
Abstract
Background:
Electro-acupuncture (EA) can be effective in some pain conditions, but still there have been no randomized controlled studies of EA for treatment of acute postoperative pain in nasal septoplasty. Therefore, we did a study to test whether EA of specific points is superior to sham acupuncture for complementary analgesia after nasal septoplasty.
Methods:
Ninety (90) patients with an American Society of Anesthesiology (ASA) physical status of I–II scheduled for elective septoplasty were randomly allocated to acupuncture group or control group. Postoperative pain was treated with intravenous meperidine. The time to the first analgesic request, and pain intensity on a 100-mm visual analogue scale (VAS-100) were used to evaluate postoperative pain, and the amount of postoperative meperidine and incidence of analgesia related to side-effects were recorded.
Results:
Postoperative pain intensity on VAS-100 and respiratory depression were similar in both groups (p > 0.05), but nausea and vomiting were less in the acupuncture group than in the control group (p < 0.05).
Conclusions:
Findings from our study demonstrate that both uses of EA and 0.1 mg/kg IV morphine given intraoperatively resulted in a similar postoperative pain score, and meperidine was not given in any patient in the two groups during postoperative period because the VAS scores of all patients were less than 40 mm.
Introduction
Acupuncture analgesia is a technique directed toward the relief of pain and regulation of the physiologic function of the human body by needling. 7 Stimulation of special acupuncture points on the body surface with needles, heat, or pressure has been done in China for more than 2500 years to treat diseases and relieve pain. 8,9 The traditional theory behind this therapy includes non-Western concepts such as meridians, Qi, Yin, and Yang, and other aspects of Chinese philosophy. These ideas appear to be incompatible with the modern, Western view of life. 10 Nevertheless, the West has been intrigued with acupuncture, and spectacular reports about surgery with acupuncture-induced analgesia in China have appeared in the Western press since the 1950s. 11 –13
There have been increasing numbers of clinical trials evaluating the efficacy of acupuncture and related techniques as an adjuvant method for postoperative analgesia.
The aim of the present research was to evaluate the efficacy of electro-acupuncture (EA) analgesia in septoplasty surgery by studying its influence on the level of pain at the operative site when specific acupuncture points were used.
Materials and Methods
Patient population
With the approval of our Institutional Ethics Committee and written consent, 90 patients with an American Society of Anesthesiology (ASA) physical status of I–II scheduled for elective septoplasty because of nasal septal deviation were enrolled in the study. The patients were not included if they (1) had a history of opioid abuse, or nonsteroidal anti-inflammatory drug medication; (2) were unable to understand the consent formal visual analogue scale (VAS) for pain measurement; (3) had a history of psychiatric disease; (4) revealed extreme obesity (body–mass index >40); (5) had local or systemic infection; (6) had prosthetic or damaged cardiac valves; or (7) had a positive pregnancy test for female patients.
Study design
A randomized, double-blind study was conducted, and a sealed envelope method was used for randomization. After informed consent was obtained, patients underwent screening procedures to determine eligibility for this study. Patient screening included medical history, physical examination, and vital signs. Patients in both groups received midazolam (0.03 mg/kg) intravenously, and in the control group, they received morphine (0.1 mg/kg) in a total volume of 10 mL, but in the acupuncture group, instead of morphine, patients received physiologic saline 0.9%, in a total volume of 10 mL intravenously prior to induction in the operating room. Anesthesia was induced intravenously with thiopental (4–5 mg/kg) and fentanyl (1–2 μg/kg), and atracurium (0.6 mg/kg) was used to facilitate trachea intubation.
After that in the acupuncture group, we inserted acupuncture needles (size 0.25 × 30 sterile disposable) in acupuncture points Li4 (Hegu), Li11 (Quchi), Ht7 (Shenmen), HC6 (Neiguan), as shown in Figures 1 and 2, in the dominant hand of patients. We selected these points according to previous studies and protocols of acupuncture therapy and found these points by the EA system that has a point finder, and acupuncture points were located with a probe indicating areas of decreased tissue resistance. Then these four needles were connected to the EA system (WQ-IOD1 multiple electronic acupunctoscope model, Beijing, China) and stimulation started with dense-disperse frequency (f1:10 and f2:80) and an intensity of 4 mA, for all of patients in this group. Then the hands of patients were covered by an operating room drape. We started stimulation 5 minutes prior to the start of surgery. In the control group, the wire of the EA system is pasted over the hand without needle and stimulation, and then covered by operation room drape for blindness of study. Anesthesia was maintained with isoflurane (1.20 vol%) in a 50% oxygen–N2O mixture. The surgeon did not use vasoconstrictors or local anesthetic drugs in the nose. Lung ventilation was mechanically controlled throughout the surgery. Heart rate and mean arterial pressure of patients in both groups before induction of anesthesia, after tracheal intubation and 5 minutes after surgical incision, are recorded.
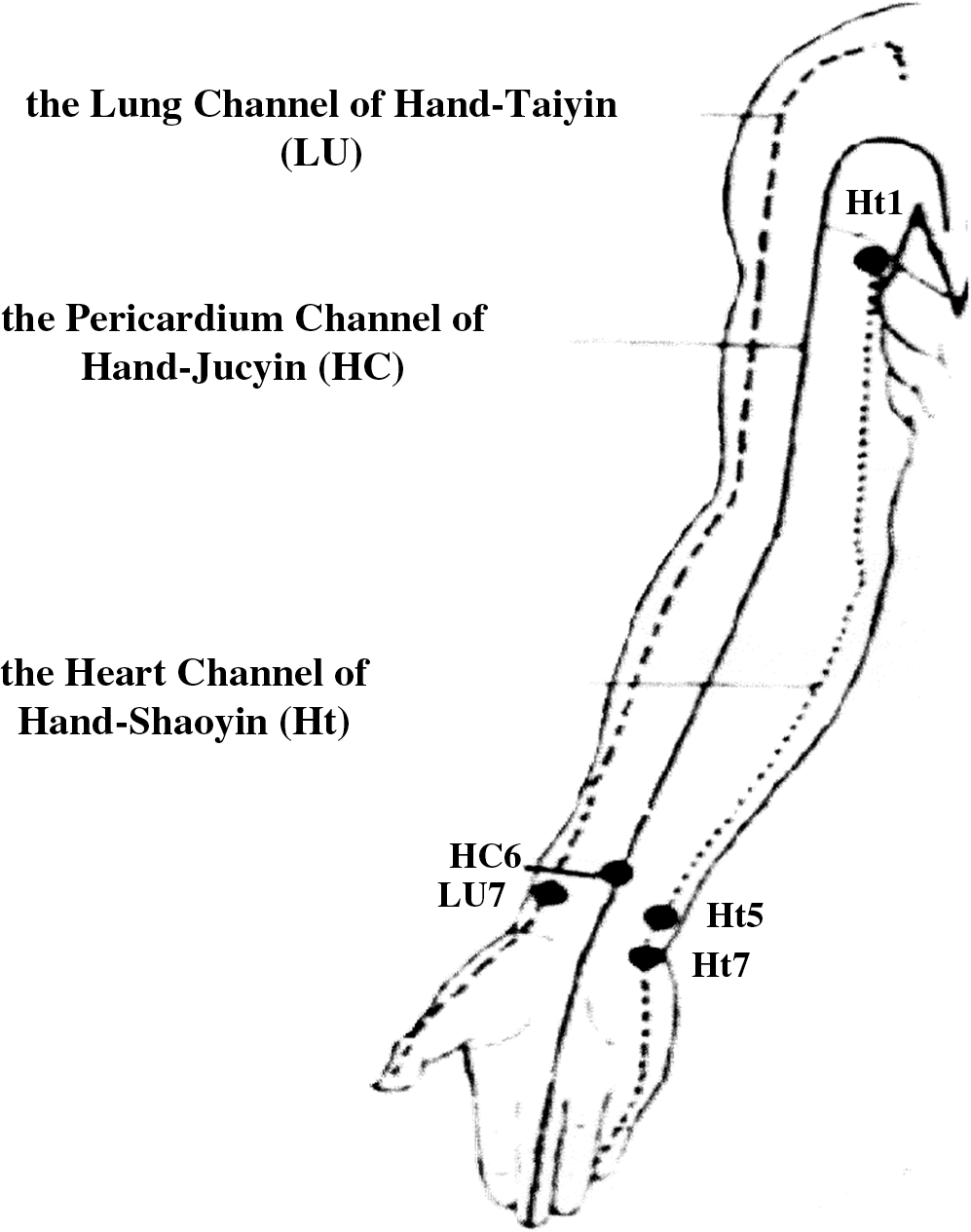
Distribution of channels and related acupuncture points (anterior view).
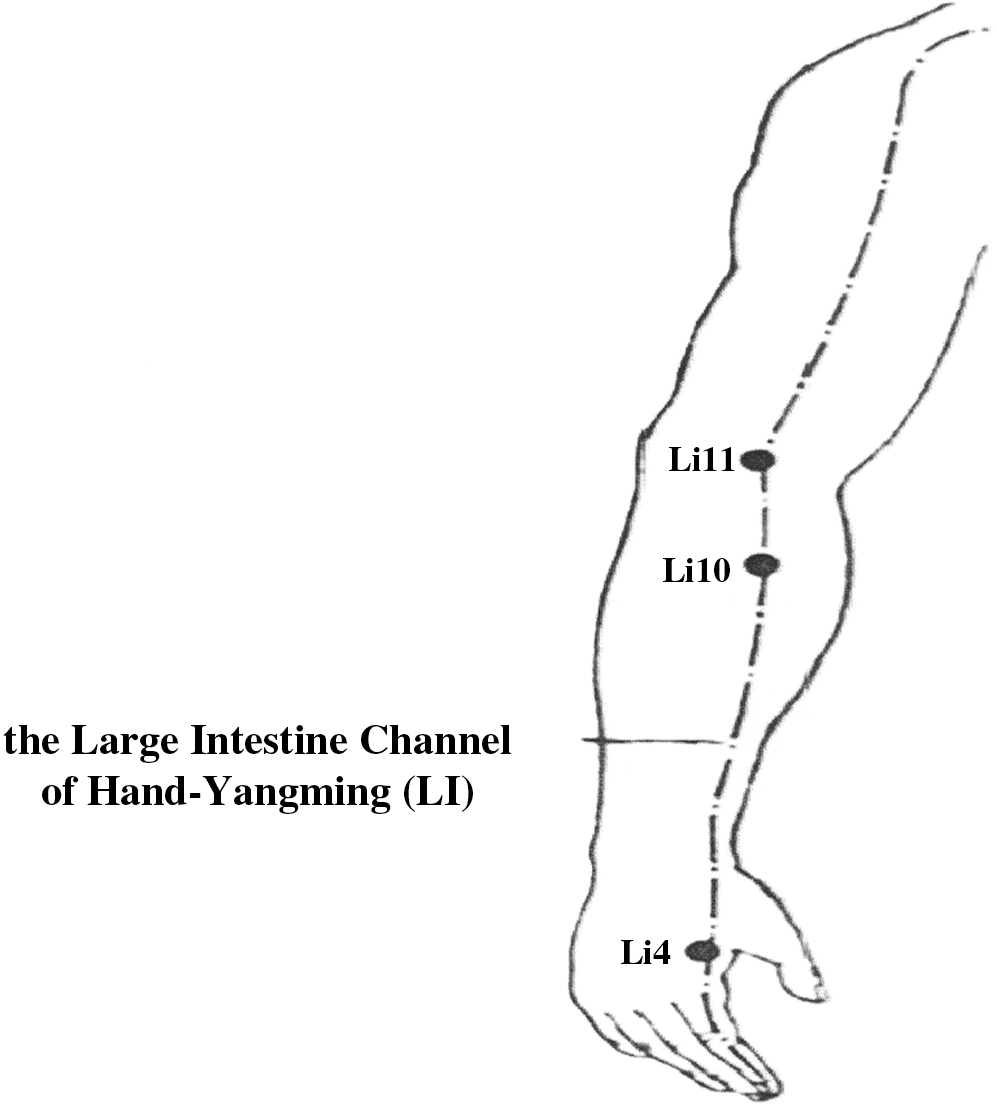
Distribution of channels and related acupuncture points (lateral view).
After the end of surgery, the patients were transferred to the postanesthesia recovery room, and pain intensity was assessed on a visual analogue scale (VAS-100, where 0, no pain; 100, worst pain imaginable). The other anesthetist who was the pain assessor did not know to which group the patients belonged. The aim of the postoperative pain relief was to keep the pain intensity reported by the patients at less than 40 mm on a 100-mm VAS up to 6 hours postoperation. If the postoperative pain of patients was ≥40 mm on a 100-mm VAS, they received 1 mg/kg meperidine as an analgesic, and the amount of postoperative meperidine was recorded. Also, in the postoperative nausea and vomiting episode, respiratory depression was recorded per hour after surgery for 6 hours. Vomiting is defined as the forceful expulsion of gastric contents from the mouth and is brought about by the powerful sustained contraction of the abdominal muscle; nausea is defined as a subjectively unpleasant sensation associated with awareness of the urge to vomit, and respiratory depression is defined as respiratory rate less than 8/min.
Statistics
The primary measure of efficacy in this study was total pain relief over the 0–6-hour time interval postacupuncture in comparison with morphine that was measured on the 100-mm VAS.
Statistical analysis was performed using SPSS 11.0 statistic package for Mac OS X version (SPSS Inc., Chicago, IL). The sample size of each group was calculated to obtain a mean difference in the immediate postoperative VAS of 30 mm with a power of 0.8. A p value <0.05 was considered significant. Normally distributed continuous data (demographics, pain intensity on VAS-100, heart rate, and blood pressure) were compared using the unpaired Student's t-test. χ2 test was used to analyze the incidence of analgesia-related side-effects.
Results
The demographic and surgical variables data were similar in the two groups, as shown in Table 1.
Analysis of total pain relief by unpaired Student's t-test indicated no significant differences between treatment groups (p = 0.69). Serial pain intensity (VAS) scores are shown in Table 2. Both the acupuncture group and the control group demonstrated the same reductions in pain intensity numerically at all time points evaluated through 6 hours postoperation (Table 2). Meperidine was not given in any patient in the two groups during the postoperative period because the VAS scores of all patients were less than 40 mm.
All values reported represent the mean ± standard deviation.
VAS, visual analogue scale.
The pulse rate fluctuation did not exceed between 5% and 10% of the initial reading throughout the surgical procedure in both groups, as shown in Figure 3 (p = 0.67).
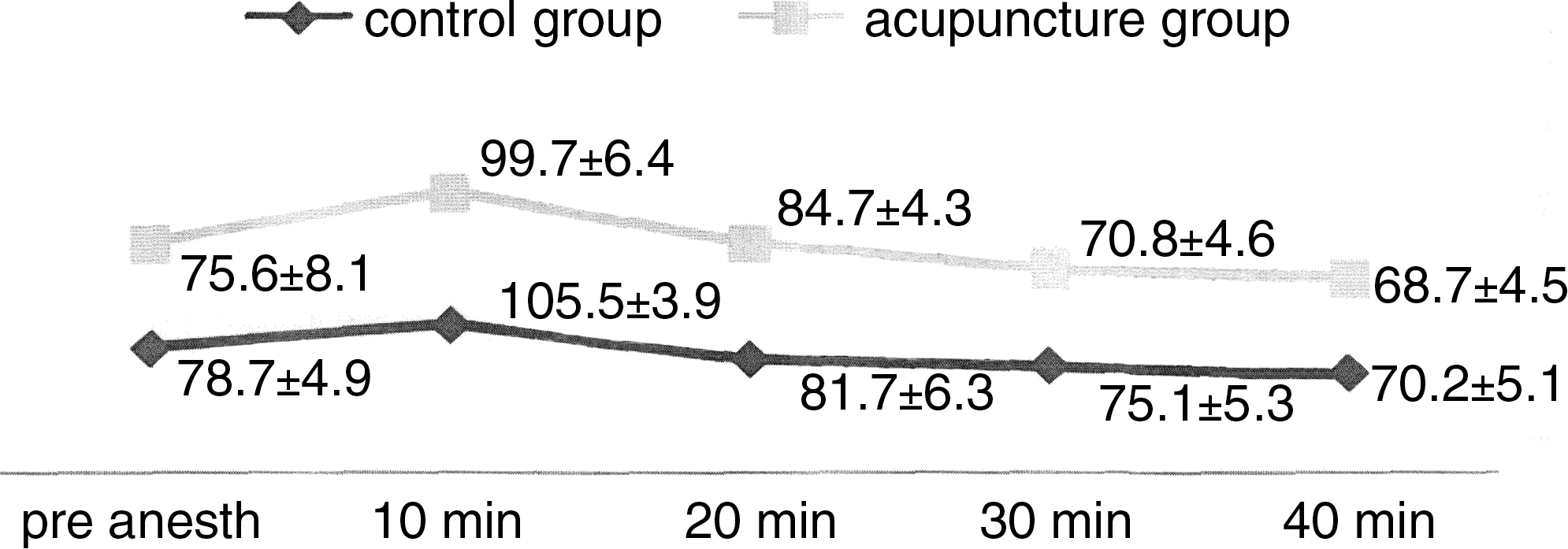
Changes in heart rate/min in both groups during surgery. (All values reported represent the mean ± standard deviation.)
The mean arterial pressure fluctuation did not exceed 10% and 20% of the initial reading throughout the surgical procedure in both groups, as shown in Figure 4 (p = 0.86).
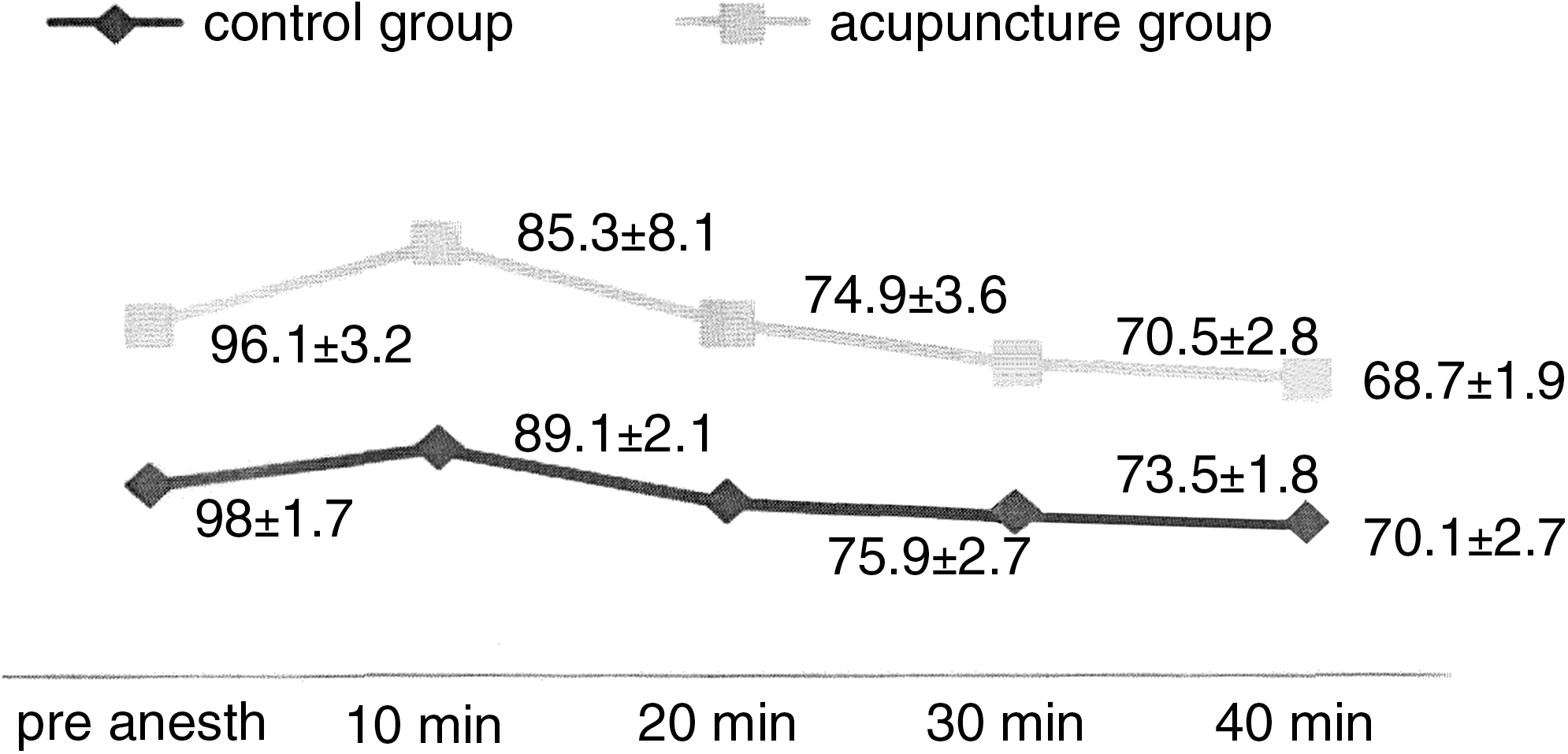
Changes in mean arterial pressure (mm Hg) in both groups during surgery. (All values reported represent the mean ± standard deviation.)
The incidence of analgesic-induced side-effects were as follows: nausea and vomiting were less in the acupuncture group than in the control group (p < 0.05) and respiratory depression was similar in both groups, as shown in Table 3 (p > 0.98).
Discussion
According to our results, perioperative EA is a suitable alternative to intravenous morphine (0.1 mg/kg) in reducing postoperative pain scores. Analgesic requirements and pain scores were not different between the groups.
Acupuncture is an important therapeutic modality in Traditional Chinese Medicine. It involves inserting fine needles into specific points. The needles are usually manipulated to elicit a characteristic sensation (de qi). 14 A well-known use of acupuncture is pain control. Several hypotheses about its mode of action have emerged in neurohormonal mechanisms involving opioids, serotonergic, and noradrenergic systems and descending noxious inhibitory control. 15,16
Findings from our study confirm the previous study of Chudakova, which showed that acupuncture analgesia can be a useful adjunct to conventional anesthesia in maxillofacial surgery. 17
In a sham-controlled randomized clinical trial, Kotani et al. applied intradermal needles to “Back Shu” acupoints in a group of patients who were scheduled to undergo major abdominal procedures. 18 These acupuncture needles were inserted 2 hours before induction of anesthesia and were retained in place for 48 hours postoperatively. The investigators found that patients in the acupuncture group reported a significant reduction in postoperative pain and analgesic requirements and postoperative nausea and vomiting compared with the sham group. 18 Christensen et al. conducted research involving 20 healthy women who underwent gynecological surgery and received either EA or no treatment (control). The intervention was administered while these women were emerging from general anesthesia. Postoperatively, the investigators found that patients who received acupuncture needed significantly less (40%) meperidine in the postanesthesia care unit when compared with the sham group. 19
In another study, preoperative treatment with low and high EA can reduce the postoperative analgesic requirements and associated side-effects in patients undergoing lower abdominal surgery. 15
Wang et al. conducted a sham-controlled randomized clinical trial evaluating the analgesic effect of postoperative EA in patients undergoing lower abdominal surgery. 20 Following a standardized anesthetic protocol, EA was applied either to acupuncture points or the para-incisional dermatomes, with the intensity of the electrical stimulation delivered at a high (9–12 mA) or low (4–5 mA) level. The investigators found that EA of these points resulted in a 30%–35% reduction in the postoperative opioid analgesic requirements. 20
As in our study, several authors have previously shown that the best effects of combined anesthesia treatment were reached when the following acupoint combinations were selected for stimulation: Yang Channel LI—the Large Intestine Channel of Hand-Yangming:Li4 (Hegu), Li10 (Shousanli), also acupoints related to the operation site technique combined with the points of Yin Channels: the Heart Channel of Hand-Shaoyin: Ht7 (Shenmen), and the Pericardium Channel:HC6 (Neiguan). 17
Location of electrode placement plays a less significant role in the analgesic effect as long as the placement of electrodes is either at an appropriate acupuncture point or at the peripheral nerves corresponding to the surgical incision. 21
In this study, we stimulated HC6 (Neiguan) during surgery, as other authors have shown that stimulation of this point reduces nausea and vomiting, 22,23 so stimulation of HC6 (Neiguan) not only helped in reducing pain but also in reducing postoperative nausea and vomiting.
Acupuncture functions by regulating the physiological state of the human body, so doctors are able to take immediate measures to avoid the physiologic disturbance caused by severe pain by adjusting the technique according to the subjective physical signs of the patient. Blood pressure and pulse rates during the operation remain stable in most cases. Postoperatively, the patient's physiologic state generally remains stable. 14,17,21
The major advantages of acupuncture analgesia are (1) safety of application for high-risk patients, (2) possible postoperative pain relief, and (3) low complication rate following surgery. 14 However, acupuncture analgesia maybe effective as an adjunctive treatment for acute postoperative analgesia if administered to surgical patients in the postoperative period. Future studies should examine whether the efficacy of EA and related forms of acupuncture is influenced by the depth of anaesthesia, types of anesthetics (i.e., intravenous versus volatile), and different states of anesthesia or types of anesthetics. 24
Limitations of the Study
However, this study was designed based on formulaic acupuncture, not individualized acupuncture. Original acupuncture textbooks state that individualized acupuncture provides better outcomes than the formulaic one. Also, it would be beneficial if in another study a group of electrical stimulation on nonacupoint tissue is designed to define that the analgesia effect of EA is acupoint specific. In our study, general anesthesia was adjusted and monitored in a classic way by using the heart rate and blood pressure. In order to avoid any influence of intraoperative factors on postoperative analgesic requirement, the monitoring of the general anesthesia in future studies should be strengthened by measuring the bispectral index. 25
Conclusions
The results suggest that both use of EA and 0.1 mg/kg IV morphine given intraoperatively resulted in a similar postoperative pain score and postoperative analgesic requirement, which meant EA had a similar analgesic effect to morphine (0.1 mg/kg) in this study.
Footnotes
Acknowledgments
The authors thank the staff and nurses of Shariati Hospital and administration staff of the Fasa Medical University for their contribution to this study and the patients who participated in this study.
Disclosure Statement
No competing financial interests exist.