 patients with stroke who started the IR treatment in the period between January 1, 1991 and May 31, 2002 on an intention-to-treat basis. Seventy-three (73) patients met the diagnostic criteria for ischemic stroke used in Copenhagen Stroke Study. 18,19 For each of the 73 patients, the diagnosis was confirmed in the registries of the National Board of Health. 20
Via a unique 10-digit identification code, all persons living in Denmark can be tracked with regard to mortality data. Death rates of the general Danish population were computed as death rates based on data from approximately 35,000 Danes with the same age, gender, and observation period as our patients (general Danish population I in Fig. 1), 21 and for the patients from the Copenhagen Stroke Study (general Danish population II in Fig. 1). 21

Accumulated risk of death for 4 groups: 4.5-year risk for integrated rehabilitation and a matched control group from the general Danish population; 4-year risk for patients from Copenhagen Stroke Study who survived initial stroke and a matched control group from the general Danish population.
With respect to the comparison to the death rate of the patients from the Copenhagen Stroke Study, each of the 73 patients receiving IR was plotted into the accumulated survival curve of the Copenhagen Stroke Study, with respect to the time of start for IR and length of observation period as to the recommendation of the leader of the Copenhagen Stroke Study. 19
Since the present study represents the second consecutive clinical database study examining the effect of IR in patients with cardiovascular disease, the results of the first study
15
are added to the present study using conventional statistics. The likelihood of obtaining a statistically significant result in two consecutive trials is the product of the likelihoods:
For both studies, similar risk evaluation measures have been used: The general Danish population, and Danish patients with the same disease receiving conventional treatment. When compared to the general Danish population, a twofold increased death risk rate has been found for both diseases. 18,22
The patients
Patient data are summarized in Table 1. The median time period between diagnosis and start of IR was 12 months (interquartile range 3–24 months).
The Intervention: Integrated Rehabilitation
IR is a biofeedback-guided stress management and lifestyle adjustment program based on self-care.
The patients had an average of 15 IR consultations (interquartile range 7–17) during the full observation period with the aim to have the first 10 consultations within the first month.
At each visit, the patient was given acupuncture as well as education in self-care (IR) on an “intention-to-treat” basis. Thus, each patient is presented with the options and selects, in collaboration with the physician according to personal preferences, possibilities and needs from the overall list of possible means. The professional program was guided by measurement of pressure pain sensitivity of the chest bone. This measure was used as a marker for stress and autonomic tone of the heart, a theory that later has been confirmed.
23
It was used as a guideline for long-term effects of the entire program as well as for the effect of the individual acupuncture treatment. Acupuncture was performed with the patient in the supine position and done in agreement with traditional Chinese practice.
24
After placing needles, they were left in situ for 20 minutes with no further mechanical or electrical stimulation. Five (5) principal points were used: Shanzhong (C.V.17), Jueyinshu, and xinshu (U.B.14 and 15), Neiguan (Per.6), and Zuzanli (St.36). The self-care education aimed to provide the individual patient with the motivation and the tools to exert daily control of his or her own health. The education was based on addition of new lifestyle-related behavioral patterns with positive effects, rather than restrictions of existing patterns with a negative effect.
25,26
The program included the following means: biofeedback measurement of stress sensory nerve stimulation (acupressure/shiatsu massage) a variety of daily cognitive and mindfulness-related stress reduction techniques a variety of daily physical exercises diets social activity and/or getting a pet, and education in disease mechanisms from a Western medical and a traditional Oriental medical point of view.
The patient is instructed to perform acupressure twice daily for prevention. Acupressure is performed by applying finger pressure for 1 minute, sufficiently enough to feel it, but without causing pain on the following acupuncture points (Fig. 2): on the sternum at the level of the fourth intercostal space (Shanzhong, C.V. 17), and on the back 1.5 inch lateral to the spinal process of the fourth and fifth thoracic vertebra (Jueyinshu and Xinshu, U.B. 14 and 15). The acupressure is said to be conducted successfully when a decrease of tenderness can be observed by the patient after performing the treatment. If this result is not obtained, the patient is instructed to repeat the treatment. The experience of the acupressure effect teaches the patient that individual control is possible, and the daily success obtained by doing acupressure helps motivate the patient for self-care. Furthermore, if possible, the spouse or partner is instructed to conduct the acupressure on the back, which may add independently to the stress-relieving effect. 27,28
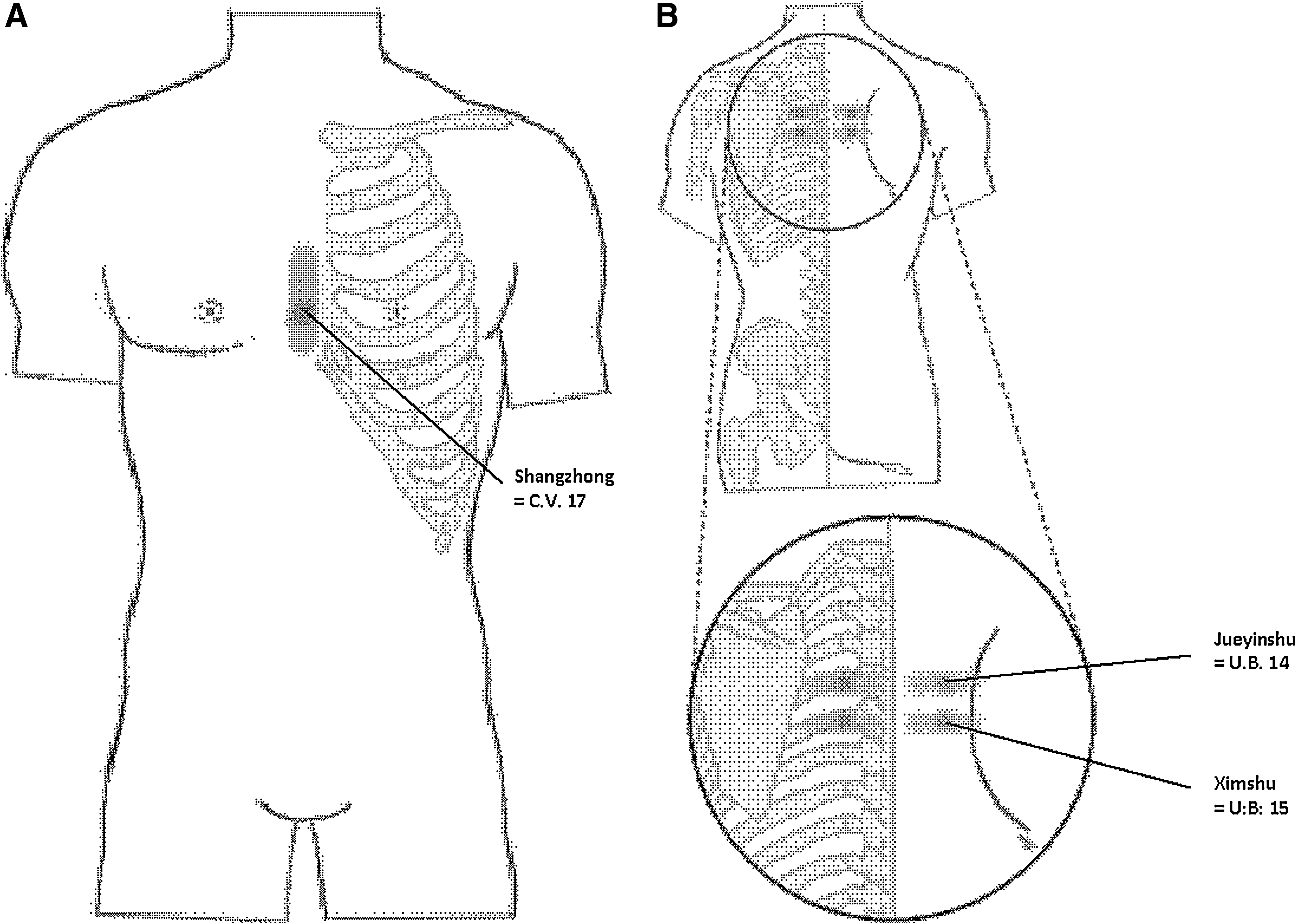
Acupressure points for patient self-care.
The daily cognitive and mindfulness-related stress-reduction techniques had the aim to increase bodily and mental awareness as well as to improve cognitive data processing. It included meditation, relaxation and awareness exercises, expressive writing, count blessings and life attitude exercises, music listening, and leadership- and time-management tools. 29 –41
The daily physical exercises included a 20-minute brisk walk without a break, the Royal Canadian Air Force physical fitness program, 42 yoga 43,44 and/or qigong breathing exercises. 45 The diet recommendations focused on a Mediterranean diet, 46 –49 in combination with green tea, 50 nuts, soy, and moderate alcohol. 51 Social activity and/or having a pet was recommended as a separate activity. 52 –55
The full program is described in a 330-page booklet 56 (including a total of 593 scientific references), which each patient received at the start of treatment.
The accumulated risk of death was calculated by Kaplan-Meier's analysis (SPSS for Windows).
Results
The median observation period was 54 months (interquartile range 27–74 months), starting from the beginning of treatment and until the occurrence of death or the end of observation period at January 24, 2003.
Risk evaluation for death in stroke patients
The 4½-year accumulated risk of death was 11.6% (95% confidence limits [CL]: 3.2%–20.0%) for the 73 patients with stroke treated with IR in addition to conventional stroke treatment, compared to 18.4% for the general Danish population matched sex, age, and time period (p < 0.1). The corresponding figures for patients receiving conventional stroke treatment only were 43.2% (CL: 39.7%–46.7%), and 20.0% for the general Danish population matched for sex, age, and time period (Fig. 1).
Risk evaluation for death in patients with cardiovascular disease
In the 103 patients with angina pectoris who were candidates for invasive treatment, the 3-year accumulated risk of death was 2.0% (CL: 0.0%–4.7%) compared to 6.4% for the general Danish population 15 (p < 0.05). When combined with the findings of the present study (p < 0.1), the likelihood (p) for IR being associated with a decreased risk of dying when compared to the general Danish population is 0.05 (p 1) × 0.1 (p 2) = total p < 0.005, which equals the likelihood for a 50% reduction from IR in death rate, when compared to conventional treatment for ischemic cardiovascular lifestyle-associated disease.
Discussion
Our results indicate that IR may be beneficial for patients with stroke and cardiovascular disease or at least not harmful.
Many factors, such as lifestyle, exercise, psychologic treatment, and hence also IR are said to be related to the risk and course of illness based on knowledge obtained by observational epidemiological studies because experimental studies are impossible for practical reasons or just not feasible. Thus, observational studies are frequently used in the evaluation of stroke recommendations and risk factor analysis. 9 –14,19 In addition, clinical databases are to be used for quality control comparisons between hospitals. Furthermore, an editorial in JAMA 57 points out that observational studies suffice to support practical recommendations when the effect size is large and the risk is low, as, for example, with advice to stop smoking. The same may be true for IR.
The present results are drawn from a patient database and public databases. Any quality control review has limitations such as expectation bias (because neither the patient nor the therapist can be blinded), selection bias (as patients are not randomly allocated to a treatment or a control group), lack of a control group, and because evaluation of the effect applies to the whole treatment and not to the individual components. For IR and acupuncture, the patients and the therapist cannot be blinded. Patient and doctor expectations are known to influence the outcome in a variety of trials. 24 However, in the present investigation patients rarely saw their doctor after the initial 3 weeks of education and still avoided death. Accordingly, the abovementioned sources of bias are not likely to explain the findings of this study.
Selection bias occurs when the clinician excludes too many patients from a trial. 58 Moreover, it occurs when some patients do not want to participate in the trial. Thus, in any study, population selection bias occurs. Nevertheless, conclusions from such studies have been applied to the patient population as a whole. In any quality-control review, selection is unavoidable, since the patients have chosen the treatment or the hospital themselves.
We tried to compensate for bias by: using the toughest possible yardstick for comparison: the general population; using death rate as the effect variable, as death rate is not substantially affected by methodological limitations
27
; by conducting two consecutive studies using the same design and control conditions, including patients with different disease, yet both potentially influenced by stress and the selected intervention; comparing with control groups consisting of thousands of patients in order to reduce the confidence limits with respect to patient characteristics.
With the aim to address all these sources of comparison bias between the two groups of patients, differences in patient characteristics should be considered. The patients of the present study are younger, more often male, more often with a partner, less frequently smoking and diabetic, most likely having a less severe stroke, but more often with hypertension. However, in the Copenhagen Stroke Study, all patients dying at home were excluded. 19 With respect to the difference in age between the two groups, this is taken into account by the construction of two control groups from the general Danish population.
With respect to the effect from IR compared to other kinds of interventions provided for patients with the same diseases, the death rate for stroke patients who survive the first year after their stroke is reported to be double the death rate of the general population, 9,10 and a similar rate is found for patients with ischemic heart disease. 17 Furthermore, the cumulative 3-year death rate was 2% for our candidates for invasive treatment, compared to a 30-day death rate of 3.2% and 2.6% for Danish patients receiving percutaneous coronary intervention and coronary artery bypass graft, respectively. 58
In conclusion, in two consecutive studies, IR was found to be associated with a minimum of 50% in reduction of death rate, when compared to similar patients with cardiovascular disease receiving conventional treatments (p < 0.005).
Other studies using comprehensive lifestyle adjustments in patients with cardiovascular disease have found improvements in risk factors, quality of life, and degrees of atherosclerosis, but no effect on death rate. 59,60
A possible explanation for this difference could be the effects of the biofeedback-guided treatment leading to a high compliance rate for the self-care lifestyle adjustments, as well as the activation of cardiovascular autoregulation and reduction of the autonomic tone by acupuncture and acupressure. 15,61,62
Accordingly, we find it fair to conclude that IR may be a potentially useful treatment for patients with both a previous stroke and angina pectoris. The results presented here invite further research, ideally in randomized trials.
Footnotes
Acknowledgments
This work has been financially supported by the Knowledge and Research Center for Alternative Medicine, Denmark (Videns- og Forskningscenter for Alternativ Behandling [ViFab]). We thank Tom Skyhøj Olsen for assistance in preparation of the study and subsequent critical review of the results, Finn Gyntelberg for critical review of the manuscript, and Arne Hahr Andreasen and Pernille Bjørn Petersen for statistical analyses.
Disclosure Statement
No competing financial interests exist.