
Abstract
Background:
Saireito consists of components of shosaikoto and goreisan. There are several reports of liver injury caused by shosaikoto and saireito, whereas cases caused by goreisan are rarely seen.
Patient:
A 70-year-old woman suffered from sicca of the eyes and oral cavity that arose in 2003. In June 2004, we diagnosed her as having Sjögren syndrome on the basis of Schirmer's test, salivary scintigraphy, presence of anti-SS-A/Ro antibody, and subjective symptoms. Although a muscarinic agonist was commenced, her sicca symptoms did not improve.
Interventions:
In February 2008, 7.5 g/day of shosaikoto extract granules (for ethical use, Tsumura & Co., Tokyo, Japan) was introduced. Her symptoms and laboratory data did not change. The next month, the treatment was replaced by 9.0 g/day of saireito extract granules (for ethical use, Tsumura & Co., Tokyo, Japan).
Results:
After 10 weeks, elevation of liver enzymes was observed. On suspicion of drug-induced liver injury (DILI), saireito was withdrawn, and the patient's liver enzymes returned to normal the next month. Drug-induced lymphocyte stimulation tests (DLSTs) for saireito, shosaikoto, and goreisan were all positive.
Conclusions:
The clinical course suggested allergy to the goreisan component of saireito. It is important to be aware of the limitation of DLST as a diagnostic tool for DILI, especially for herbal medicines.
Introduction
In SjS cases, various autoantibodies are detected. Among these autoantibodies, anti SS-A/Ro antibody may be related to drug allergy. Many reports showed cases positive for anti-SS-A/Ro antibody accompanied by allergy to anticonvulsants, 3 sulfa drugs, 4 antirheumatic drugs, 5 and anticancer agents. 6
We experienced a case of allergy to a Kampo medicine accompanied by SjS positive for anti-SS-A/Ro antibody. To diagnose drug allergy, we performed drug-induced lymphocyte stimulation tests (DLSTs). However, there was a discrepancy between the results of the DLSTs and the clinical course. We discuss here several problems related to the diagnosis of drug allergy to herbal medicines.
Case Report
A 70-year-old woman had suffered from xerostomia and xeroophthalmia since 2003. She had no specific medical history. She was a housewife and a lifelong nonsmoker. There was no family history of collagen vascular disease.
She visited a hospital in June 2004. A physical examination revealed dry mouth with atrophic lingual papillae. Ophthalmological examination findings included positive Schirmer's tests (less than 5 mm per 10 minutes bilaterally), and positive rose bengal and fluorescein tests, suggesting keratoconjunctivitis sicca bilaterally. Results of laboratory data revealed an antinuclear antibody level of 1280 × (discrete speckled pattern), a positive finding for anti-SS-A/Ro antibody, but negative findings for anti-SS-B/La antibody, anti-DNA antibody, and C-reactive protein (Table 1). Salivary scintigraphy revealed no accumulation in parotid and submandibular glands, which suggested extreme hypofunctioning of the salivary glands.
Reference ranges are shown in parentheses.
On the basis of these facts, a diagnosis of SjS was made. Although 90 mg/day of cevimeline hydrochloride hydrate was commenced, the patient's sicca symptoms did not improve, and she concomitantly needed external use of artificial saliva and tear fluid.
In October 2006, the first Japanese herbal medicine, 7.5 g/day of rokumigan extract granules (for ethical use, Tsumura & Co., Tokyo, Japan), was introduced. She continued to take rokumigan for 6 months. However, her symptoms did not improve and she finally stopped taking the medicine.
In February 2008, she was still troubled with xerostomia and xeroophthalmia, which became exacerbated, especially in winter. For the purpose of correction of immunological abnormality, 7.5 g/day of shosaikoto extract granules (for ethical use, Tsumura & Co., Tokyo, Japan) was introduced. In March 2008, the shosaikoto seemed to have caused no change in her symptoms, so shosaikoto was switched to 9.0 g/day of saireito extract granules (for ethical use, Tsumura & Co.). Saireito includes the components shosaikoto and goreisan (Table 2). One of the classic indications of saireito and goreisan is relief of thirst. In the latter half of May 2008, a blood analysis was performed, and revealed elevation of liver enzymes, especially alkaline phosphatase and γ-glutamyl transpeptidase (Fig. 1). Such abnormal findings were not observed until March 2008. The patient had not experienced any new symptoms, and physical examination did not show any sign of jaundice. Ultrasonography of the abdomen showed no abnormal finding. Viral infections related to hepatitis were ruled out by serological tests. Suspecting drug-induced liver injury (DILI), we decided to stop all treatment with Japanese herbal medicines. Blood tests performed the next month confirmed normalized liver enzymes (Fig. 1).
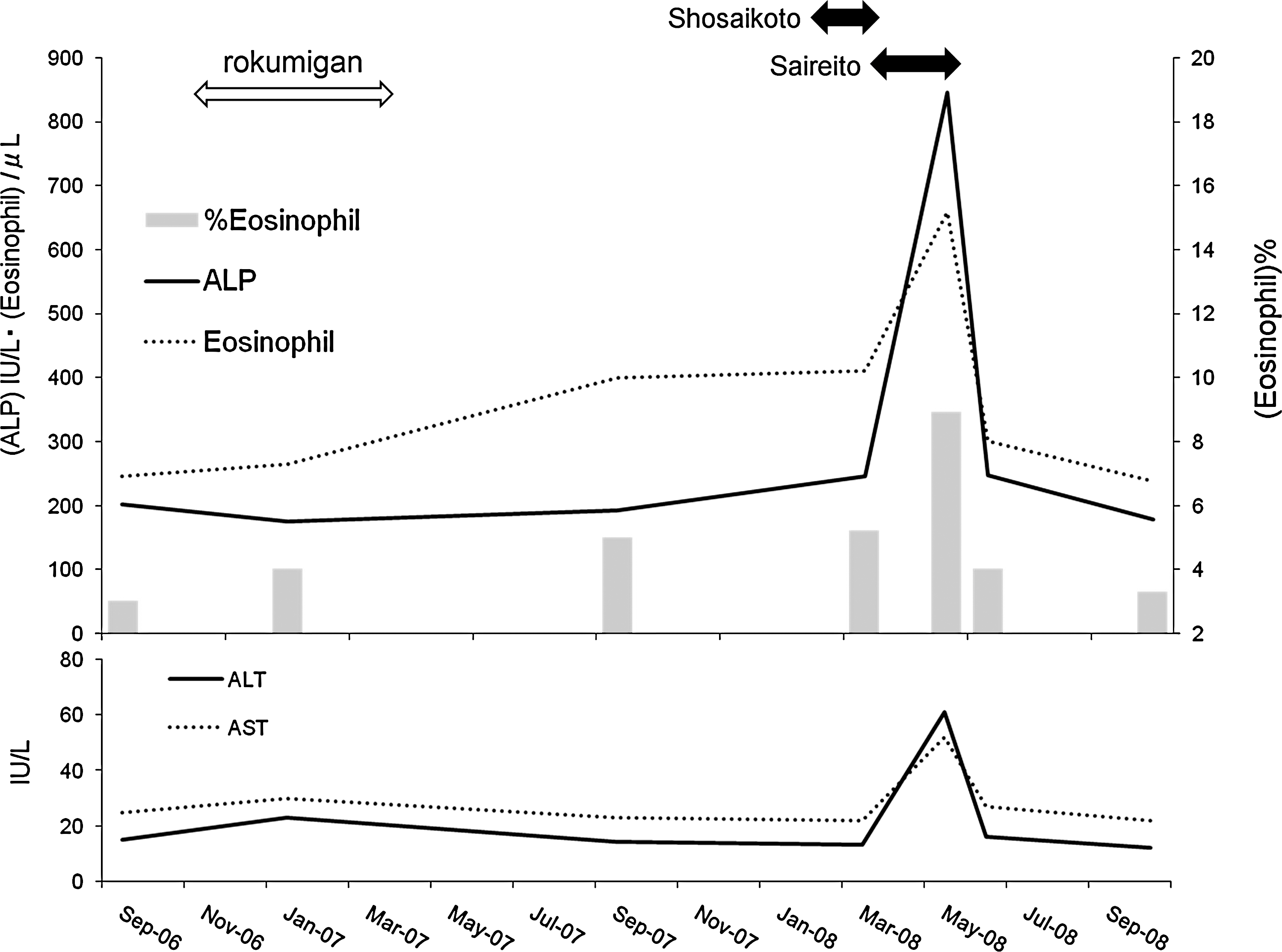
Clinical course of this case. ALP, alkaline phosphatase; ALT, alanine transferase; AST, aspartate transferase.
—, none.
DLSTs for Japanese Herbal Medicines
In February 2009, to determine the cause of the liver injury, we requested that Bio Medical Laboratories (BML) perform DLSTs for shosaikoto, saireito, and goreisan.
Briefly, peripheral blood mononuclear cells were isolated from the patient's peripheral blood, by density gradient centrifugation, and washed in serum-free RPMI 1640. The cells were resuspended in culture medium supplemented with 20% plasma from the patient. Various concentrations of the three Kampo medicines, which were sterilized with a filter before use, were incubated with 1 × 106 cells/mL for 3 days. Phytohemagglutinin was employed as a positive mitogen control. The proliferative response was assessed by measuring 3 H-thymidine incorporation. Radioactivity was measured by liquid scintillation spectrometry. The stimulation index was defined as “counts per minute (cpm) with allergen/cpm of negative control.” The DLST was considered positive if the stimulation index was 1.8 or more, according to the criteria recommended by BML. The stimulation indexes for shosaikoto, saireito, and goreisan were 22.7, 21.0, and 7.1, respectively (Table 3).
The stimulation index was defined as 3H-thymidine counts per minute (cpm) with allergen/cpm of negative control. The DLST was considered positive if the stimulation index was 1.8 or more.
PHA, phytohemagglutinin.
Discussion
According to a review of 1676 DILI cases by the Japanese Society of Hepatology, 7 64 cases (7.1 %) were caused by herbal medicines. On the other hand, the most frequent causes of DILI were antibiotics (14.3%), psychiatric and neurological drugs (10.1%), and dietary supplements (10.0%). Mantani et al. 8 studied the incidence of liver injury related to Kampo medicine in 2496 cases for 20 years. The authors estimated that the incidence of DILI in all cases treated with prescribed Kampo medicines was a maximum of 0.6%. Compared with other medicines, this value is not so high.
So far, several criteria of DILI have been proposed. In 1993, an international consensus meeting defined a scoring scale for evaluating DILI. 9 The criteria consisted of time to onset, course of the reaction, risk factors, concomitant drugs, search for nondrug causes, previous information on hepatotoxicity of the drug, and response to readministration. In our case, the score is 8, so it is classified as a “probable” case (Table 4). In 2004, Takikawa and Onji 10 modified the conventional scale. They added eosinophilia (more than 6%) and DLST, and omitted concomitant drugs and age as risk factors. On the basis of their analysis of 683 DILI cases, 11 they concluded that the sensitivity and specificity of the scale were 98.7% and 97.0%, respectively. According to this scale, the score in our case is 10, so it is classified as a “high possibility” (Table 5).
These scores obey the scales of cholestatic type, which consist of the following items: (1) Time to onset from the beginning of the drug; (2) course of the reaction (after cessation of the drug, alkaline phosphatase [ALP] decreased within 180 days > 50%, +2; < 50%, +1; persistence or no information, 0); (3) risk factor; (4) concomitant drugs; (5) search for nondrug causes (among recent hepatitis A, B, and C virus infections, biliary obstruction, alcoholism, and acute hypotension history, all ruled out, +1; 5 or 4 ruled out, 0; less than 4 ruled out, −2); (6) previous information on hepatotoxicity of the drug (labeled in the product characteristics, +2; published but unlabeled, +1; unknown, 0); and (7) response to readministration. Scores are classified according to 5 degrees: ≤ 0, relationship “excluded”; 1–2, “unlikely”; 3–5, “possible”; 6–8 “probable”; above 8 “highly probable.”
ALP doubled with the drug alone, +3; and ALP doubled with the drugs already given at the time of the first reaction, +1.
ALP increased less than normal upper limit, −2.
DILI, drug-induced liver injury.
These scores obey the scales of cholestatic type, which has 1, 2, 4, 5, and 6 items common to ICM criteria. Scores are classified according to 3 degrees: ≤ 2, “low possibility”; 3–4, “possible”; above 4, “high possibility.”
ALP doubled with the drug alone, +3; and ALP doubled with the drugs already given at the time of the first reaction, +1.
ALP increased less than normal upper limit, −2.
DILI, drug-induced liver injury; ALP, alkaline phosphatase.
Aiba et al. 12 reported on saireito-induced liver injury and concluded that Pinelliae tuber was the causative agent. Mantani et al. 8 showed that Kampo medicines including Scutellariae radix and/or Bupleuri radix were prescribed in 11 cases (73%). These crude drugs are contained in shosaikoto. However, in our case, liver enzymes did not change during treatment with shosaikoto; liver injury appeared after shosaikoto had been replaced by saireito. Thus, the goreisan component of saireito seemed to cause liver injury. DILI caused by goreisan is quite rare. Although there are several reports 8,13 about DILI caused by shosaikoto and information about hepatotoxicity is listed on the product label, there is no published or product label information about DILI caused by goreisan.
Although we performed DLSTs to determine a causative agent, the results were positive for shosaikoto, saireito, and goreisan. Some experimental evidence suggests that Kampo medicines that contain B. radix, such as saireito and shosaikoto, may tend to cause a false-positive reaction for DLST. Hot water extracts of B. radix show mitogenic activity to murine lymphocytes. 14 The mitogenic activities were especially strong in large molecular weight subfractions containing polyphenolic compounds and polysaccharide. 15 These facts demonstrate that DLST, regarded as a useful tool to diagnose DILI, may not be useful to determine causative agents.
Conclusions
We report a case of saireito-induced liver injury accompanied by Sjögren syndrome. Although the clinical course suggested that the goreisan component of saireito is causative, the results of DLSTs were positive for all components of the Kampo medicines administered. We think that it is important to be aware of the limitation of DLST as a diagnostic tool for DILI, especially for herbal medicines. However, this report is a single case study. Further studies in a larger case series are required to elucidate the optimal diagnostic method of DILI caused by herbal medicines.
Footnotes
Disclosure Statement
This work was supported by a Grant-in-Aid for Scientific Research (C) (20590712).