
Abstract
Introduction:
Traditional Chinese Medicine (TCM), a modern interpretation of Chinese medicine, developed in the 1950s. It differentiates biomedical diseases into patterns. Each pattern comprises symptom/signs that have their own unique treatment protocol. Most TCM research has used fixed formula treatments for Western-defined diseases with outcomes often measured using objective biomedical markers. More recently, a number of trials have attempted to accommodate TCM clinical practice within the framework of rigorous evidence-based medical research. The aim of this article is to describe a novel outcome measure based on TCM patterns that was used in a pilot study for people with hepatitis C virus (HCV).
Methods:
Sixteen (16) participants with HCV were enrolled in a randomized, controlled pilot study and allocated to a treatment or control group. TCM pattern diagnosis was obtained at baseline and used to guide acupuncture treatment for the treatment group. Each individual's primary, secondary, and tertiary TCM patterns were identified, which involved the systematic evaluation of the participant's information against the TCM patterns and conversion of the pattern to a percentage. Baseline and postintervention percentages for the three TCM patterns for the two groups were compared to assess change.
Results:
There was a significant mean percentage decrease in pattern expression at week 12 compared to baseline for the secondary and tertiary patterns of the treatment group (56.3% versus 47.5%; p = 0.045 and 48.1% versus 33.6%; p = 0.037, respectively). No significant change was found for the primary, secondary, or tertiary patterns for the control group or for the primary pattern associated with the treatment group.
Conclusions:
The quantification of TCM patterns in this study permitted statistical evaluation of TCM pattern change. Previously, TCM pattern identification had only been used as a basis for developing the treatment protocol in clinical trials. This is the first time it has been employed as a novel outcome measure.
Introduction
In an attempt to align research design with clinical practice, several studies have used TCM pattern identification to guide both acupuncture and herbal treatment within the constraints of a clinical trial. 3 –5 This method was developed and first documented by Schnyer in 1998, in a study in which participants who were initially recruited according to a biomedical diagnosis were then further diagnosed according to the TCM pattern. 6 Schnyer termed this approach “manualization,” whereby each TCM pattern for the condition of depression was linked to a defined treatment protocol, with each participant receiving acupuncture at a set of acupoints, dependent on their TCM pattern. It was suggested that this would improve the external validity of the trial with the treatment designed to align with clinical practice, thereby providing individualization of treatment and a reproducible and standardized protocol. The process of manualization and its use in acupuncture clinical trials has been described by many authors. 7 –12
This article reports on a novel extension of Schnyer's work in a randomized, single-blind (participants), controlled pilot study using acupuncture on people with hepatitis C virus (HCV). TCM pattern differentiation was used not only to guide acupuncture treatment but also as an outcome measure. The design of the study as well as the results of the effect of acupuncture on the primary outcome disease measures (alanine aminotransferase levels and RNA viral load) and secondary outcome measure Hepatitis Quality of Life Questionnaire (HQLQ) are not reported in this article and will be the basis of a future article. This article reports on the development of a novel outcome measure used to evaluate TCM treatment within the constraints of a clinical trial.
Methods
Manualization of HCV disease using TCM patterns
To identify the various TCM patterns and associated acupoint treatments for HCV, a search was undertaken to identify HCV published literature including clinical trials, cohort studies, journals, textbooks, and conference abstracts. Searches were conducted using electronic databases: Alternative and Allied Medicine Database (AMED), Cumulative Index to Nursing and Allied Health (CINAHL), Cochrane multifile EBM reviews, MEDLINE,® and PubMed (last searched July 14, 2008). Terms used for the search were acupuncture, Chinese herbal/ or medicine, and Traditional Chinese Medicine with hepatitis or hepatitis C. A total of 235 references were generated. Only one study reported the use of TCM patterns as a basis for treatment. 13
A hand search of journals and textbooks kept at the University of Technology, Sydney library, however, revealed one acupuncture case study 14 and five English language sources that identified TCM patterns associated with hepatitis. 15 –19 These seven sources reported in total 38 TCM patterns associated with hepatitis. 13 –19 Analysis of the 38 TCM patterns revealed some similarity in both name and symptom cluster, which led to the 38 TCM patterns being collapsed to 17 (Table 1). The second edition of A Practical Dictionary of Chinese Medicine 20 was used to reference and standardize the TCM patterns.
Please note where appropriate the pattern names were aligned with Wiseman and Feng. 20
An example of symptom/signs of one TCM pattern associated with hepatitis, Liver Yin Vacuity, are: slight rib/side flank pain, dizziness, irritability/quick temper, fatigue, warm palms and soles of feet, low fever, dryness of eyes/nails/throat and mouth, blurry vision, muscle spasms, reddish cheeks and eyes, and numb limbs.
Similarly, symptom/signs were identified and collated for the remaining 16 TCM patterns. Several sources were then reviewed for acupuncture treatment protocols for the 17 TCM patterns. 14,17,21,22 An example of one acupuncture treatment protocol for the TCM pattern Liver Yin Vacuity is given in Table 2.
Individuals with confirmed HCV who were aged 18–70 years were considered eligible for the study. Participants were recruited through local advertising, HCV health workers, and support groups. In total, 130 people expressed an interest in entering the trial. After the initial telephone inquiry that assessed eligibility, potential participants were asked to schedule an interview. Inclusion criteria were confirmed: HCV RNA (polymerase chain reaction) viral detection test; and an elevated alanine aminotransferase (ALT) level (≥ 57 and ≤ 350 U/L) within 6 months of enrollment. Participants with other forms of liver disease, recently (within the last 3 months prior to screening), currently, or about to undertake antiviral treatment, or current alcohol consumption greater than two standard drinks daily (42 g [1.5 oz], 80 proof; 336 g [12 oz], 5% beer; or 150 g [5 oz], 12%–17% wine) were excluded. Following verification of eligibility, written consent was either obtained at the time of interview or the participant posted the consent form to the researcher. Sixteen (16) eligible participants consented over a recruitment period of 19 months. As successful applicants were received, the eligible participants were put into a block of 4 and then randomly allocated to either of one of two interventions (two to the treatment group and two to the control group) using a random-number generator.
Two (2) consecutive treatments for each TCM pattern were developed. Because multiple TCM patterns were identified for an individual, each primary, secondary, and tertiary TCM pattern was treated successively over 3 weeks and then repeated three times. Therefore, each participant in the treatment group received six different treatments four times (first and second treatment for each of three TCM patterns were repeated three times, totaling 24 acupuncture treatments). This process is representative of the procedure that occurs in day-to-day acupuncture practice closely replicating the diagnostic and treatment process that a TCM practitioner undertakes with each patient.
The control intervention involved a “sham” style acupuncture (shallow insertion with no needle manipulation at nonacupoint sites) at designated sites across the body and on the ear. Two (2) sham-style acupuncture interventions were repeated each week over the 12-week period.
A TCM pattern history form that included all the symptoms derived from all the 17 TCM patterns associated with hepatitis was used to collect data by the researcher (C.A.B.). This was undertaken at enrollment and 12 weeks later at completion of the intervention phase.
Participant pattern differentiation and quantification
First, a list of the participant's symptom/signs was generated from the developed questionnaire, which was systematically evaluated against the TCM patterns (symptom clusters) to ascertain the number of symptoms within each diagnostic pattern. Table 3 shows an example of a trial participant's response to two patterns of the Diagnostic Pattern Questionnaire.
Filled squares indicate that the symptom was present.
Once the participant's symptom/signs were tabulated, the total symptom frequency score for each TCM pattern was then transformed to a percentage using the following formula:
For example, the Liver Yin Vacuity pattern (Table 3) shows that 6 of the 11 symptom/signs were expressed (6/11), which transforms to 55%, while the other example, binding depression of Liver Qi pattern symptom expression (3/9), transforms to 33%. (For the full listing of symptom/signs associated with the diagnostic patterns, please contact the main author.)
Figure 1 shows an example for the same participant, listing both raw and the transformed percentage scores for all TCM patterns expressed by this individual. Thirteen (13) TCM patterns of the 17 patterns represented organ-specific patterns, whereas 4 TCM patterns (Qi Vacuity, Yin Vacuity, Blood Vacuity, and Blood Stagnation) represent general dysfunction patterns. Because of the general representative nature of these patterns and the inability to specifically direct a treatment and selection of acupoints, these last four patterns were not incorporated into the treatment protocol and are not shown in the analysis figure (Fig. 1).
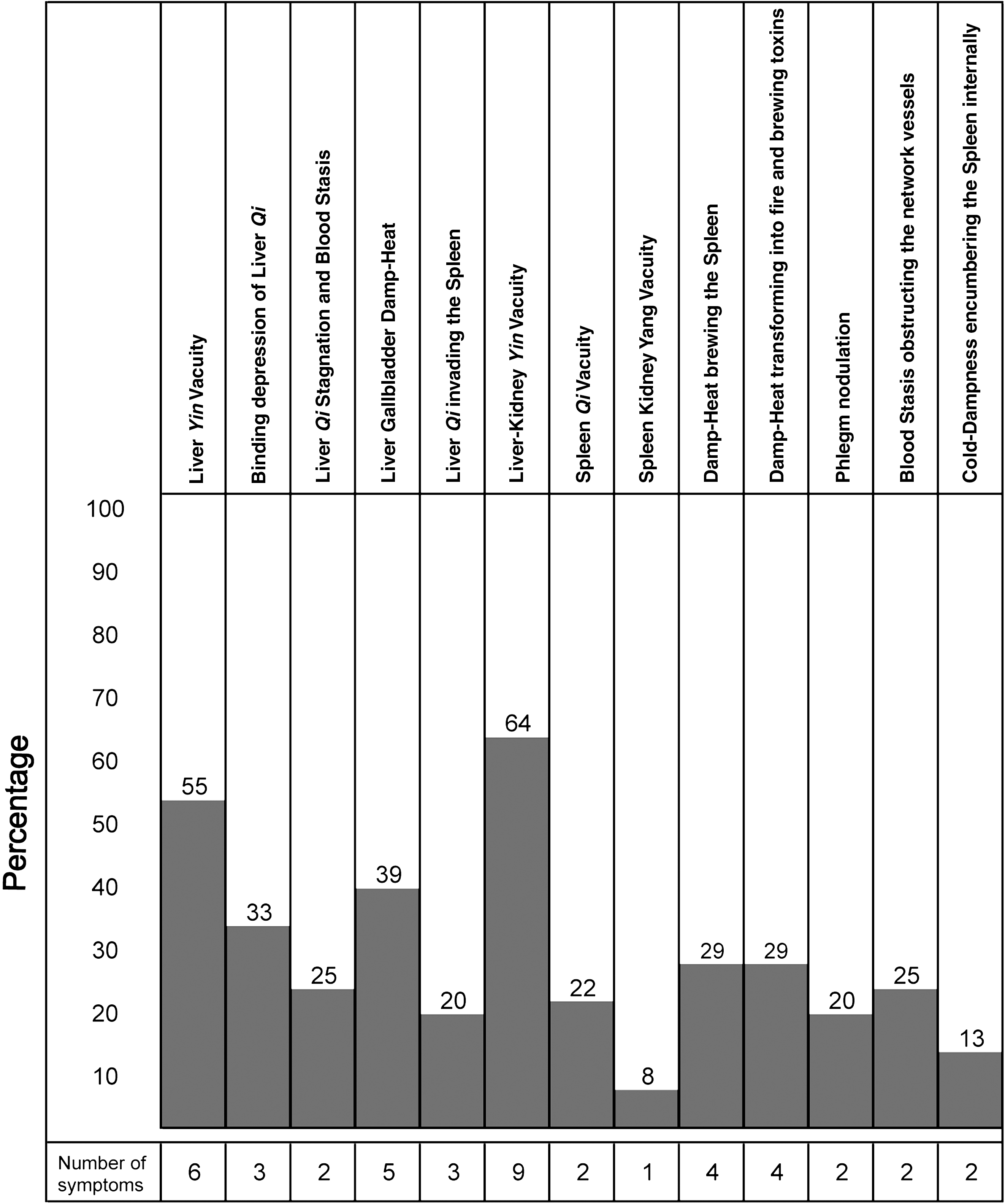
Example of a Traditional Chinese Medicine pattern expression for an individual at baseline.
As Figure 1 shows, the primary TCM pattern for this individual was Liver-Kidney Yin Vacuity (64%), secondary pattern was Liver Yin Vacuity (55%), and the tertiary pattern was Liver Gallbladder Damp-Heat (39%).
TCM pattern reassessment
By systematically identifying the symptom/sign expression within each TCM pattern both pre- and postintervention, a unique TCM outcome measure was developed. This measure allows statistical analysis of any change in expression of a TCM pattern over a course of treatment. Figure 2 shows pre- and post-treatment TCM pattern changes for the previous example.
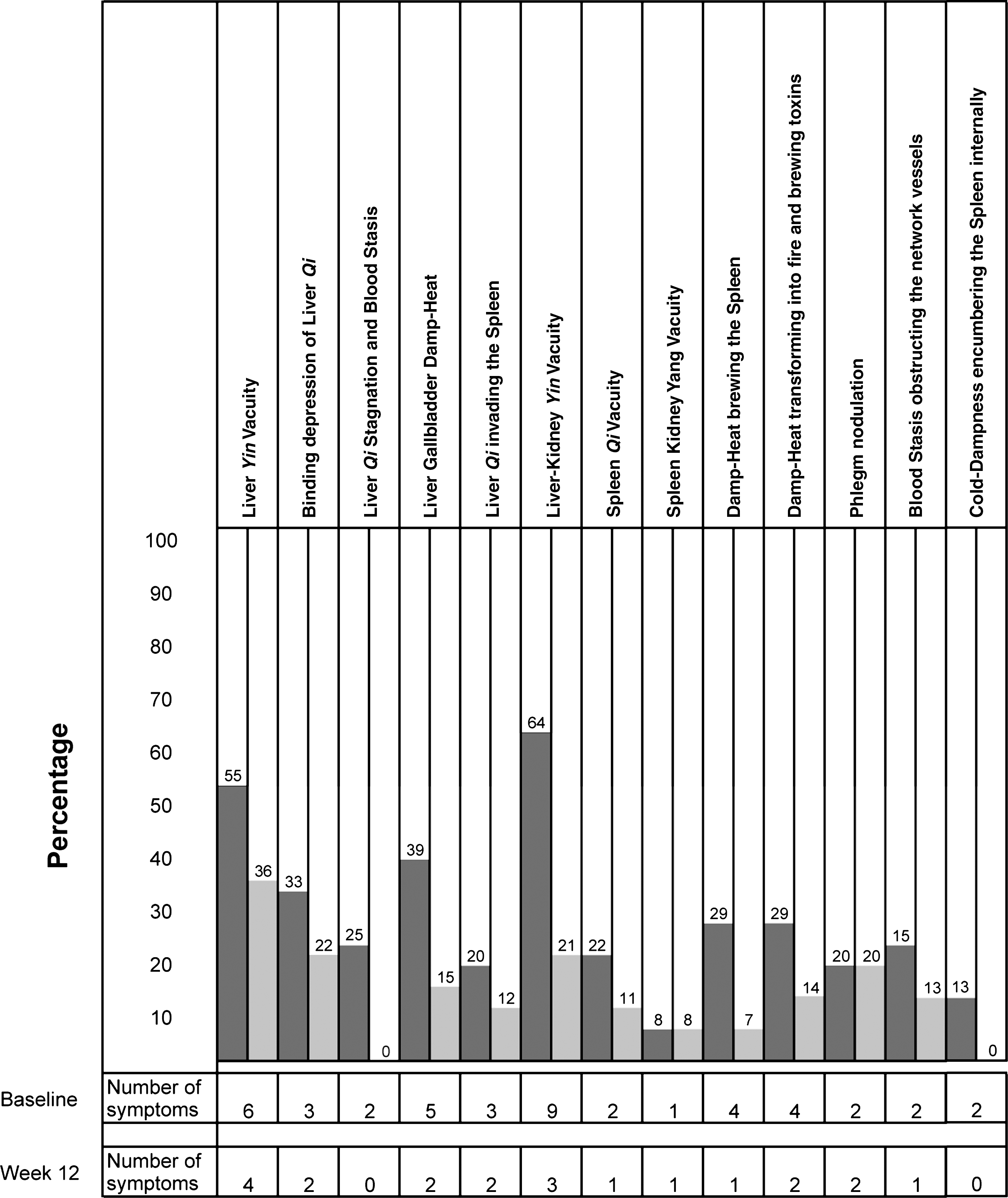
Traditional Chinese Medicine pattern expression for an individual, baseline and at completion of the treatment (week 12).
Statistical Analysis
Data analysis was conducted after all the participants completed the study. Data were tabulated and transferred into an appropriate statistical package (Minitab version 14). For baseline comparison of the patterns between the control and treatment group, a two-sample t test was used. For comparison between baseline and postintervention pattern scores for each group, a paired t test was used for the secondary and tertiary patterns, while an analysis of covariance (general linear model) was used for the primary pattern to take account of the differences in baseline scores between the treatment and control groups. A p value < 0.05 was considered significant.
Results
The results focus on the symptom expression associated with TCM pattern differentiation rather than the primary (ALT) and secondary HQLQ outcome measures, which did not change significantly from baseline.
Results are presented for: baseline TCM pattern expression by all participants (treatment and control groups) primary, secondary, and tertiary TCM pattern scores at baseline comparison between the treatment and control group for the primary, secondary, and tertiary TCM pattern scores at baseline and on completion of the intervention phase.
Baseline TCM pattern expression by all participants (treatment and control groups)
Table 4 shows the TCM patterns expressed by all participants at baseline (week 0). Eight (8) participants expressed all specific organ patterns and no participant expressed all four general dysfunction patterns (Qi Vacuity, Yin Vacuity, Blood Vacuity, and Blood Stagnation). The most commonly expressed pattern was Liver Yin Vacuity, which was the primary pattern for 8 participants. Of the 17 TCM patterns, 6 TCM patterns were expressed by all 16 participants (Liver Yin Vacuity, Liver Kidney Yin Vacuity, binding depression of Liver Qi, Liver Qi invading Spleen, phlegm nodulation, and Cold Dampness encumbering the Spleen internally). Only 1 participant expressed Blood Vacuity symptoms, and Blood Stagnation was not expressed by any participant.
Each participant is represented by their ID number.
TCM patterns at baseline
Four patterns emerged as the primary TCM pattern expressed by the trial participants (n = 16) at baseline. Table 5 shows that Liver Yin Vacuity was expressed as the primary pattern by 8 participants with a mean percentage expression of 62.5%, followed by binding depression of Liver Qi, which was expressed by 4 participants with a mean percentage expression of 55.6%, 2 participants expressed Liver–Kidney Yin Vacuity (mean 46.5%), and another 2 participants expressed phlegm nodulation as their primary pattern (mean 45%).
Six (6) patterns were identified as the secondary TCM pattern expression by the trial participants (n = 16) at baseline. Liver–Kidney Yin Vacuity was expressed by 5 participants as their secondary pattern with a mean percentage expression of 58.6%, followed by binding depression of Liver Qi expressed by 4 participants with a mean percentage expression of 50%, 3 participants expressed Liver Yin Vacuity (mean 42.4%), 2 participants Damp Heat brewing the Spleen (42.9%), and 1 participant each expressed Liver Qi invading the Spleen (33.3%) or phlegm nodulation as their secondary pattern (mean 30%).
In total, seven patterns were expressed as the tertiary patterns by participants (n = 16). Two (2) participants (9 and 11) expressed two patterns with equal weighting (Liver–Kidney Yin Vacuity and Damp Heat brewing the Spleen). The pattern of Damp Heat brewing the Spleen was expressed by 7 participants (mean percentage expression 40.8%), with Liver–Kidney Yin Vacuity expressed by 5 participants (mean 40.0%). Binding depression of Liver Qi was expressed by 2 participants (mean 50.0%). The patterns Liver Yin Vacuity, Liver Gallbladder Damp Heat, and Liver Qi invading the Spleen, Damp Heat transforming into fire and brewing toxins were each expressed by only 1 participant (54.5%, 38.5%, 26.7%, and 21.4%, respectively) (Table 5).
Comparison of the TCM pattern expression for primary, secondary, and tertiary patterns at baseline between treatment and control groups
At baseline, the treatment group showed a significantly higher percentage expression for the primary TCM patterns compared to the control group (66.3 versus 50.6; p = 0.03). No difference in pattern expression was found between the treatment and control groups for the secondary or tertiary patterns at baseline (p = 0.13) (Table 6).
p-values are shown in bold where significant.
SD, standard deviation.
Comparison of the primary, secondary, and tertiary TCM patterns at baseline and on completion of treatment
Table 6 shows the TCM pattern scores recorded on completion of the treatment phase (week 12). One (1) participant withdrew from the study after eight treatments due to work commitments; therefore, only 15 participants (treatment n = 7, control n = 8) were used for statistical comparison of pattern change from baseline to completion. There was a significant mean percentage decrease in pattern expression at week 12 compared to baseline for the secondary (56.3% decreased to 47.5%; p = 0.045) and tertiary patterns (48.1% decreased to 33.6%; p = 0.037) of the treatment group. No significant change in expression was found for the primary, secondary, or tertiary patterns for the control group or for the primary pattern associated with the treatment group (Figs. 3 –5).

Pattern expression percentage change for the primary patterns for the treatment and control group.

Pattern expression percentage change for the secondary patterns for the treatment and control group.
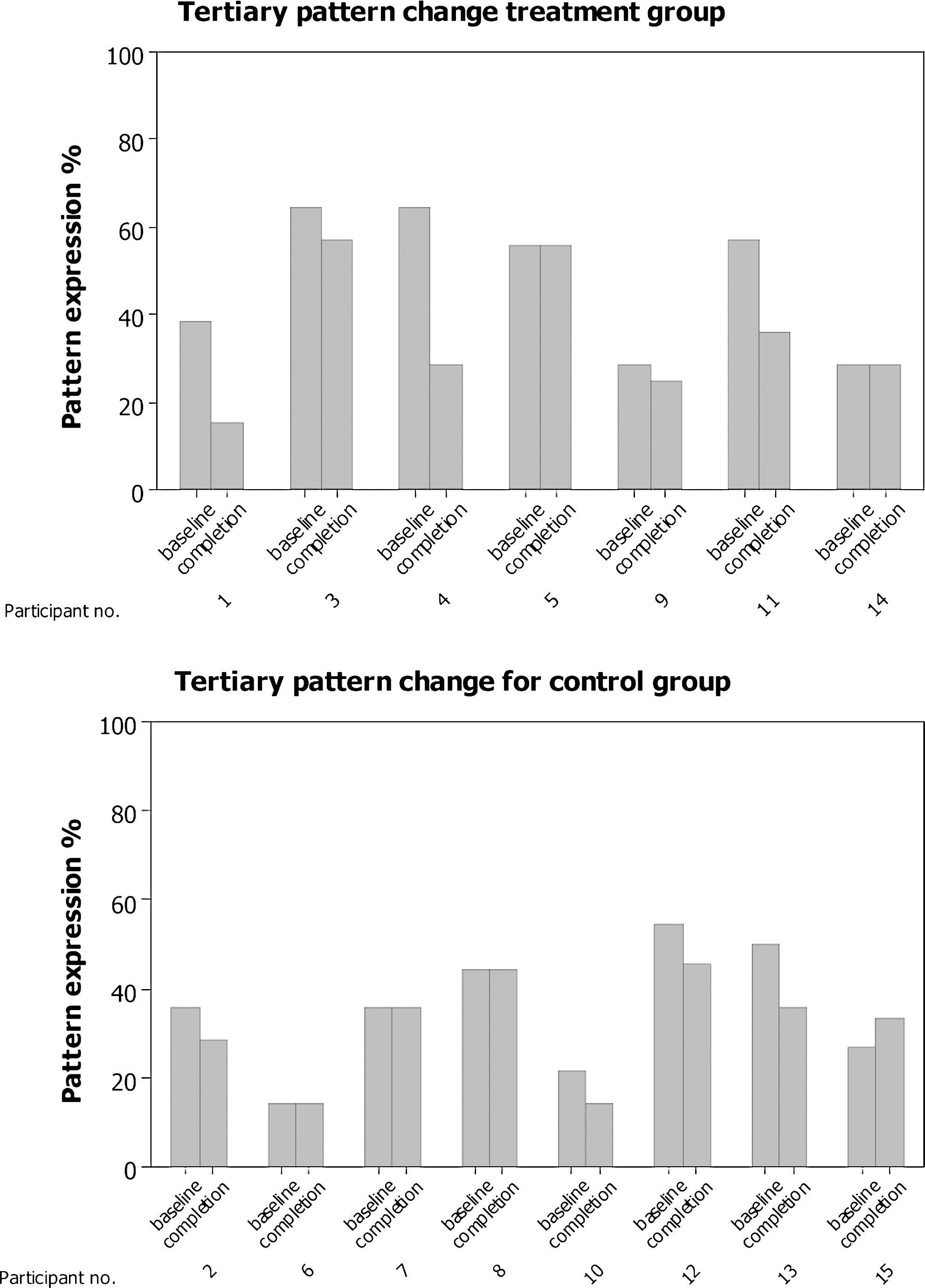
Pattern expression percentage change for tertiary patterns for the treatment and control group.
Discussion
TCM patterns were used as the basis for guiding treatment for this pilot study. While TCM pattern identification has previously been used as a basis for developing a treatment protocol in a clinical trial, this is the first time it has been used as an outcome measure. The process quantified the primary, secondary, and tertiary TCM patterns pre- and post-treatment phase, thereby allowing statistical evaluation of TCM pattern expression. A significant decrease in the expression of the secondary and tertiary TCM patterns for the treatment group was observed, suggesting an improvement in symptom/signs associated with these patterns.
In biomedicine, there has been a recent move to describe particular symptom clusters associated with specific diseases, including HCV, 23 acute bipolar mania, 24 cancer, 25,26 and diabetes mellitus. 27 This approach is being used to identify and monitor the disease and may have the potential to be a more sensitive instrument than pathology testing. 23 This method shares some similarities with the TCM pattern approach, which uses symptom clusters to formulate an individual treatment protocol. This pilot study has extended the use of TCM pattern expression to provide an additional TCM outcome measure.
During the study, it became apparent that a number of modifications could improve the sensitivity of the measure. For example, the TCM diagnostic pattern questionnaire only permitted the researcher to record whether the symptoms were present or absent. A rating scale with descriptors ranging from slight to strong expression for each symptom/sign would allow a more sensitive evaluation of the symptom change and consequently the TCM pattern.
Each primary, secondary, and tertiary TCM pattern was treated successively over 3 weeks and then repeated 3 times. There may have been some benefit in treatment prioritization with the primary pattern being treated more often than the secondary and tertiary patterns.
In the present study, the patterns were only assessed at baseline and at completion 12 weeks later. If the participants had been reassessed more regularly, it might have been possible to observe changes in the strength of the expression of the patterns and treatment protocols could have been changed or modified over the course of the trial. This process would more closely align with that of everyday acupuncture practice. For example, in the present study, of the 21 patterns (a primary, secondary, and tertiary pattern for each individual) that were present for the 7 participants in the treatment group at baseline, only 15 were still present as primary, secondary, and tertiary patterns at the completion of the study. This represents a 28% decrease in the expression of the TCM patterns over the course of the trial. In contrast, of the 24 primary, secondary, and tertiary patterns expressed by the 8 participants in the control group at baseline, 19 were still present at completion, representing a 20% decrease in TCM pattern expression. It should also be noted that 2 participants in the treatment group (participants 1 and 4) showed substantial reductions in the primary pattern, while no one in the control group demonstrated a similar percentage reduction. A more frequent pattern assessment and subsequent treatment modification might have achieved even further symptom/sign reduction for the treatment group.
The process of gathering and tabulating the symptom/sign diagnostic data was undertaken by the acupuncturist/researcher. One approach to maintaining accuracy while avoiding possible diagnostic bias would be to have the trial participant complete the symptom diagnostic checklists. An explanation or clarification could be supplied to the participant for unusual technical or Chinese medical terms.
Two important signs that need practitioner interpretation and were not evaluated in this study were the radial pulse and tongue characteristics. This is problematic in that information obtained from inspection of the tongue and palpation of the radial pulse is generally thought to be pivotal in determining the primary TCM patterns in clinical practice yet was not included in the study design. Over the last 10 years at the University of Technology, Sydney, two systematic data collection methods for diagnostic tongue features and radial pulse forms have been developed that demonstrate reasonable levels of reliability 28 (Kim M, Cobbin D, Zaslawski CJ, unpublished observations, 2009). Future studies should incorporate both of these methods into a TCM pattern practitioner-related diagnostic data collection process to consolidate the identification of the TCM patterns.
One criticism of the pilot study is the small number of participants. This may have led to the significant difference observed for TCM pattern expression between the treatment and control group for the primary pattern at baseline. A larger number of randomized participants would have ensured that such factors were distributed evenly across both intervention conditions.
Conclusions
This pilot study is the first to evaluate the effects of acupuncture on people with HCV. It was a randomized, single-blind, controlled pilot study with two parallel arms that used several objective outcome measures and a quality of life measure. The diagnostic and treatment process described in this article allowed the systematic assessment, documentary measurement, and evaluation of change in the symptom/signs associated with the primary, secondary, and tertiary patterns before and after the intervention phase. This method attempted to accommodate TCM practice within the framework of rigorous evidence-based medical research and quantified the TCM patterns for a specific disease.
Although this approach has been used for HCV, this method could be modified for any biomedical disease where sufficient documented diagnostic information exists in textbooks, journal articles, or research articles. If there is insufficient information available, a preliminary study such as an uncontrolled cohort study that identifies potential TCM patterns could be undertaken. To ensure intrarater reliability, trial participants should complete two TCM diagnostic questionnaires within a limited period of time, preferably within a day.
While there are a number of suggested modifications and improvements to the method, the authors believe that this approach is worthy of further study and should be incorporated into future acupuncture and Chinese medicine clinical trials. This will ensure a better understanding of TCM and facilitate the development of the evidence-based practice.
This methodology using symptom clusters could also be modified for use with any complementary and alternative medicine (CAM) therapy as an additional measure to evaluate change after the intervention phase. Biomedical testing may not relate to the patients' quality of life or the presence and severity of symptoms and therefore not be the best method to evaluate TCM and CAM disciplines that primarily focus on patients' health, patterns and symptom clusters.
Footnotes
Acknowledgments
This project wishes to acknowledge the support of Australian Acupuncture and Chinese Medicine Association (AACMA), Hepatitis C Council of NSW, and the Helio Supply Company for their donations and support.
Disclosure Statement
No competing financial interests exist.