
Abstract
Objectives:
The study objectives were to determine whether methyl B12 treatment improves behavioral measures in children with autism and whether improvement is associated with increased plasma concentrations of glutathione (GSH) and an increased redox ratio of reduced glutathione to oxidized glutathione (GSH/GSSG), both of which have been previously identified to be low in children with autism.
Design:
This was a 12-week, double-blind, placebo-controlled, cross-over clinical trial of injectable methyl B12. Following this 12-week study, subjects were given the option of entering a 6-month open-label trial of methyl B12.
Settings/location:
All procedures took place at the UC Davis M.I.N.D. Institute.
Subjects:
Subjects were 3 to 8 years old with autism.
Interventions:
All subjects received 6 weeks of placebo and 6 weeks of methyl B12 at a dose of 64.5 mcg/kg every three days administered subcutaneously into the buttocks.
Outcome measures:
Blood for GSH analysis and behavioral assessments were obtained at baseline, week 6, and week 12.
Results:
Thirty (30) subjects completed the 12-week, double-blind study and 22 subjects completed the 6-month extension study. No statistically significant mean differences in behavior tests or in glutathione status were identified between active and placebo groups. Nine (9) subjects (30%) demonstrated clinically significant improvement on the Clinical Global Impression Scale and at least two additional behavioral measures. More notably, these responders exhibited significantly increased plasma concentrations of GSH and GSH/GSSG.
Conclusions:
Comparison of the overall means between groups suggests that methyl B12 is ineffective in treating behavioral symptoms of autism. However, detailed data analysis suggests that methyl B12 may alleviate symptoms of autism in a subgroup of children, possibly by reducing oxidative stress. An increase in glutathione redox status (GSH/GSSG) may provide a biomarker for treatment response to methyl B12. Additional research is needed to delineate a subgroup of potential responders and ascertain a biomarker for response to methyl B12.
Introduction
Methyl B12 is a vital cofactor for the regeneration of methionine from homocysteine by providing methyl groups for the transmethylation metabolic pathway. 8 Methyl B12 deficiencies, therefore, can result in increased levels of homocysteine and low levels of methionine and S-adenosylmethionine (SAM), producing cytotoxic effects. SAM deficiencies may further contribute to the accumulation of homocysteine by restricting the transulfuration pathway, as SAM stimulates the activation of cystathione beta synthase. 9 Reduced synthesis of the products of the transulfuration pathway, including cysteine and glutathione (GSH), may consequently lead to decreased antioxidant capacity 8 (Fig. 1). GSH dysregulation may be of particular significance, as GSH is a key antioxidant responsible for minimizing macromolecular damage produced by oxidative stress. 10
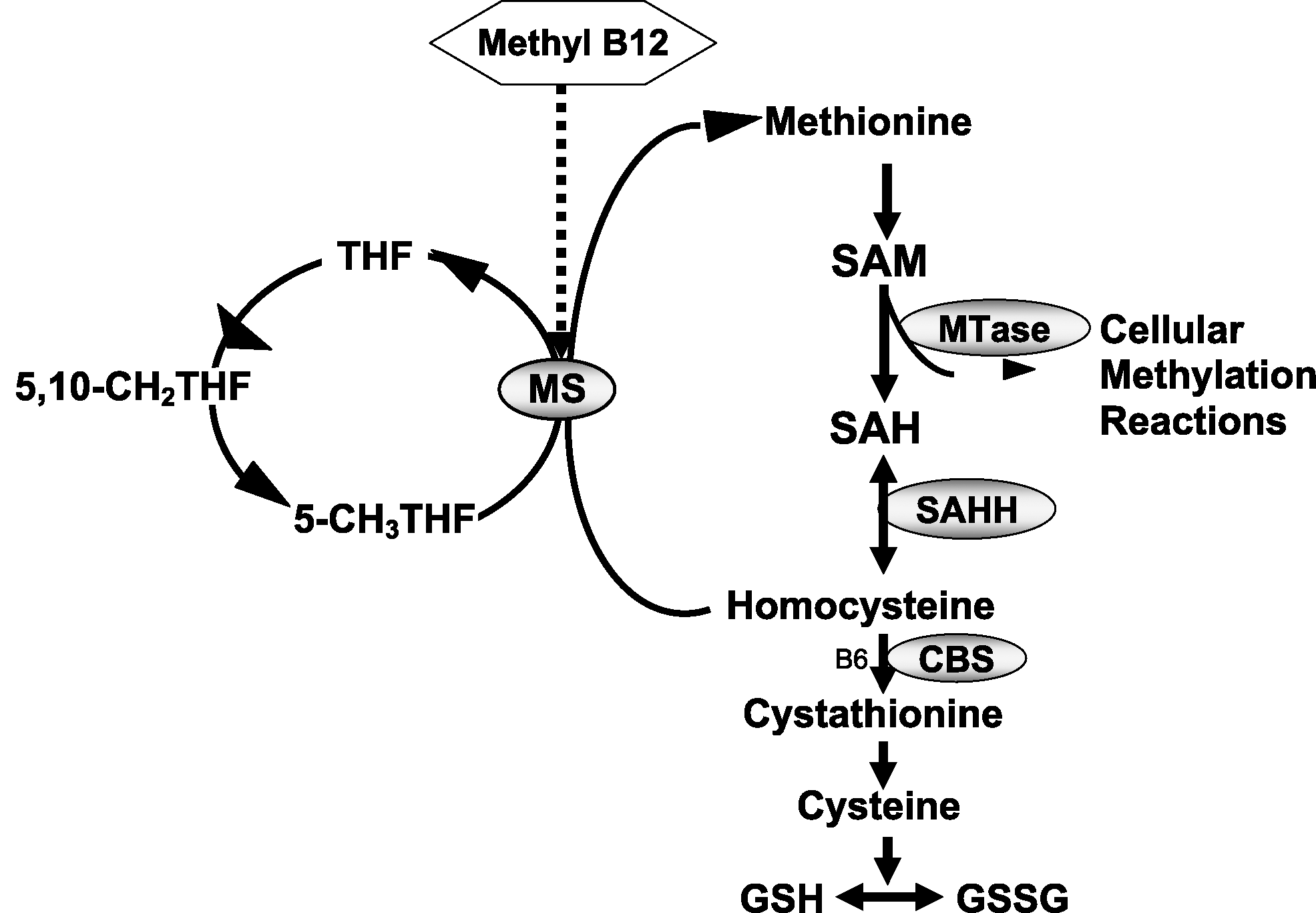
The methionine transmethylation metabolic pathway. The methionine cycle involves the remethylation of homocysteine to methionine by either the folate–vitamin B12-dependent methionine synthase (MS) reaction or the folate-vitamin B12-independent betaine homocysteine methyltransferase (BHMT) reaction. Methionine is then activated by methionine adenosyltransferase (MAT) to S-adenosylmethionine (SAM) the major methyl donor for cellular methyltransferase (MTase) reactions. After methyl group transfer, SAM is converted to S-adenosylhomocysteine (SAH), which is further metabolized in a reversible reaction to homocysteine and adenosine. Homocysteine may be permanently removed from the methionine cycle by reversible conversion to cystathionine by vitamin B6-dependent cystathionine synthase (CBS). Cystathionine is converted to cysteine, which is the rate-limiting amino acid for the synthesis of the tripeptide glutathionine (Glu-Cys-Gly). THF, tetrahydrofolate; 5-CH3 THF, 5-methyltetrahydrofolate; SAHH, SAH hydrolase.
James et al. recently showed that many children with autism exhibit low levels of GSH and a decreased GSH/GSSG redox ratio. 11 Furthermore, in a small, open-label trial, it was demonstrated that 1-month administration of methyl B12 resulted in a significant increase in plasma GSH concentrations; however, behavioral assessments were not done in this study. 10 To date, no published studies are available to support the reported clinical benefit of methyl B12 in autistic children. This study aimed to determine whether methyl B12 supplements improve behavioral symptoms of autism, and if improvement is associated with improved glutathione redox status.
Materials and Methods
Participants and study procedures
This 12-week, double-blind, placebo-controlled, cross-over study was funded by the UC Davis M.I.N.D. Institute. Thirty (30) children between the ages of 3 and 8 years with autism were recruited to participate from clinical referrals and an internal database through which families request to be contacted for studies for which their child might qualify. Children who were currently taking methyl B12 were excluded, and all participants committed to not change or add any treatments during the 12-week study. All subjects were required to have a nonverbal IQ of 49 or above, confirmed by the Wechsler Preschool and Primary Scale of Intelligence, Mullen Scales of Early Learning, or the Wechsler Intelligence Scale for Children conducted by a licensed psychologist. A diagnosis of autism in all participants was confirmed by the Diagnostic and Statistical Manual-IV: TR criteria, as well as the Autism Diagnostic Observation Schedule 12 conducted by a licensed psychologist trained to research reliability. If any diagnostic questions arose after the above were completed, the Autism Diagnostic Interview Revised 13 was also conducted, followed by diagnostic agreement from a consensus rater's meeting (RH and LD) reviewing all available diagnostic information.
All study procedures were approved by the UC Davis Institutional Review Board. Following signed consent, subjects were randomly assigned by the UC Davis Investigational Drug Pharmacy to either initial treatment with methyl B12 for 6 weeks followed by a 6-week placebo (saline) treatment, or an initial 6-week placebo, followed by 6 weeks of active methyl B12 treatment. All subjects attended visits at baseline, 6 weeks, and 12 weeks for a blood draw, clinical assessments, dispensing methyl B12, and safety monitoring. Clinical assessments were administered by a licensed psychologist or an experienced clinician trained to reliability, and included the Parent Interview for Autism–Clinical Version (PIA-CV), 14 Clinical Global Impression Scale of Improvement (CGI-I), 15 Childhood Autism Rating Scale (CARS), 16 Peabody Picture Vocabulary Test-Third Edition (PPVT-III), 17 Stanford Binet Fifth Edition Routing Subsets, 18 Aberrant Behavior Checklist (ABC), 19 Child Behavior Checklist (CBCL), 20 and the MacArthur Communication Developmental Inventory (MCDI). 21 Following the initial 12-week, double-blind study, subjects had the option of entering a 6-month, open-label extension study, during which they returned at 3 and 6 months for visits involving clinical assessments. The primary outcome measure was the CGI (0–7-point scale). Secondary outcome measures include assessments of communication, social reciprocity, and behavior. Cutoffs used to define improvement on all outcome measures were determined through consultation with the study psychologist (LD) prior to data analysis (see Results).
Methyl B12 dosing and administration
Parents administered a dose of 64.5 μg/kg of methyl B12 or placebo, which was administered by the parents every 3 days for 6 weeks in each treatment arm, then switched without washout by means of subcutaneous injection into alternating buttocks at night while their child was sleeping. All parents were trained to administer the injections by the principal investigator (RLH). The syringes were covered with an opaque material in order to protect the stability of methyl B12, which is photo labile, and to mask the active injections from the placebo injections. The methyl B12 and placebo dispensed for study treatment were prepared and donated by Wellness Pharmacy, chosen by the UC Davis Investigational Drug Services from several potential laboratories for their product sterility and consistency. Parents were advised that they would randomly encounter different colors of the solution injected.
Blood analysis
Fasting blood samples were collected into ethylenediaminetetraacetic acid-containing (EDTA) evacuated tubes and immediately chilled on ice before being centrifuged at 4000 × g for 10 minutes at 4°C. Plasma aliquots were transferred into cryostat tubes and stored at −80°C. Samples were then shipped to the laboratory of Dr. Jill James at Arkansas Children's Hospital for extraction and blinded analysis by high-performance liquid chromatography. Glutathione and other metabolites were measured by the same methods described by James and colleagues. 11
Statistical analysis
The study was designed with 80% power to detect a 40% improvement in the methyl B12 group compared to a 10% improvement in the placebo group. Paired sample t-tests were conducted between active and placebo groups on both blood and behavioral measures. Paired sample t-tests were also conducted to compare GSH and GSH/GSSG measures between placebo versus active treatment arms within the responder group and within the nonresponder group. Chi-square analyses were conducted to detect any difference between responders and nonresponders on frequent infections, gastrointestinal symptoms, or food allergies.
Results
A total of 30 subjects, 28 males and 2 females, completed the 12-week, double-blind study. Twenty-two (22) subjects (73%) chose to enter the 6-month extension study. Side-effects were limited to increased hyperactivity and increased mouthing of objects. No serious adverse events were reported. No statistically significant differences in the overall means for behavior or glutathione endpoints were identified between active and placebo groups. Data were analyzed using only those who had placebo first in the placebo group (n = 17 out of the 30 total) but significance was not reached, possibly due to the small size of this group.
Responder subgroup
Although no overall significant difference was identified between active and placebo groups through whole group analysis, a subgroup of children responded remarkably well to what we learned was the active treatment group. A subset of 9 subjects (30%; 3 who received placebo first; 6 active first) exhibiting substantial improvements were identified as “responders” based on clinically significant improvement on the CGI and at least two additional behavioral measures (Fig. 2 and Table 1). These responders significantly improved from baseline when they were on active treatment, and showed no significant improvement from baseline to placebo. Three (3) of the 9 subjects in this responder subgroup received active drug for the first 6-week treatment arm, and 6 of the 9 subjects received active drug during the second 6-week treatment arm. Clinical significance for these measures was defined as an improvement of at least 1 point on the CGI, 10 points on the PIA-CV and CBCL, 5 points on the PPVT-III, MCDI, and ABC, or 2 points on the CARS. This responder subgroup also showed significantly improved GSH (p = 0.008) and GSH/GSSG (p = 0.028) (Figs. 3 and 4). Comparatively, the placebo group included 3 subjects (1%) identified as “responders” based on positive response to behavioral measures described above. However, the small number of placebo responders is not sufficient to identify any statistically significant difference in measures of glutathione. Chi-square analysis suggests no significant association between response status (response versus no response) and frequent infections, gastrointestinal symptoms, or food allergies. Glutathione analysis was conducted on 11 subjects due to sample hemolysis during the blood draw. However, none of these subjects with hemolysed blood were qualified as responders.
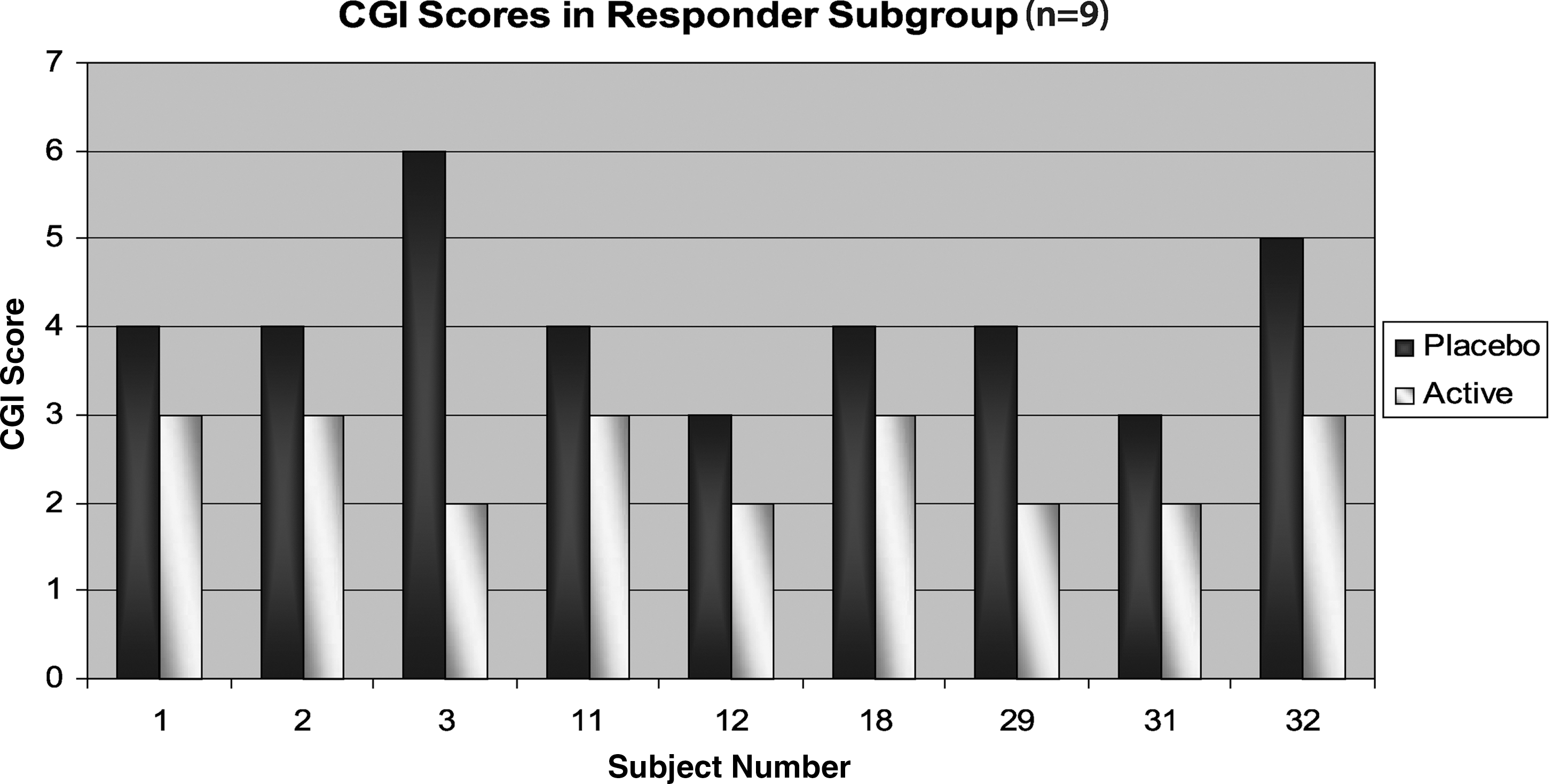
Clinical Global Impression Scale (CGI) scores at active and placebo arms in the responder subgroup. Lower scores indicate improvement.
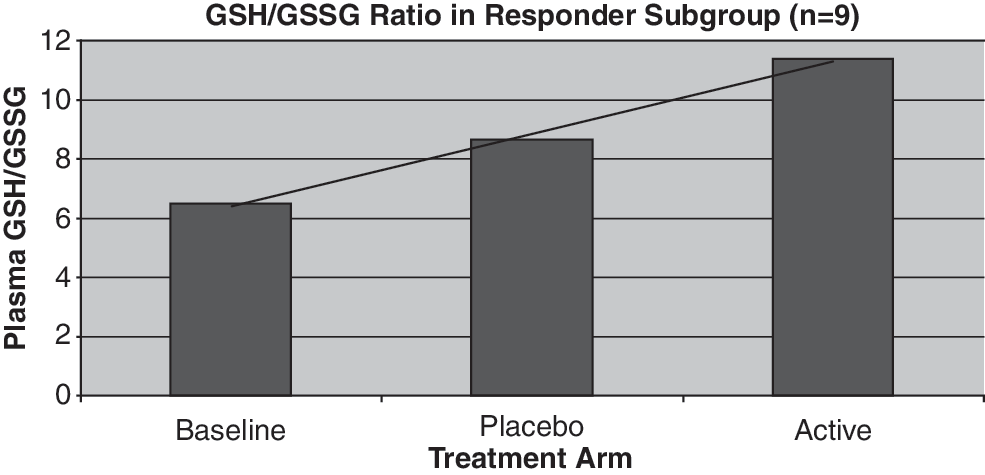
Ratio of plasma glutathione to oxidized glutathione (GSH/GSSG) in responder subgroup at baseline, placebo, and active treatment arms (p = 0.028).

Plasma glutathione (GSH) in responder subgroup at baseline, placebo, and active treatment arms (p = 0.008).
CGI, Clinical Global Impression Scale; PIA-CV, Parent Interview for Autism Clinical Version; PPVT-III, Peabody Picture Vocabulary Test-Third Edition; ABC, Aberrant Behavior Checklist; CBCL, Child Behavior Checklist; MCDI, MacArthur Communication Developmental Inventory; SB, Stanford Binet: V Edition.
Discussion
These pilot data provide the suggestion of a positive response to methyl B12 in a subgroup of children with autism. Autism spectrum disorders encompass many different subgroups, each of which may have a different response to treatment. However, there is not yet enough information on the etiology or treatment of autism to clearly define and identify these subgroups. Therefore, treatment research studies conducting only whole-group analysis—comparing placebo to active in a group of children with autism—may overlook a subgroup of treatment responders in an autism subgroup, displaying a false negative for treatment efficacy.
Although no significant overall mean difference was identified between active and placebo groups, 30% of subjects enrolled in the study displayed substantial positive responses to methyl B12. Additionally, this responder subgroup exhibited significant improvement in blood plasma levels of glutathione, indicating a potential biomarker of response and a mechanism of improvement, which may include increased antioxidant capacity and reduced oxidative stress. The improved redox ratio of reduced to oxidized glutathione (GSH/GSSG) replicated findings in the James study and reflects an equilibrium shift from a more pro-oxidant environment toward a more reducing environment associated with a decrease in oxidative stress. 22 These observations in a significant subgroup of children suggest that the responder subgroup may have been diluted out in the whole group analysis. We began the study using a cross-over design in hopes of best utilizing the small number of subjects with limited funding. We now recognize that the cross-over design may have limited the data. When analyzing the data from only the first 6 weeks of the study in an attempt to eliminate the effects of the cross-over, no significance resulted between active and placebo groups. However, we argue that this is due to analyzing such a small sample size (15 subjects) as opposed to the cross-over design. There are no data yet showing that methyl B12 improves the symptoms of autism, let alone how long the improvements last. However, if subjects in the active treatment arm during the first 6 weeks of the study continued to improve during the second 6 weeks, the data would tend to show there is less benefit of methyl B12, as there would be less of a difference between active and placebo groups. Therefore, the limitations of the cross-over design has, if anything, contributed to diminish significance between active and placebo groups, as opposed to accentuating significance.
It is important to note that a positive response to B12 supplementation in our study does not presume overt B12 deficiency. Under conditions of severe deficiency, the hepatic B12 stores are mobilized to maintain adequate plasma and intracellular levels. 23 Severe B12 deficiency is documented by elevated methylmalonic acid levels, which have not been reported in children with autism. Rather, it is our hypothesis that weekly high-dose B12 supplementation is most likely addressing abnormal one-carbon metabolism and altered metabolic priorities in autistic children as previously reported. 11 One possibility is that intracellular transport of dietary sources of B12 may be compromised in autistic children. Supporting this possibility, the frequency of a polymorphism in the transcobalamin II gene (TCN2 C776G) that codes for the B12 transport protein is increased in many autistic children. 11 Weekly supplementation with methyl B12 may improve intracellular B12 transport efficiency by mass action in a subset of children and thereby indirectly improve glutathione status. Liver stores would not be mobilized with a transport deficiency because plasma B12 can be normal despite intracellular deficiency. A similar scenario has been documented for plasma folate levels, which can be normal or elevated when there is a block in transport or utilization of folate. 24,25 Thus, we believe that mobilization of liver B12 stores is not an issue in the cross-over design in the present study.
Future studies may more effectively delineate a responder subgroup by an improved study design. Seventy-three (73%) percent of parents observed enough benefit to choose to continue methyl B12 in the extension study, suggesting that all improvements may not have been captured by the measures used. Given that many of the children were low functioning, some measures lack the sensitivity to pick up subtle changes observed. In the future, utilizing measures that are able to identify these subtle benefits, such as improved attention, may more effectively capture change. The cross-over design with 6-week treatment arms and no washout may also have contributed to an underreporting of positive results in this study. Many parents, and study psychologists, reported recognizing when a subject was on active medication, but observed improvements were not lost after crossing over to the placebo treatment arm. Therefore, although no additional improvements were reported during the placebo treatment arm, many subjects receiving active treatment during the first 6 weeks did not lose skills reportedly acquired from active methyl B12 administration. Consequently, many of these subjects demonstrated improvement on both active and placebo arms. This confounding factor may have limited the ability to differentiate active from placebo, as the placebo may reflect improvement resulting from methyl B12 administration in the active treatment arm. Based on these preliminary results, true separation between active and placebo, or a more clearly defined responder subgroup may be revealed in a larger, double-blind, placebo-controlled study designed without a cross-over or with a washout period between treatment arms.
Conclusions
These preliminary results indicate a strong trend toward improvement following methyl B12 administration in a subgroup of children with autism, warranting further research into the efficacy of methyl B12 and potential biomarkers of response to this treatment. The mild nature, and limited number of side-effects observed, supports that subcutaneous administration of methyl B12 appears safe to use in this population. Although these preliminary results indicate a trend toward improved symptoms after supplementation with methyl B12, larger sample sizes in a parallel group design are needed to better characterize a subgroup of responders, as well as to determine statistically significant efficacy between active and placebo groups. Longer, double-blind treatment arms will allow the assessment of whether longer administration of methyl B12 results in additional improvements.
Footnotes
Acknowledgments
The authors would like to thank and acknowledge The Medical Investigation of Neurodevelopmental Disorders (M.I.N.D.) Institute of the University of California, Davis Medical Center, for providing funding for this study and to Deb Matsumoto for her assistance in preparing the manuscript.
Disclosure Statement
No competing financial interests exist.