
Abstract
Objectives:
Vipassana meditation (VM) is one of the most ancient and diffused types of meditative practices belonging to the pole of mindfulness. Despite the growing interest toward the neurobiological and clinical correlates of many meditative practices, no review has specifically focused on current evidence on neuro-imaging and clinical evidence about VM.
Methods:
A literature search was undertaken using MEDLINE,® ISI web of knowledge, the Cochrane database, and references of retrieved articles. Controlled and cross-sectional studies with controls published in English up to March 2009 were included.
Results:
Seven (7) mainly poor-quality studies were identified. Three (3) neuro-imaging studies suggested that VM practice could be associated with the activation of the prefrontal and the anterior cingulate cortex during meditative periods, and with increased thickness in cortical areas related to attention as well as increased subcortical gray matter in right insula and hippocampus in long-term meditators. Three (3) clinical studies in incarcerated populations suggested that VM could reduce alcohol and substance abuse but not post-traumatic stress disorder symptoms in prisoners. One (1) clinical study in healthy subjects suggested that VM could enhance more mature defenses and copying styles.
Discussion:
Current studies provided preliminary results about neurobiological and clinical changes related to VM practice. Nonetheless, few and mainly low-quality data are available especially for clinical studies and current results have to be considered with caution. Further research is needed to answer critical questions about replications, self-selection, placebo, and long-term effects of VM.
Introduction
In recent years, growing attention has been given to a particular subgroup of meditations called mindfulness meditations, in particular for their applications in the improvement of physical and mental health. 2 –6 The concept of mindfulness has its roots in Buddhism and can be firstly found in the Abhibdamma 7 and later on in the Visuddhimagga, “the path of purification,” a summary of the part of Abhibdamma that deals with meditation. 8 The core feature of mindfulness is referred to a particular kind of attention characterized by a nonjudgmental awareness of present experiences that allows the practitioner to act reflectively rather than impulsively. 9 –11 Current evidence showed that mindfulness-based interventions can enhance mindfulness levels and that increases of mindfulness levels seem to be directly related to improvements in clinical outcomes. 12 –18
While the greatest quantity of studies focused on recently developed standardized mindfulness based programs such as mindfulness-based stress reduction and mindfulness-based cognitive therapy, 2,5 in the last decade scientific studies started focusing on one of the main mindfulness meditations previously scarcely considered from a scientific point of view, Vipassana meditation (VM).
VM is supposed to be the meditation practiced by Gautama the Buddha more than 2500 years ago and is the most ancient of the Buddhist meditations. 19 A complete description of the variegate world of VM goes beyond the aim and the possibilities of the present work (for a better description see Ahir and Gunaratana 19,20 ).
In synthesis, individuals practicing VM assume the role of an observer of their thoughts and sensations. In doing so, they learn to be less judgmental. The main aim is to remain aware in the present moment. 20 VM is currently typically taught in standardized intervention of a 10-day retreat as in the tradition lead by S.N. Goenka. 21 It is usually practiced in a motionless seated position even though other postures are allowed, and can be practiced from 5 to 10 minutes twice a day for novice meditators up to several hours for expert meditators. 19,20
A growing number of VM centers are spreading all over the world 22 and, as happened for many other meditative practices, 23 –29 VM could become a tool for physically and mentally ill subjects as well as for healthy people. However, the popularity of this approach has grown in the absence of rigorous scientific evaluation. Thus, the aim of the present article is to review current evidence on the neurobiological and clinical data about VM, providing an integration between these data and suggesting new directions for future studies.
Methods
Literature research
A literature search was undertaken using MEDLINE,® ISI web of knowledge, the Cochrane database, and references of retrieved articles. The search included published articles and congress abstracts indexed in the abovementioned web-based electronic bibliographic databases, published up to March 2009. The search strategy considered only studies published in English. The search terms were the following: Vipassana, Buddhist mindfulness meditation, neuro-imaging, electroencephalography, mental disorders, physical disorders, and healthy subjects in various combinations among them.
Selection of trials
Studies and congress abstracts that focused on the relationship between VM practice and neuro-imaging or clinical outcomes in patients with mental and physical disorders as well as in healthy people were screened by 1 reviewer in order to be considered for the inclusion (Fig. 1). Included studies had to (1) be randomized controlled, controlled, or cross-sectional studies with controls; (2) include both active (i.e., treatment as usual) and inactive comparators; (3) provide quantitative data supported by statistical methodology, and (4) focus on electroencephalographic, neuro-imaging, or biological data or alternatively on clinical data in healthy subjects or in clinical samples. Reasons for exclusion were (1) qualitative reports, (2) absence of a control group, (3) statistical methodology not reported, (4) unpublished papers, and (5) reviews or meta-analysis.
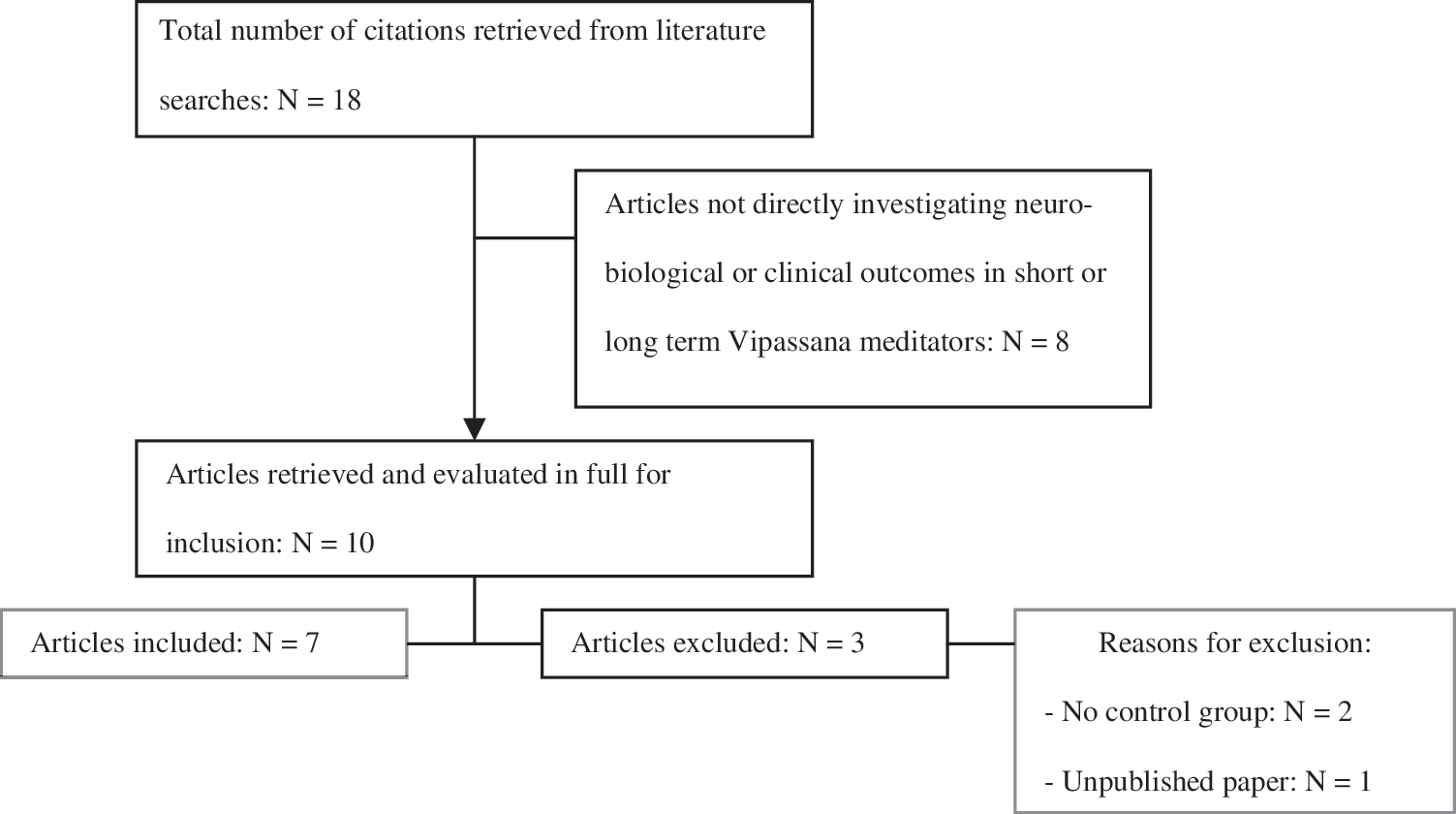
Flow diagram of the review process.
Outcome measures
The main considered outcome measures were (1) differences in cortical and subcortical thickness in Vipassana meditators and controls as measured by magnetic resonance imaging (MRI) voxel-based morphometry (trait findings), (2) differences in activation of brain areas during meditation and resting conditions in Vipassana meditators and controls as measured by functional MRI (fMRI) blood oxygen level dependence signals (state findings), (3) the reduction in alcohol and drugs consumption as measured by self-reports instruments such as the Daily Drinking Questionnaire 30 and the Daily Drug-Taking Questionnaire * in psychiatric populations of Vipassana meditators and controls, (4) the reduction of psychiatric symptoms as measured by self-reports instruments such as the Brief Symptom Inventory 31 in psychiatric populations of Vipassana meditators and controls, (5) the changes in personality measures such as the Tennessee Self-Concept Scale 32 in healthy Vipassana meditators and controls. The implications of the use of self-reports instruments for the assessment of clinical outcomes will be considered in the discussion.
Data extraction and synthesis
The data were extracted by a single reviewer using a comprehensive and pretested data extraction form (see appendix D1 and D2 in Ospina et al. 23 ). Studies were grouped together according to the type of investigated outcomes in neuro-imaging studies and clinical studies. On the basis of the investigated outcomes, neuro-imaging studies were further divided into “neuro-imaging studies focusing on short-term outcomes,” and “neuro-imaging studies focusing on long-term outcomes.” Clinical studies were further divided into “mental disorders” and “healthy subjects.” Quality of controlled studies was assessed using the Jadad Scale 33 ; quality of cross-sectional studies with controls was assessed using the Newcastle-Ottawa Scale. 34 For both measures, a score <3 was considered to be indicative of a low-quality study.
Results
Search results
The original search sought 18 articles. Eight (8) articles were excluded because their primary focus was not the investigation of neurobiological or clinical outcomes in short- or long-term Vipassana meditators. After the first screening, 10 articles remained. After the inclusion and the exclusion criteria were applied, seven studies were included in the present review (Fig. 1). Included studies comprised three crossover 35 –37 and four nonrandomized controlled studies. 38 –41 Studies excluded after the initial screening and reasons for their exclusion are showed in Table 1. A summary of included studies is shown in Table 2.
fMRI, functional magnetic resonance imaging.
VM, Vipassana meditation; PTSD, post-traumatic stress disorders; TAU, treatment as usual; NOS, New Castle Ottawa Scale.
Characteristics of included studies
A first split in the result section was performed between “neuro-imaging studies” (three studies 35 –37 ), and “clinical studies” (four studies 38 –41 ). On the bases of the investigated outcomes, the first group of studies was further divided into “neuro-imaging studies focusing on short-term outcomes 36 ” and “neuro-imaging studies focusing on long-term outcomes. 35,37 ” Clinical studies were further divided into “psychiatric disorders” (two studies on alcohol and substance abusers, 38,30 one study focusing on post-traumatic stress disorder [PTSD] symptoms 41 ) and “healthy subjects” (one study 41 ). Four (4) studies compared meditation to an inactive control: of these, three studies compared long-term meditators to nonmeditators 35 –37 ; one study compared subjects who attended a VM 10-day retreat to matched controls 41 ; three studies compared meditators who attended a 10-day VM retreat to an active comparator (i.e., treatment as usual 38 –40 ). Because of the scarcity of data, the difference in investigated outcomes, and the difference in study designs, data were reported in narrative form.
Neuro-imaging data about VM
Neuro-imaging studies focusing on short-term outcomes
A single study compared 15 expert Vipassana meditators to 15 nonmeditators, matched for sex, age, education, and handedness, investigating both mindfulness of breathing and of mental arithmetic conditions. 36 The decision to investigate only expert meditators was motivated by their greater ability to maintain focused attention when compared to novice meditators who periodically enter into a state of “daydreaming” characterized by self-generated distracted mental activity. In the meditation condition but not during the arithmetic condition, the activation in the rostral anterior cingulated cortex (ACC) and the dorsal medial prefrontal cortex (mPFC) in both hemispheres was stronger in meditators compared to controls. The authors suggested that greater rostral ACC activation in meditators could reflect stronger processing of distracting events and that meditators were more successful in attention regulation. ACC, in fact, has often been suggested to play an important role in self-control and in cognitive control with the role of detecting conflict between simultaneously active, competing representations and of engaging the dorsolateral PFC to resolve such conflict. Furthermore, the authors suggested that the increased activation in the dorsal medial PFC could reflect the fact that meditators were more engaged in emotional processing. PFC represents the neural basis of higher cognitive functions such as self-reflective consciousness and identification of emotions, and its greater activation was suggested to be related to a higher integration of these complex functions in Vipassana meditators.
Neuro-imaging studies focusing on long-term outcomes
A first study investigating whether a long practice of VM could provide long-term modifications of brain structures 35 found in a sample of 35 subjects (20 long-term Vipassana meditators compared to 15 matched controls) that in Vipassana meditators brain regions associated with attention, interoception, and sensory processing were thicker than in matched controls, whereas no difference was found in other areas. Furthermore, this effect was correlated with meditation experience. Thicker areas included the PFC, in particular superior frontal sulci and right anterior insula. The differences in prefrontal cortical thickness were greater in older participants and the authors suggested that meditation, especially if long practiced, might offset age-related cortical thinning and enhance cortical thickness. Interestingly, the authors noted that these results are in accord with previous findings suggesting that, when a task that requires attention is consistently directed toward a behaviorally relevant sensory stimulus, robust changes in sensory cortical maps are observed. Unfortunately, however, the cross-sectional design of this study did not allow detection of possible confounding factors such as, for example, a possible initial greater cortical thickness in those who desired to meditate.
A second study 37 investigated whether gray matter concentration in regions that are typically activated during meditation was greater than in matched nonmeditator controls. The authors noted that the method of cortical thickness analysis employed by Lazar et al. 35 bears the disadvantage that changes in subcortical structures cannot be detected, and the authors wanted to extend previous findings. Their results showed that gray matter concentration was significantly greater for meditators in the right hippocampus and the right anterior insula and showed a trend toward significance in the left inferior temporal gyrus. The authors noted that the right anterior insula is involved in interoception and visceral awareness and that this difference in meditators from controls presumably reflects the specific training during VM, namely, the awareness of bodily sensations. Moreover, they emphasized the importance of their findings on hippocampus because of its involvement in modulating cortical arousal and responsiveness. Eventually, meditators' mean gray matter concentration within the relevant regions in the left inferior temporal gyrus was predictable by the amount of meditation training, corroborating the assumption of a causal impact of meditation training on gray matter concentration. However, the expected differences at the dorsolateral PFC, ACC, and left postcentral gyrus were not confirmed, thus underlying the necessity for further investigations in larger samples.
Clinical studies
Psychiatric disorders
Note, however, that adherence to mindfulness practice was not assessed during or following the course, so it is not possible to assess whether participants understood and correctly practiced the techniques, and therefore it is not clear whether the effects of course participation were due to mindfulness training or other course characteristics. Also, it is worth mentioning that the two questionnaires used to investigate alcohol and drugs abuse 30 * assess quantity and frequency of alcohol and drug use for both a typical week and the peak week in the past 90 days (in the case of the present investigation in the 90 days prior to incarceration). As a consequence, it is not possible to rule out that the reduction in alcohol and drug consumption could simply be related to the higher impossibility/difficulty of getting alcohol and drugs in prison, at least for patients who were still inside the prison at the time of the follow-up. A further shortcoming of included studies was that the average incarceration time at baseline was not reported.
Unfortunately, many limitations affect these findings: the two major limits concern the findings based on an incarcerated population, which limit the generalizability to substance or alcohol abusers in the general population, and the absence of randomization, which could result in selection bias of participants.
Healthy subjects
The only clinical study in healthy subjects comparing two cohorts that exceeded 200 participants each attending a 7-day VM retreat to a nontreated control group found positive gains in all areas of self-representation in meditators compared to controls, 41 as measured by the Tennessee Self-Concept Scale. 32 Moreover, meditators developed more mature defense and coping strategies characterized by greater maturity and tolerance of common stressors, and increases in Buddhist beliefs were found to be significantly correlated to heightened self-esteem and less impulsiveness. These findings could reflect, according to the authors, that Buddhist philosophy of the “middle way” would enhance an increased and more reflexive and mature awareness. Unfortunately, the absence of randomization and of follow-up measures could have introduced a self-selection bias and interfered with understanding to what extent the improvements obtained in the short term could be maintained in the long term.
Discussion
The aim of the present study was to review current evidence on the neurobiological and clinical data about VM. A single fMRI study suggested that, during the practice of VM, an increased activity in the PFC and in the ACC can be observed in expert meditators compared to controls. This finding is in accordance with observations in other types of meditations, suggesting that all voluntary meditative practices associated with sustained attention activate frontal structures engaged in attentional processes and that this effect could be particularly prominent in expert meditators, possibly because of their higher ability to maintain a sustained attention without distractions. 48,49 Further studies focusing on long-term effects of VM observed in expert meditators compared to controls indicated structural modifications of specific brain areas as well; specifically, they found in meditators increased cortical thickness, suggesting a protective effect of VM from age-related cortical thinning; they also found increased gray matter concentration in the right hippocampus and the right anterior insula—areas involved in the modulation of cortical arousal and responsiveness and in interoception and visceral awareness, respectively. Interestingly, these results are in accord with previous findings suggesting that, when a task that requires attention is consistently directed towards a behaviorally relevant sensory stimulus, robust changes in sensory cortical maps are observed. 50 –52 Thus, it could be suggested that repeated activation of specific brain areas could lead to long-lasting brain structure changes. 35,37 Consonant with such a hypothesis, structural MRI studies found a partial overlap between thicker areas in meditators 35,37 and areas activated during meditation in the early functional study by Holzel and colleagues. 36 Notably, results in Vipassana meditators are in line with findings in long-term Zen meditation, a further mindfulness meditation, showing that, while control subjects displayed the expected negative correlation of both gray matter volume and attentional performance with age, meditators did not show a significant correlation of either measures with age. 53 The authors proposed that Zen meditation could have a protective effect from physiologic cognitive decline and could be useful for illness implying an attention deficit such as, for example, attention deficit disorders.
A first interesting area of research could be trying to correlate these findings with the development of a more reflexive rather than automatic reactive awareness, as suggested by mindfulness theories, through studies focusing on the same sample both from a clinical and from a neuro-imaging point of view. A second area of investigation could be studying prospectively brain areas in novel Vipassana meditators and matched controls in order to control for possible baseline confounding factors not detectable by the cross-sectional design of actual studies.
To our knowledge, no specific electroencephalographic (EEG) study specifically investigated a possible relationship with VM practice. On the other hand, some EEG studies are currently available about other types of active meditations, usually in the direction of an increase in α and θ activities, the last one correlated with experience, associated with different degree of self-induced concentration and relaxation, 49 and further EEG studies could be useful to investigate the EEG patterns in novice and long-term Vipassana meditators.
From a clinical point of view, VM was found to be related to a significant reduction of substances and alcohol abuse, suggesting an enhancement of more adaptive copying strategies in prisoners' samples, and could have a role in the enhancement of more mature defenses in healthy people as well. Note, however, that the instruments used for the assessment of clinical outcomes were all self-reports, and this could raise concerns about the reliability of reported findings. Such concerns could be partially reduced by the fact that, at least in some studies, 38,39 participants were assured that responses would be kept confidential, thereby increasing reliability and validity of self-report data. 54,55 Nevertheless, future studies could be improved by the use of more rigorous external assessments as well as of specific scales that assess the possibility of a social desirability bias such as the Marlowe-Crowne Social Desiderability Scale, 56 a strategy already used in previous works about other types of mindfulness meditations. 57
Further limitations, such as the inclusion of only incarcerated subjects and the absence of randomization, suggest considering current evidence with caution and do not yet allow generalization of the present findings to other populations of patients. Note, however, that adherence to mindfulness practice was not assessed during or following the course, so it is not possible to assess whether participants understood and correctly practiced the techniques, and it is therefore not clear whether the effects of course participation were due to mindfulness training or other undetected features.
It is noteworthy that the average incarceration time was not reported. As a consequence, the pre-test alcohol and drugs consumption was based on memory of events, which may reduce the validity of the pre-test measures. In any case, the fact that subjects reported less alcohol consumption at post-test than they recalled from before they went to prison is encouraging, and further research with more objective behavioral measures is needed.
Interestingly, other meditative practices, in particular transcendental meditation, already showed efficacy for the treatment of addiction disorders 27,58,59 and for prisoners' rehabilitation, 60 and further better-designed randomized controlled trials could compare VM, transcendental meditation, and TAU for the treatment of addictive disorders so as to extend available evidence as well as to investigate possible predictors of response to different meditation strategies. Additionally, it could be useful to compare a VM retreat to scholarly courses about VM that were comparable to the retreat in terms of group and teaching support but did not include the active component of VM and to study the effect of VM retreats in the long term in order to exclude possible nonspecific placebo effects.
It is noteworthy that an important problem in the overall interpretation of findings about VM is the absence of a validated scientific model of this practice. Such an issue is particularly concerning, especially considering that there is not yet general agreement about the broader class of meditative practices in which VM is currently classified, mindfulness meditations. Kabat-Zinn, for instance, proposed that mindfulness should be considered as ‘‘the awareness that emerges through paying attention on purpose, in the present moment and non-judgmentally.” 61 While comparable definitions of mindfulness abound, research uncovering the etiological basis of mindfulness is equivocal. Langer proposed that the construct of mindfulness consisted of five components: openness to novelty, alertness to distinction, sensitivity to differing contexts, implicit awareness of multiple perspectives, and an orientation to the present 62 and related such components to personality traits. Others have argued that mindfulness is a cognitive ability 63 or a cognitive style, 64 hence suggesting that mindfulness is a skill that one can learn. Psychometric evaluations of mindfulness also abound and suggest alternatively that it should be considered as a single construct characterized by a receptive attention to and awareness of present events and experience 65,66,† or as a multifaceted construct characterized by at least five independent facets, namely, nonreactivity, observing, acting with awareness, describing, and nonjudging. 15,67 Further disagreement exists also between those who consider mindfulness as a state-like quality that is maintained only when attention to experience is intentionally cultivated with an open, nonjudgmental orientation to experience 9 and those who suggest that it should be better considered as a trait-like quality. 15,65
A further problem is represented by the scarcity of proposed mechanisms of action through which VM could improve health. In particular, the only attempt to correlate VM practice to the reduction of alcohol and substance consumption suggested that this clinical outcome was mediated by thought acceptance. 39 Recently, however, many hypotheses including both psychologic and biological mechanisms have been proposed to explain how further meditations including mindfulness meditations improve health. The first hypotheses comprise, for instance, paying attention in a particular way, paying attention in the present moment, and paying attention nonjudgmentally, all factors that could contribute to re-perceive reality in a more flexible and adaptive way through a reduction of ruminative and dichotomous thinking. 68 Increases of acceptance, nonjudging, and acting with awareness have been consistently reported to increase with increases of overall mindfulness levels and to mediate clinical outcomes as well. 15,67,69 On the other hand, proposed biological mechanisms comprise the activation of cerebral areas related to positive emotions, 70 reduction in cortisol levels, 48 the release of β-endorphins, 48 and an enhancement of parasympathetic activity. 71 Thus, future research should better investigate the neurobiological correlates of VM in order to confirm and/or extend these findings to VM practice as well.
It is noteworthy that many limitations affect the present review. A first limitation is represented by the decision to limit the research to articles published in English, so that a number of Eastern journals that could contain further results about VM practices have not been indexed. A second limitation is characterized by the literature review process that was conducted by a single author, thus introducing a potential selection bias. Finally, a further limitation is the inclusion of different study designs that could bias our findings; for example, not considering possible confounding factors due to the absence of randomization in the controlled study or not allowing inference of causality in cross-sectional studies that are carried out at one time point and give no indication of the sequence of events. Future studies should replicate present findings, investigate larger samples, introduce randomization and at least single blinding (a methodology where an external evaluator, but not the practitioner, is blind to treatment), and investigate use of VM for further disorders.
In conclusion, long-term VM practice seems to be related to both state and trait brain modifications, and preliminary evidence suggests a possible role for the management of alcohol and substance dependences as well as for healthy people. Nevertheless, more research through better-designed randomized controlled studies is needed to confirm present findings and explore further directions.
Footnotes
Disclosure Statement
No competing financial interests exist.
*
Parks GA. The Daily Drug-Taking Questionnaire (DDTQ) version 1: A measure of typical and peak drug use. Unpublished manuscript, 2001.
†
Feldman GC, Hayes AM, Kumar SM, et al. Development, factors structure and initial validation of the Cognitive and Affective Mindfulness Scale. Unpublished manuscript, 2004.