
Abstract
In Part I of this pair of articles, the fundamental experimental observations and theoretical perspectives were provided for one to understand the key differences between our normal, uncoupled state of physical reality and the human consciousness–induced coupled state of physical reality. Here in Part II, the thermodynamics of complementary and alternative medicine, which deals with the partially coupled state of physical reality, is explored via the use of five different foci of relevance to today's science and medicine: (1) homeopathy; (2) the placebo effect; (3) long-range, room temperature, macroscopic size-scale, information entanglement; (4) an explanation for dark matter/energy plus human levitation possibility; and (5) electrodermal diagnostic devices. The purpose of this pair of articles is to clearly differentiate the use and limitations of uncoupled state physics in both nature and today's orthodox medicine from coupled state physics in tomorrow's complementary and alternative medicine.
Introduction
We have also discovered a procedure, via the use of conscious intention imbedded into an intention-host device, for generating a coupling medium between these two uniquely different kinds of substances so as to significantly change the properties of the combined material. 1 We label such composite material the partially coupled state of physical reality. In addition we have discovered that, in the human body, the acupuncture meridian/chakra system is already at the coupled state of physical reality 1 while the rest of the body is at the uncoupled state. Thus, human intention is capable of altering the output performance, to some degree, of their own acupuncture meridian/chakra system and this, in turn, is capable of significantly altering the energetic performance of the electric atom/molecule cells in our composite body. This is the working territory of psychoenergetic science and complementary and alternative medicine (CAM).
In this article, five examples of the application of the working principles of Part I 1 are laid out in some detail for the reader. Both CAM and orthodox medical practitioners need to become operationally aware of both the similarities and significantly different science foundations involved in their own medical considerations.
Examples
Where does homeopathy fit into the picture?
A recent article, published in this journal, 2 recorded a roundtable debate between proponents of homeopathy and its opponents from allopathy, with no clear resolution of the issue. I believe that this “butting of heads” occurred because there is no overarching general theoretical construct that includes both perspectives. This had not been formulated until recently. 3,4 In this section, my purpose is to clearly reveal this general theoretical construct through the use of thermodynamics.
Utilizing my duplex space model as discussed in the Part I, 1 the Gibbs thermodynamic free energy per unit volume * G of a material in the partially coupled state of physical reality can (according to Part I, Equation 1 in the Introduction with the undefined quantity Q replaced by G) be generally expressed as an expansion about some standard state value G0 in terms of the thermodynamic intensive variables to obtain the mathematical result given in Appendix I. G – G0 is the sum of two main groupings of contributions from different thermodynamic intensive variables, and ξ is defined as the general representation of all these different thermodynamic intensive variables that include: P = pressure, T = temperature, C = concentration of a particular species, E = electric field, H = magnetic field and g = gravitational field.
Expressed in this way, one can immediately distinguish in D-space the electric, magnetic dipole, atomic, molecular, and allopathic contributions from the R-space magnetic information wave and homeopathic contributions. Thus, in terms of thermodynamics, the homeopathic contributions are real and distinguishable from the allopathic contributions provided that (1) αeff is nonzero in magnitude and (2) ξj is much smaller than
For all humans, their acupuncture meridian/chakra system is already at the partially coupled state of physical reality,
4
so the local αeff is always greater than 0. Thus, if the mathematical variations of the slope
Homeopathic physicians need to understand that their remedies are not functioning at the traditional electric, magnetic dipole, atomic, molecular level of the body but, rather, at the magnetic information wave level within the physical vacuum that interpenetrates all the atoms and molecules of the human body.
In addition, it is important to understand that the overall picture is somewhat more complex than might be anticipated from the equations of Appendix I. This is because of the strength of a particular individual's value of αeff due to the acupuncture meridian/chakra-related biofield. This leads to a type of human-generated “placebo” effect that is always present to some small degree.
Moving on to homeopathic potencies, the succussion/dilution-with-intention aspect of homeopathy has “boggled” the mind of traditional chemists and allopathic medicine practitioners for well over a century. From their traditional thought processes concerning ideal thermodynamic solutions, they naturally ask the question, “How can there possibly be a chemical reactivity effect when the average aqueous solution concentration, Ci of the treatment molecule, i, has been reduced to less that one molecule per 100 mL of solution by the sequential succussion/dilution process?”
In response, one needs to realize that all processes in nature that we know of are driven by spatial or temporal differences in thermodynamic free energy functions, G-G0 (see Appendix I). To simplify things a little, let us restrict our remarks to just the ∂G/∂Ci = μ i = the chemical potential contribution to G for the ith-species. In terms of all the thermodynamic intensive variables mentioned above, μi is completely specified by Equation I-5b of Appendix I.
Now, a very important definition for the chemical activity is given by
so that
Here, γi is called the thermodynamic activity coefficient for the ith-species and γI* is the modified thermodynamic activity coefficient (see Appendix I, Equation I-5d).
For ideal chemical solutions, experience has shown that, as Ci is taken toward very high dilutions, γi goes to unity so, both terms on the right-hand side of Equation I-3b become very small in magnitude and ai becomes insignificant. This would completely support the position of traditional chemists and allopathic medical practitioners if a sequentially diluted and succussed with intention solution were an ideal thermodynamic solution, but it is not, it has been diluted with intention! In order to show this effect, we return to Equations I–5c and 5d of Appendix I.
In Equation 1 above, the Ci– term deals with the very local perturbation effect of the solute molecule on the immediate host water molecules, while the γi- effect relates to the sum of all the macroscopic environmental effects stored in the water solvent associated with all the processing details that act on the therapy molecule i.
For example, the effects of AC or DC electric and magnetic fields on Equation I–5d result in general energy storage as does the ΔP term due to the pressure pulse associated with succussion. This pressure pulse creates cavitation and nanobubbles of air in the host water that, in turn, create highly entangled, inhomogeneous, localized, electric and magnetic fields that provide both macrostructure patterns and excess energy in the bulk water. Furthermore, an αeff Qmi- term should be included in Equation I–5b to account for the coupled state of physical reality 1 providing specific information from the coupled vacuum level of physical reality. Thus, even while the ln Ci- term in Equation 1b above is shrinking to 0, the ln γi*- term is increasing toward very large values. This is definitely not the behavior of a thermodynamically ideal solution! This result is totally consistent with the experimentally observed behavior of solutions reported by Elia and Niccoli 5 and by Roy et al. 6
Where does the placebo effect come from?
The experimental findings referred to in the previous Part I 1 of this series indicate that there can be, and is, a profound connectivity between one part of Nature and another and that any one of us can potentially influence all biological life forms around us by our biofield emissions and the information they carry, whether we consciously intend it or not. In this regard, it is useful for us to have a mental picture as to how we operate in life with respect to one another and how all the time energy/information emissions can occur from our surroundings to us, as well as from us to our surroundings.
Figure 1 provides a simple picture of the five key factors involved in this general interactive relationship. 1 Usually, all five components of this figure are intimately involved in the interaction even though the practitioner and client using some material device may only acknowledge that she/he and the client are intimately involved in the process. Now, let us look at what has been labeled the placebo effect.

The simplest possible general communication system between practitioner and client in complementary and alternative medicine. EM, electromagnetic.
My interest in this phenomenon of Nature began on reading a short 1999 article by Enserink, 7 who noted how greatly the placebo effect's magnitude in double-blind pharmacological studies had grown in the previous 15 years. He pointed out that “when companies started testing drugs for obsessive–compulsive disorder (OCD) back in the mid-1980's, the placebo response rate in this old testing was almost zero.” Thus, the normal experimental assumption that the placebo in the experimental protocol was an inert participant was a good approximation to the truth at that time.
However, as time passed, the placebo response rates began to creep upward to a point in 1999 where they were 70%–80% of the treatment response rates and one could reasonably conclude that some clinical trials failed because of high placebo response rates. How is this possible if the placebo behaves in the overall experiment as an inert object? Let us look into that because, according to Part I, Equation 1 , if something is happening in Nature to cause αeff to slowly increase with time, but in an accelerating fashion, then the connectivity between things would likewise increase in an accelerating fashion and the second term on the right of Part I, 1 Equation 1 could be of negligible size in the mid-1980s and of a significant portion of Qe in 2000.
In Appendix II, the magnetic information wave aspect of the system represented in Figure 1 has been worked out, and one can readily see that a macroscopic information entanglement between all of the designated subsystems of the overall system can occur and furthermore, that this piece of physics is the origin of the placebo effect. The relevant aspects of physics are the following. In R-space, each subsystem must be represented as a vector with both amplitude, R(k), and phase angle, θ(k), where each is a function of the position coordinate, k, in R-space. The entire system's vector, Rs(k)exp[iθs(k)], is given by the vector sum (head to tail addition) of all the subsystem vectors converted first to common units, where exp = the exponential function and i = the imaginary number (−1)1/2 (or i2 = −1). Experimentally, one measures the system intensity Is, which is given by Rs
2 and which involves Rsexp(iθs) multiplied by its complex conjugate, Rsexp(-iθs), which eliminates the “imaginary” part to give a mathematically “real” quantity. Is is given by two groups of terms: (1) the sum of the squares of each vector amplitude and (2) the sum of pairs of different vector amplitudes multiplied by the cosine of the phase angle differences between these pairs, and The total information entanglement for the Figure 1 system is given by Equation 4d of Part I
1
or by the pairwise term of Appendix II, Equation 5b.
Now, let us consider a typical clinical trial involving the subsystems (1) doctors, D, (2) treatment, T, (3) placebo, P, and (4) subjects, s. For such a system event written in Equation 1 of Part I format using the suffices of these subsystems, the placebo-effect magnitude will be given by
Thus, although QeP≈0 because the placebo is essentially inert at the electric, magnetic dipole, atomic, molecular level; QMP is definitely not 0, provided that the system is functioning at the partially coupled state of physical reality where αeff is greater than 0. Since the overall event involves humans and their biofields, the system–event is definitely at the coupled state of physical reality.
Small details relating to the D-space separations between the doctors and the subjects can be readily handled in the mathematics, since the vehicle of interaction occurs via R-space not D-space. This will become more clear with the next example.
Where does long-range, room temperature, information entanglement between macroscopic-sized spaces, objects, or humans come from?
The first important point to recognize in this example is that electric, magnetic dipole, atomic, molecular substance directly interacts with, and communicates with, its own kind via a space–time subspace. Conversely, its conjugate, magnetic information wave substance directly interacts with, and communicates with, its own kind via a reciprocal subspace that has frequency domain coordinates. These two very different kinds of substances cannot directly interact with each other because both have mass and, while the positive mass portion is constrained by relativity theory to move at velocities less than c, the negative mass portion is constrained in space time by Qm plus relativity theory to move at velocities greater than c (see Part I, Equation 2a 1 ). In the uncoupled state of physical reality, each of these two, unique domains of substance exhibits a U(1) electromagnetic gauge symmetry state (Ue(1) and Um(1)). For one of these domains of substance to interact and communicate with the other, even indirectly, requires the presence of a coupler medium, which I have heretofore named deltron, which can be activated from the domain of emotion (see Part I Figure 2 1 ) and lies beyond relativity theory constraints.

A schematic illustration of D-space and R-space as a construct.
In gauge reaction form, this coupling process is thought to occur in two major steps, (1) a reaction between deltrons and vacuum information waves, w, to create “rope-like” information waves with magnetic charge type properties plus stoichiometries of wjδk ratios followed by (2) reactions between Ue(1) materials and
Here Cδ is the starting deltron concentration and SU(2) is the electromagnetic gauge symmetry condition of the coupled state of physical reality.
Let us now use Figure 2 as a convenient metaphor for describing how both coupling between these two domains occurs and what is required for information entanglement to occur between the D-space locations A and B. We begin in the totally uncoupled state of physical reality (the left side of Equation 3a with Cδ = 0) with almost identical pH-measuring and recording equipment at D-space sites A and B located thousands of miles apart. There was also tacit agreement between the human operators at sites A and B to cooperate in a joint experiment. The dynamic process of change begins by placing a ΔpH = +1 unit IIED at only site A, plugging it into an electrical power source and switching it on. The electrically active IIED (intention imprinted electrical device) is, in turn, thought to act as a source of deltrons by intention-activation of the emotion domain of that space. This increases Cδ in Equations 3 and begins to drive the reaction to the right. This eventually generates small D-space patches of SU(2) material via a typical nucleation and growth process. What this means is that the deltrons from A allow the equilibrium magnetic information wave spectral distribution to develop in R-space at A. Since R-space is a frequency domain, this means that this pattern is available to every location in space–time and, in particular, available to the B-site in D-space. However, at B, the D-space equilibrium counterpart to the new R-space magnetic information wave spectral distribution is not present. Although the D-space pH-equipment is present, it is not conforming to the R-space pattern generated by A and so leakage of deltrons from R-space to D-space at B occurs to provide this local equilibrium. That, in turn, requires transfer adjustments of deltrons, etc., from D-space to R-space at A and from R-space to D-space at B until B is displaying similar pH-behavior as A (i.e., ΔpH = +1 units).
An adjunct procedure for understanding this process is to recognize all key subsystems involved in this overall system event, as in the previous section for the placebo effect and how the placebo term is paired with all other subsystem terms. Since D-space site B has been tacitly acknowledged as a part of the overall experiment, it needs to be listed as a subsystem of the overall event and, since all the pH-measuring equipment is also present at B, only ΔpH(t) type of information and an IIED are absent at B to exactly replicate what is at A. The ΔpH(t)-information can be readily transferred via R-space (not via D-space) as indicated above but cannot materialize an IIED at B. Thus, the ΔpH(t) patterns at A and B are unlikely to be exactly replicated. This suggests that, in future work, placing a UED (an unimprinted intention-host device) at B might produce more exact nonlocal information entanglement between A and B sites regarding ΔpH(t) results.
Can this model explain the presence of dark matter, dark energy, electric matter acceleration at the outer envelope of the universe plus human levitation?
Let us look at these four phenomena in order:
Dark Matter: recalling Part I, Figure 2, 1 normal gravitational forces occur when the positive mass of electric substance interacts with its own kind. However, astronomers have detected gravitational effects occurring at observable objects of electric mass by something that is not observable with normal instruments. This is exactly what one would expect from the presence of space curvature due to negative mass substance interacting with negative mass substance when αeff in Equation 2 is small.
Dark Energy: Communication between electric substances of positive mass occurs via energetic electromagnetic photons that constitute EM “light” energy. Likewise, communication between magnetic information wave substances of negative mass occurs via energetic magnetoelectric photons, 1 which constitute “dark” energy. Both dark energy and dark matter produce curvature changes in space even though the sources of these effects are not independently detectable via today's instrumentation.
Accelerating Universe Expansion: When only positive mass substance exists in an expanding universe, one expects that a deceleration of the rate of this expansion should be observed at the outer edge of the universe. However, a few years ago, astronomers observed just the opposite situation to be occurring. Once again, considering Part I Figure 2, 1 this is what one might expect if positive mass substance is actually interacting with negative mass substance (when αeff in Equation 2 is of significant magnitude).
Levitation: Utilizing the foregoing concepts in humans, one can foresee the possible occurrence of human levitation appearing as a phenomenon when humans develop the inner self-management ability to greatly increase Qm and αeff with respect to mass quality. Levitation will occur when the negative mass interaction between the human's Qm-body and the earth becomes greater than the positive mass interaction between the human's Qe-body and the earth. A similar approach is ultimately expected to be developed in devices and vehicles when the appropriate technology is invented.
How do electrodermal diagnostic devices work so well for some practitioners?
Human skin consists largely of two main layers, an outer and thinner layer, the epidermis, plus an inner, thicker layer, the dermis. The epidermis consists of stratified, squamous, epithelial tissue which, on the inside, connects to the dermis of fibrous connective tissue via a basal membrane and to the air surface via a thin layer of flattened dead cells called the stratum corneum that have converted to the water-repellent protein keratin that continually flakes off. New cells are produced adjacent to the basal membrane at the rate old keratinized cells are lost from the stratum corneum.
Any cellular membrane contains fixed charge sites that may be predominantly positively or negatively charged, depending upon the pH of the tissue fluid relative to the isoelectric point (IEP) of the cells (the IEP is the solution pH needed to electrically neutralize the charge state of the surface). For the case of the solution pH being more acidic than the IEP, H+ will absorb on the membrane surface and it will become electropositively charged. In this case, it will be selectively permeable to anions only. For the opposite case, where the pH is more alkaline than the IEP, the membrane becomes electronegatively charged and is permeable to cations but not anions. The IEP of a membrane depends upon the degree and type of proteins and carbohydrates embedded in the cell surface. Skin is generally electronegatively charged and is thus permeable to cations. A plot of surface potential, ϕS, often called the ZETA potential, as a function of fluid pH relative to the surface IEP is given in Fig. 3.
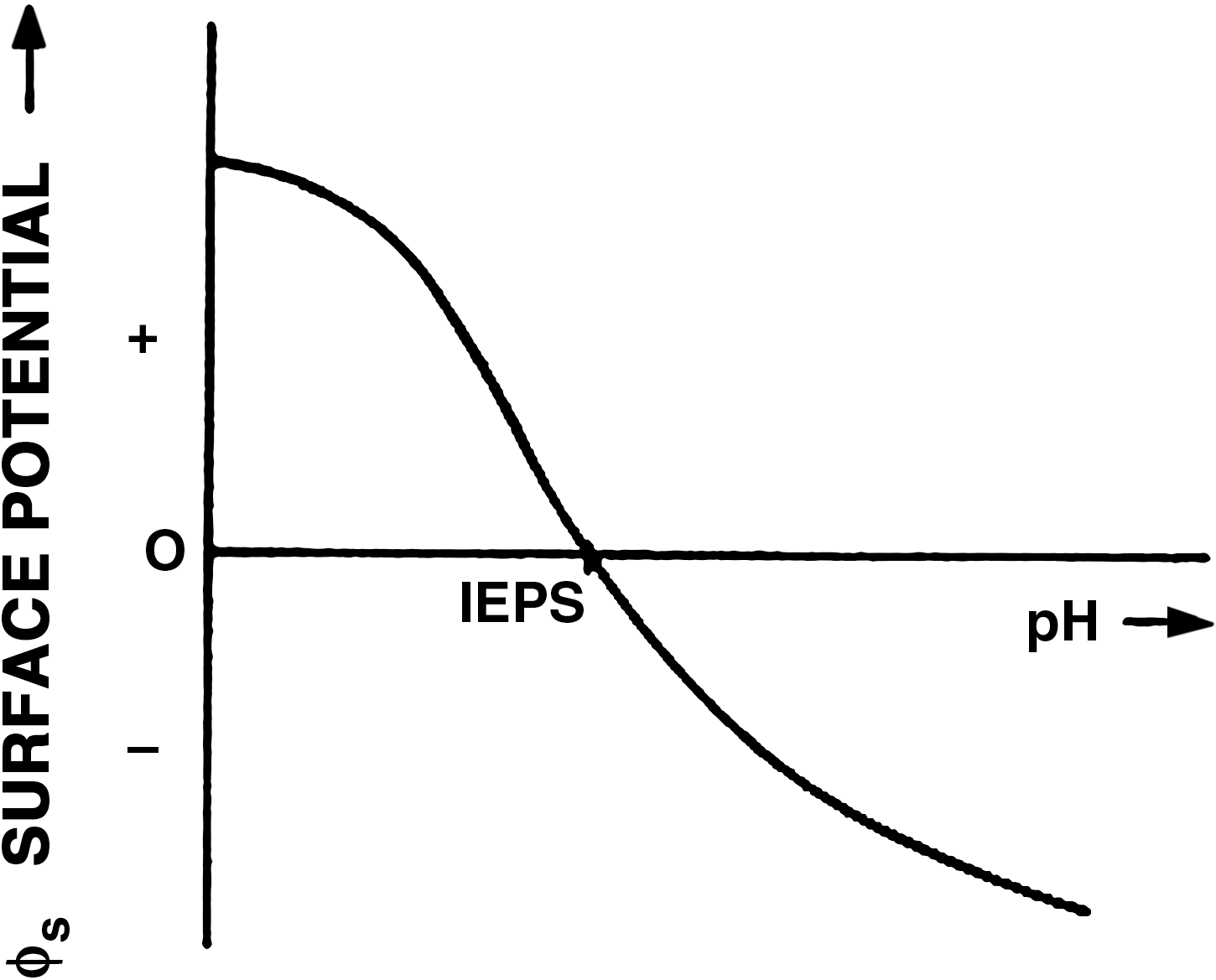
Schematic plot of surface electrical potential (zeta potential) as a function of fluid pH relative to the surface isoelectric point (IEPS).
When a steady electric current is moved outward through the skin (cathodal current), the DC resistance of the stratum corneum falls, as illustrated in Figure 4. The opposite occurs when electric current moves inward through the skin (anodal current). In both cases, the time-constant, τ1, is ∼10–50 seconds and the resistance changes by a factor of ∼5. The reason for this behavior for a cation permeable membrane is illustrated in Figure 5.
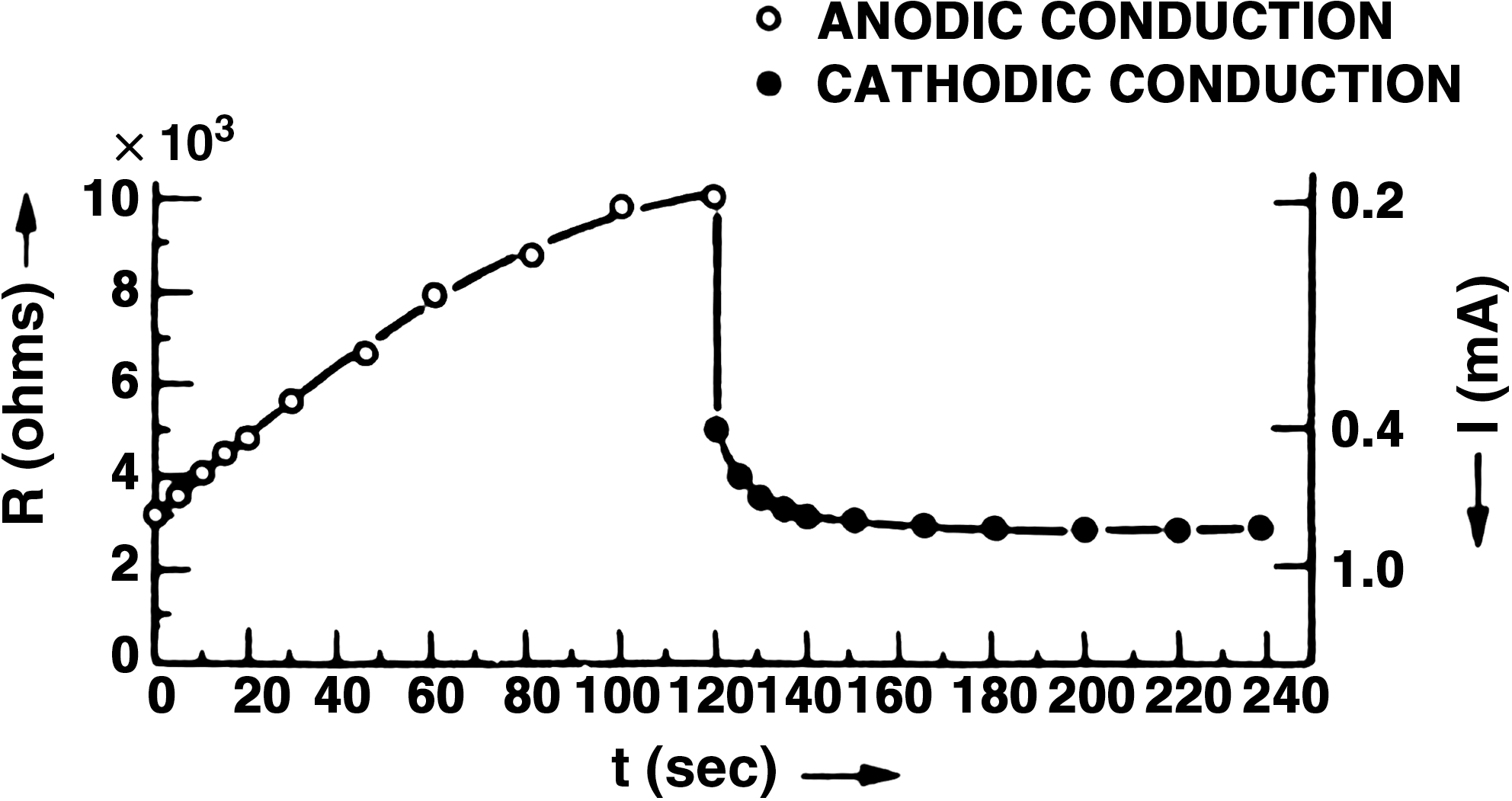
Time dependence of the electrical resistance at 2V (7 cm2 of skin moistened for 20 minutes with saturated KCl solution).

(
In this case, the simplest frequency-independent electrical equivalent circuit for skin measurements is given in Figure 6.

Simplest frequency-independent electrical equivalent circuit used for skin measurements.
However, via the use of AC conductance techniques, 8 both a high-frequency and a low-frequency diffusional admittance type of electrical equivalent circuit was observed, as illustrated in Fig. 7. 9
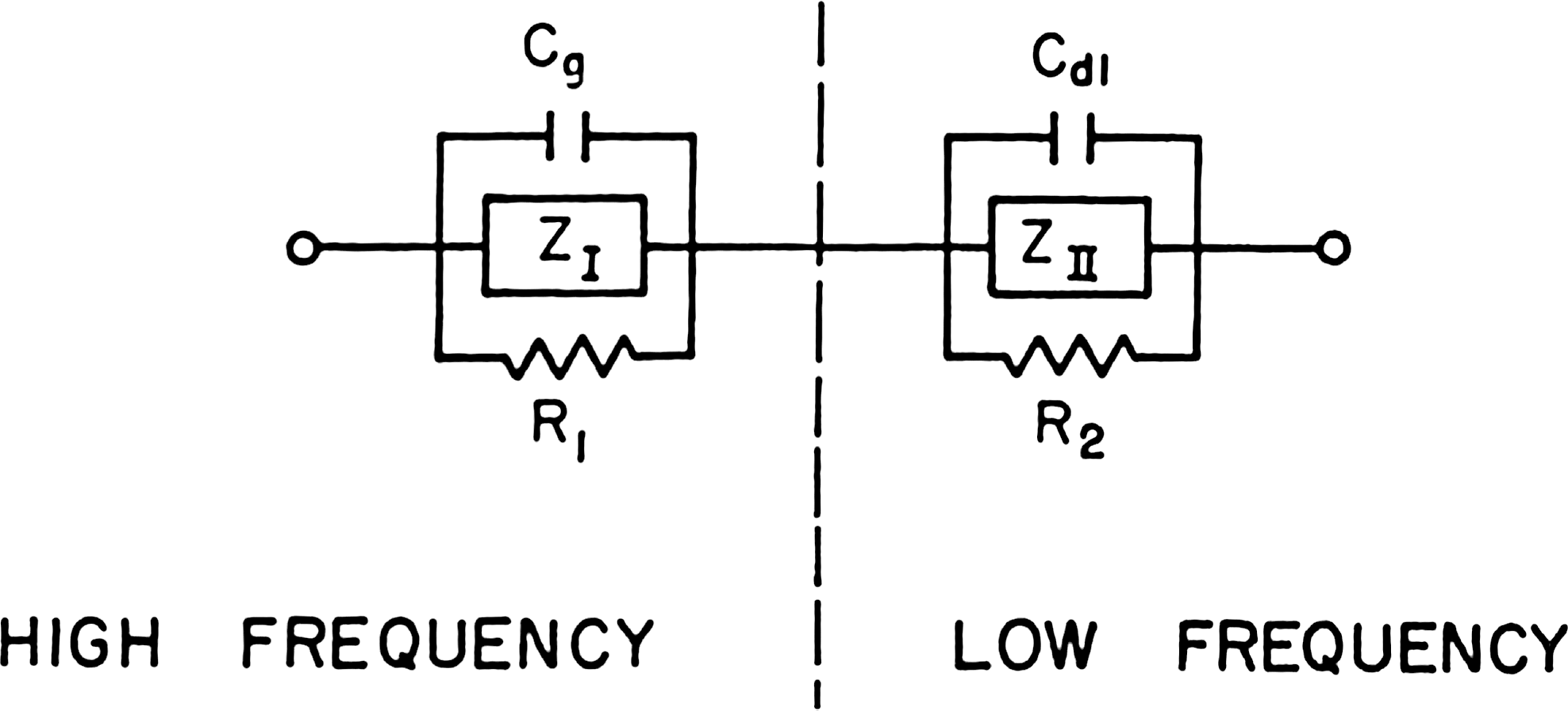
Electrical equivalent circuit generated from skin measurements using AC conductance techniques and complex plane analysis.
Probing still further, Motoyama discriminated (1) a short time-constant charge polarization process occurring at the basal membrane interface between the dermis and epidermis with τ2 ∼50 μsec and total interface voltage change of ∼1 V. In addition, (2) his experimental work reveals the presence of an electrical energy generator in the dermal connective tissues. 10 –13 Since his research was intimately related to the electrical responses associated with energy/information flows in acupuncture meridians, it connects directly to the αeffQm term in Part I Equation 1. 1 Connecting this basal membrane, τ2 time-constant process with the epidermis/stratum corneum, τ1, time-constant process of Figure 4, one obtains Figure 8 as the best approximation to a constant impedance parameters electrical equivalent circuit for the skin.

Electrical equivalent circuit for human skin approximated to constant impedance parameters.
In Figure 8, R1 is the resistance of the dermis, while V1 is its electrical energy generator (DC and AC), R2′ is the resistance of the basal membrane interface region of the epidermis while C1 is its capacitance, R3 is the resistance that allows for current leakage through this capacitor and R2′′ is the resistance of the stratum corneum while C2 is its local capacitance.
Since V1 in Figure 8 brings into play the coupled state of physical reality associated with the human body's acupuncture meridian system, Figure 8 must be expanded to include presently known details concerning the αeffQm contribution in Part I Equation 1 1 as it relates to an “effective” electrical equivalent circuit of the human skin when coupling between our two unique levels of physical reality must be taken into account. Although V1 in Figure 8 is symbolically represented as a DC battery, it is really an AC/DC system induced into the electrical dermis from the magnetic currents flowing in the “unseen” magnetic information wave level of physical reality. Thus, it should really be regarded as a complex impedance coupling term driven from a secondary source acting somewhat like the “secondary” circuit of a transformer. However, in this case it is a magnetic current, im, that flows in the secondary circuit element while it is an electric current, ie, that flows in the primary circuit element. This is metaphorically illustrated in Figure 9 where ZD is the effective electrical impedance of the dermis/epidermis/stratum corneum system and ZR is the effective magnetic impedance of the magnetic information wave system.
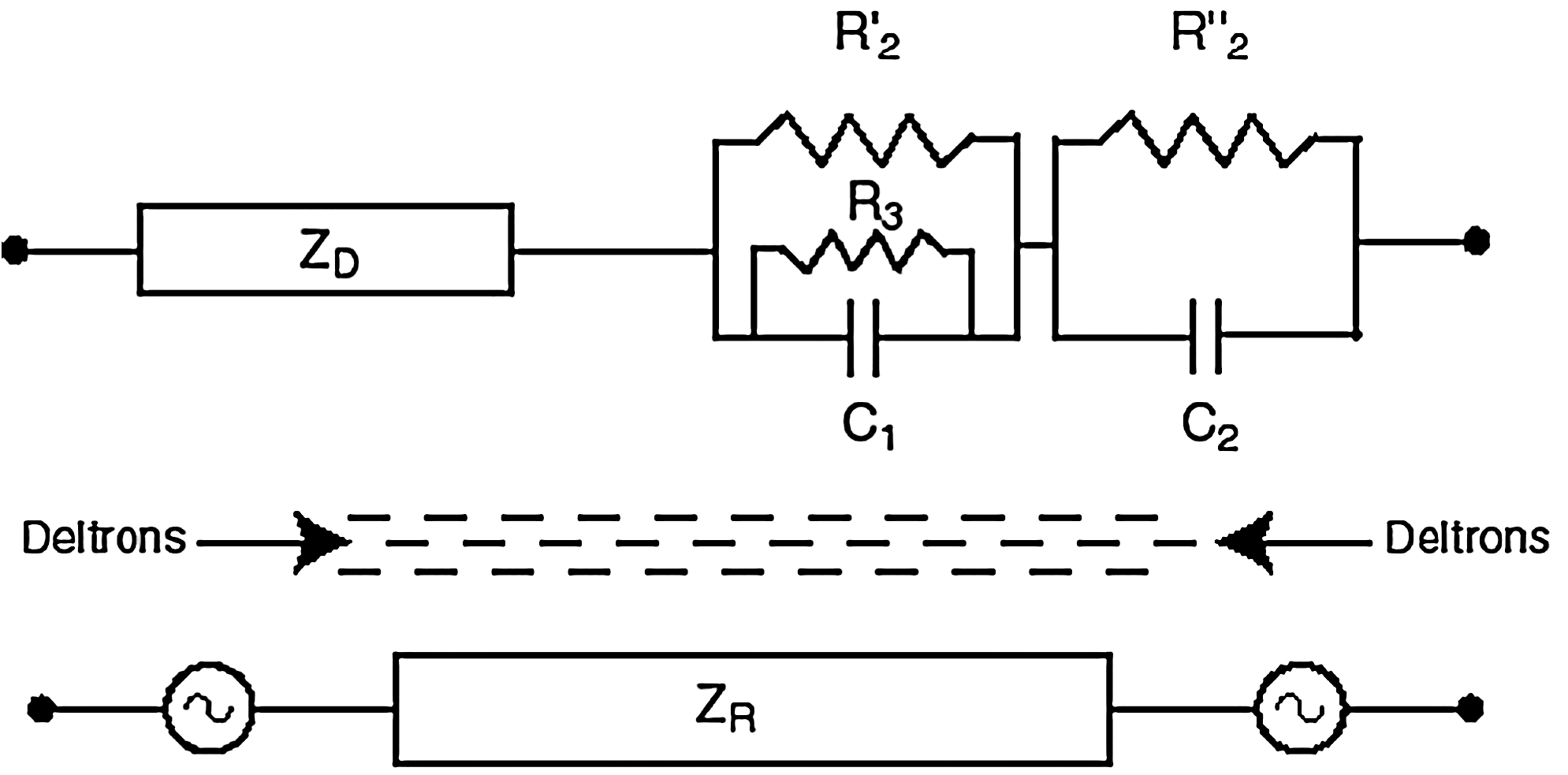
Proposed electrical equivalent circuit for human skin when the system is in the coupled state of physical reality. Here, Z is the impedance and the deltrons are the coupler medium.
When we apply our duplex reference frame (RF) to Figure 9 as the device in the Figure 1 system and also add a D-space test substance (neutraceutical, food substance, specific crystal, pharmaceutical, etc.) as one new contribution to the experimental system, the R-space contribution to Qm in Part, I Equation 1 1 grows by (1) the square of the R-space vector amplitude for this added D-space test object plus (2) the sum of pairwise R-space vector contributions between this D-space test object and each of the other R-space subsystem vectors in the overall system. Thus, if this D-space test substance is thermodynamically beneficial for the overall coupled system, a system response will appear in the (2) contributions above. Likewise, if this new contribution is detrimental to the system, the (2) contribution above is capable of indicating that.
If the practitioner in Figure 1 has a weak biofield and no other source of “space-conditioning” is present, αeff in Equation 2 will be negligible and the EM gauge symmetry state of the space will be very close to the Ue(1) state. The overall system will be in the uncoupled state of physical reality and any psychoenergetic usefulness of the electrodermal measurement responses will be very small.
In principle, if one goes further and represents the health of the client by the balance state of the client's 12 acupuncture meridians (which function in the client's R-space body), one can begin to recognize that a formal procedure exists to evaluate or anticipate the effect of various environmental factors on the state of health of the client's D-space organs.
Discussion
The main point that this author has been trying to make with this article and its predecessor, Part I, 1 is that traditional medicine and CAM build their practices on two, very different aspects of science and they both need to understand that. I and my colleague's experimental and theoretical research of the past decade has delineated these differences: (1) There are at least two unique levels of physical substance, not just one, occupying the same general space in our physical bodies but, normally, they are minimally interactive with each other. This leads to our normal, uncoupled state of physical reality. (2) The human acupuncture meridian/chakra system, functioning in the coarsest level of the physical vacuum (in the space between the fundamental electric particles that make up our electric atoms and molecules), are at the coupled state of physical reality. (3) Using intention–host devices, one can macroscopically “condition” a space, the measuring equipment contained within that space and, to some degree, humans occupying that space to the coupled state wherein the two uniquely different kinds of physical substance begin to significantly interact with each other. (4) The normal, uncoupled state of physical reality is the material medium addressed by most of orthodox medicine while the partially coupled state of physical reality is the material medium addressed by most of CAM.
The theoretical construct, invented by this author to understand the seemingly strange behavior of inorganic, organic, and living materials present in the coupled state of physical reality when human consciousness is utilized as a significant experimental variable, consists of two, reciprocal subspaces, one of which is space–time (D-space) while the other is a wave domain (R-space) with some level of a higher dimensional coupler substance activated. D-space is the home of positive mass and energy, electrically charged particles traveling at velocities slower than c, while R-space is the home of negative mass and energy, magnetically charged information waves traveling at velocities greater than c. When one expresses the thermodynamic behavior of the partially coupled duplex system in equation form, as in Appendix I, one sees allopathic-like thermodynamics dominating at large values of the intensive variables, homeopathic-like thermodynamics dominating at very small values of these same intensive variables, and some combination of both for intensive variable magnitudes in between.
As the amount of coupler substance shrinks toward 0, the duplex system separates into two noninteractive domains and only the allopathic-like world is cognitively accessibly by humans and our traditional measuring instruments. This leads to traditional science and traditional medicine. This leads to a world where one can expect randomized-controlled medical trials to be a rational strategy for experimentation. Likewise, in this domain, we have a great many traditional measurement instruments that can reliably access the relevant physics and chemistry that dominate the key electric/magnetic dipole processes of the human body.
On the other hand, as the amount of activated coupler substance substantially increases in nature, the duplex system of electric charge and magnetic charge begin to interact with each other, long-range connectedness effects begin to macroscopically appear; strong human intention effects begin to appear, human psychophysiologic and psychoenergetic effects begin to appear, nonrandom behavior in natural processes become a significant factor and many of these features are not accessed by our traditional measurement instruments. This is a physics and chemistry behavior quite different than that found in traditional science; it is a significant perturbation of that reality. In this world, one cannot expect (1) randomized-controlled medical trials to be a rational strategy for experimentation, or (2) that evidence-based medicine, gathered by traditional science-based instruments, can access all of the relevant data-streams involved in CAM practices. Today's problem for CAM is that there appears to be only one measurement instrument available to reliably discriminate between the uncoupled and coupled states of physical reality. 14
In this example section of Part II, not only does one see how the activation of the homeopathic effect arises through the presence of a significant value for αeff but that, to gain experimental insight into the details of homeopathy, one needs to measure the modified thermodynamic activity coefficient, γ*, at all phases of the process.
In the placebo effect, one sees the key factor involved in the R-space contribution to Qm; i.e., the vector summation of all the identifiable subsystem R-space vectors in the overall event and then the intensity vector for the whole system. Even though no electric D-space connections exist between the various subsystems, the R-space conjugates are connected via the pairwise R-space subsystem vector amplitudes and phase angles. One also sees in the electrodermal diagnostic testing device example how the introduction of a D-space testing substance to the client, as a new subsystem for the overall system, introduces an additional series of terms to the final result that indicates either a health improvement or a health diminishment factor.
The information entanglement example illustrates the importance of two key factors of this duplex space mathematics: (1) the deltron-modulated Fourier Transform pair relationships between the D-space object and its equilibrium R-space conjugate plus vice versa, and (2) the importance of R-space as a frequency domain. Although information entanglement is present in today's quantum mechanics, it is restricted to temperatures very close to absolute zero and to extremely small D-space object sizes. Here, room temperature, very large system sizes, and very long range (5000–6000 miles) information entanglement may somehow be related to quantum mechanics, but the connection is not yet obvious.
Finally, the connection of Figure 2 of Part I 1 to dark matter, dark energy, positive mass electric matter acceleration at the expanding edge of the universe and the possibility of human levitation is just an extra plus to validate the reasonableness of our particular duplex space model.
Conclusions
Traditional medicine's mindset and working arena is the uncoupled state of physical reality. CAM's working area is the coupled state of physical reality and its mindset needs to become psychoenergetic science. Both sets of practitioners need to become aware of the fact that data-gathering strategies that work well for uncoupled state physics do not work well for coupled state physics and vice versa.
Footnotes
Acknowledgment
The author wishes to sincerely thank Dr. Cyril Smith for his very timely help in editing this manuscript so as to make it more “user friendly” to the readership of this journal.
Disclosure Statement
The authors state that no competing financial interests exist.
Appendix I: Relevant Mathematics for Homeopathy
For the uncoupled state of physical reality, the U(1) EM gauge symmetry state, it is typical to expand various mathematical functions in a Taylor series expansion, provided there are no mathematical singularities within the domain of interest (within D-space). However, for the case where mathematical singularities do exist in the D-space domain of interest, one must use a Laurent series expansion
1
rather than the Taylor series expansion because, with the appropriate polynomial coefficients, one obtains a “singularity free” expression. Interestingly, this yields a very similar mathematical form as a Taylor series expansion to our special duplex space RF (reference frame) consisting of reciprocal three- or four-dimensional subspaces, one of which is space–time. Applying this approach to the Gibb's thermodynamic free energy function,
2
G, for a material in the partially coupled state of physical reality (0 < αeff < 1) as per Equation 1 of the main text of Part I, one can express G as an expansion about a domain G0, in terms of its intensive thermodynamic variables, to obtain
In Equations I-1 to I-3, the variable ξj represents all the thermodynamic intensive variables where P =; pressure, T =; temperature, c =; concentration, E =; electric field, H =; magnetic field, and g =; gravitational field. Equations I-1 and I-2 immediately distinguish the D-space allopathic contributions from the R-space homeopathic contributions to G.
From Equation I-2 with ξj =; concentration, one immediately sees that the homeopathic response is only significantly manifested when
If, for the moment, we consider the αeff =; 0 case and focus on ξ being only P, T, and c, one finds from well-known experimental results that
where V is the specific volume, S is the entropy of the system, and μ is the chemical potential of a particular species. Shifting our focus now to μ in Equation I-4, the general expression from G is
where
and where
Here E =; energy, ni =; number of species, i, per unit volume, (β1, β2, β3, β4 ) are all known coefficients, μ0i is the standard state chemical potential for the species i, a is the thermodynamic activity, a* is the modified thermodynamic activity, ln is the natural logarithm, exp is short for the exponential function, and k is Boltzmann's constant. When one takes the natural logarithm of ai * in Equation I-5c, Equation I-5b is reproduced.
Appendix II: Relevant Mathematics for the Placebo Effect
Here, we use Figure 1 as the most general example of a D-space medical interactive relationship and use it as a pedagogical vehicle for generating the R-space equilibrium counterpart for such a system event.
With r representing the D-space general spatial coordinate and k representing the R-space general spatial wave number, the standard Fourier Transform pair relationship for a D-space shape of the form f(r) is given by
and
With a deltron activation function of
and
This is how an equilibrium R-space conjugate is formed for a given D-space geometrical shape, G′(r), in the partially coupled state of physical reality when the deltron activation function is separable into the
To obtain the αeffQm term in Part I Equation 1, we first evaluate the intensity, I(k), and integrate it over all of R-space to obtain Qm. Then, we take general expansions of Cδ(r) and
and
Here G*(k) is the complex conjugate of the vector G(k).
Turning now to Figure 1 of the main text, there is only one component to Qe in Part I Equation 1
1
but five vector components for the R-space counterpart. Setting αeff =; the space gauge symmetry component in Figure 1, we now have Qm being determined by the other four vector contributions defined, with subscripts P, D, C, and U to represent, respectively, practitioner, device, client, and unseen. Therefore, the system vector, Rsexp(iθs), is given by the vector sum
The system intensity, Is(k), is given by
In Equation II-5b, the coordinate, k, has been left out for simplicity. The important point to note here is that, in the system intensity, which is all that one can expect to measure, we have six pairwise terms indicating that each term is connected to each other term and each subsystem has three neighboring interactions. For example, let us let the device be replaced by a placebo so that we can represent IS(k) by
where A is determined by subtracting Equation II-6 from II-5b. Thus, even if RD has only a nominal value, the bracket that multiplies it can be very large, so its activity effect in the system can be appreciable. This is how, in a typical doctor, treatment, placebo, subjects randomized clinical trial, the placebo group can never be isolated from the treatment group. Furthermore, the magnitude of the placebo effect depends on the size of the doctor effect, the treatment effect, and the subject effect.
If one is using just 1 subject (client) with the practitioner using a testing device on the subject and brings a sequence of food supplements X, say, into the field of the experiment, a series of new terms will enter IS (k), one for each of the other R-space subsystems in the overall system. In principle, one can use such a testing procedure to determine beneficial versus harmful reactions of the R-space aspect of X upon the R-space aspect of the client.
*
A system at constant temperature and pressure will reach equilibrium at a minimum of its components' Gibbs free energy G = E + PV − TS if the system's properties are determined both by the temperature T and by the pressure P, and at a maximum of their entropy S (E is the internal energy and V is the volume).