
Abstract
Objective:
The objective of this study was to evaluate a program for managing myofascial pain syndrome (MPS).
Design:
The study design was a randomized controlled trial.
Setting:
The setting was the pain clinic of an academic hospital in Taiwan.
Participants:
Sixty-two (62) patients with a 3-month or longer history of MPS who were treated at this institution from July to November 2007 were included in the study.
Interventions:
The participants were randomized to an experimental group (n = 32) or a control group (n = 30). Both groups underwent trigger-point dry needling and muscle-stretch exercise regimen for passively stretching the affected muscles to their normal lengths; the experimental group then watched an 8-minute multimedia instructional video about MPS with supplemental handouts.
Main outcome measures:
The Brief Pain Inventory–Taiwan was administered at baseline and 1 month thereafter. The effect size model was used to measure the effects of Brief Pain Inventory–Taiwan. Bootstrap estimation was used to derive 95% confidence intervals for group differences.
Results:
Compared to the control group, the experimental group had significantly less interference of pain, lower intensity of present pain, and least pain (p < 0.05). Multiple regression analysis of patients with shoulder pain revealed significantly improved pain intensity and interference of pain (p < 0.05).
Conclusions:
The findings emphasize the importance of including patient education programs in MPS intervention.
Introduction
Educational intervention, which aims to increase patient knowledge and attitude, can improve the effectiveness of pain treatment by enhancing adherence to recommendations provided in medical consultations. 5 –7 Although Roth et al. 3 emphasized the importance of the patient education component of chronic pain intervention, particularly for patients with MPS, few studies have explored pain education programs for MPS. 8,9 This study therefore developed an MPS education program consisting of a multimedia video CD (VCD) and handouts and tested its effectiveness for relieving pain in patients who had received trigger-point treatments using a dry-needling technique. Modern technologies now enable the use of multimedia instructional programs combining text, graphics, audio, and video, which can enhance patient learning efficiency at reduced costs.
Comparative studies of pain relief methods indicate that dry needling is as effective as injected anesthetics such as lidocaine. 10,11 Their comparable effectiveness supports the theory that mechanically disrupted muscle fibers and increased blood flow are important factors in pain relief. 12 Techniques for passively stretching muscles to their normal lengths can deactivate trigger points, reduce referred pain, and improve range of motion. 13,14 This study evaluated the therapeutic use of trigger point dry needling followed by a postisometric exercise to relax the affected muscle.
Methods
Subjects
The subjects were patients with MPS referred for evaluation and treatment to the pain clinic of the Pingtung Christian Hospital (PTCH) in the city of Pingtung, Taiwan from July to November 2007. Inclusion criteria were the following: chronic musculoskeletal pain for more than 3 months due to nonspecific muscle pain; physical examination revealing a tender spot in a palpable taut band, patient pain recognition, referred pain pattern and local twitch response; 15 Chinese speaking; and age at least 18 years. Patients were excluded if they had any current diseases or conditions that might interfere with their participation, including fibromyalgia syndrome, neurological pain, infection, drug or alcohol abuse, rheumatologic disease, and pregnancy. The study design was prospective, interventional, and randomized controlled trial.
Informed consent and institutional review board approval
The research protocol was reviewed and approved by the institutional review boards of PTCH. Signed, informed consent was obtained from all subjects.
MPS education program
An MPS education program with instructional materials including VCD and handouts was developed after reviewing the literature on this condition and consulting pain experts. An 8-minute instructional VCD was developed, which included the following seven sections: (1) definition of MPS, (2) mechanisms of MTrP, (3) clinical characteristics and incidence, (4) pharmacological efficacy of MPS treatments, (5) perpetuating factors, (6) treatment modalities, and (7) conclusion. The handouts introduced trigger-point locations and muscle-stretching techniques described by Travell and Simons, 1 and the handouts were tailored to individual patient needs. The training program entailed viewing the instructional VCD and reviewing the handouts with a research assistant. Individual patient concerns were addressed in private 15- to 30-minute counseling sessions.
Instruments
After undergoing the dry needling procedure, each subject completed a questionnaire regarding demographic information (education, marital status), pain history, including previous interventions, occupational background, and history of systemic disease.
The Brief Pain Inventory (BPI) has been widely used in the United States and has been validated in several languages. 16 The Taiwan version of the BPI (BPI-T) uses a simple 0–10 numeric pain intensity scale to measure intensity of pain (sensory dimension) as well as interference of pain with daily life (reactive dimension). 16 Pain intensity was assessed by a four-item self-reported inventory requiring patients to rate their pain at the time of completing the questionnaire (present pain) and also to indicate whether the pain was the “worst,” “least,” or “average” within the previous week. Pain severity was measured on a scale from 0 (“no pain”) to 10 (“extreme pain”). A similar seven-item self-reported inventory was used to measure interference of pain with daily life activity, including general activity, mood, walking ability, normal work, relationships with others, sleep, and enjoyment of life. The anchor points for each of the interference scale items were “0” (“no interference”) and “10” (“extreme interference”). In addition to reporting present pain intensity, patients were instructed to document changes in pain type or nonpharmacological pain treatment. The α coefficient regarding internal reliability was 0.81 for the severity scale and 0.89 for the interference scale.
Procedure and needling protocol
This randomized controlled trial assigned subjects to experimental and control groups by random-number tables (Fig. 1) to ensure that the specialist conducting the standard clinical examination was blinded to patient group allocation. The standard clinical examination included routine procedures for diagnosing palpation of local tenderness, taut bands, local twitch responses, and referred pain. All needling procedures were performed by the same specialist. Taut bands with trigger points were isolated by palpation to ensure reproducibility of symptoms. Therapeutic needling was then performed with sterile 32G-diameter, 80-mm acupuncture needles. A needle plunger was used to pierce the skin and muscle with the acupuncture needle. The plunger was then removed, and a twitch response was elicited by inserting the needle further into the taut band.
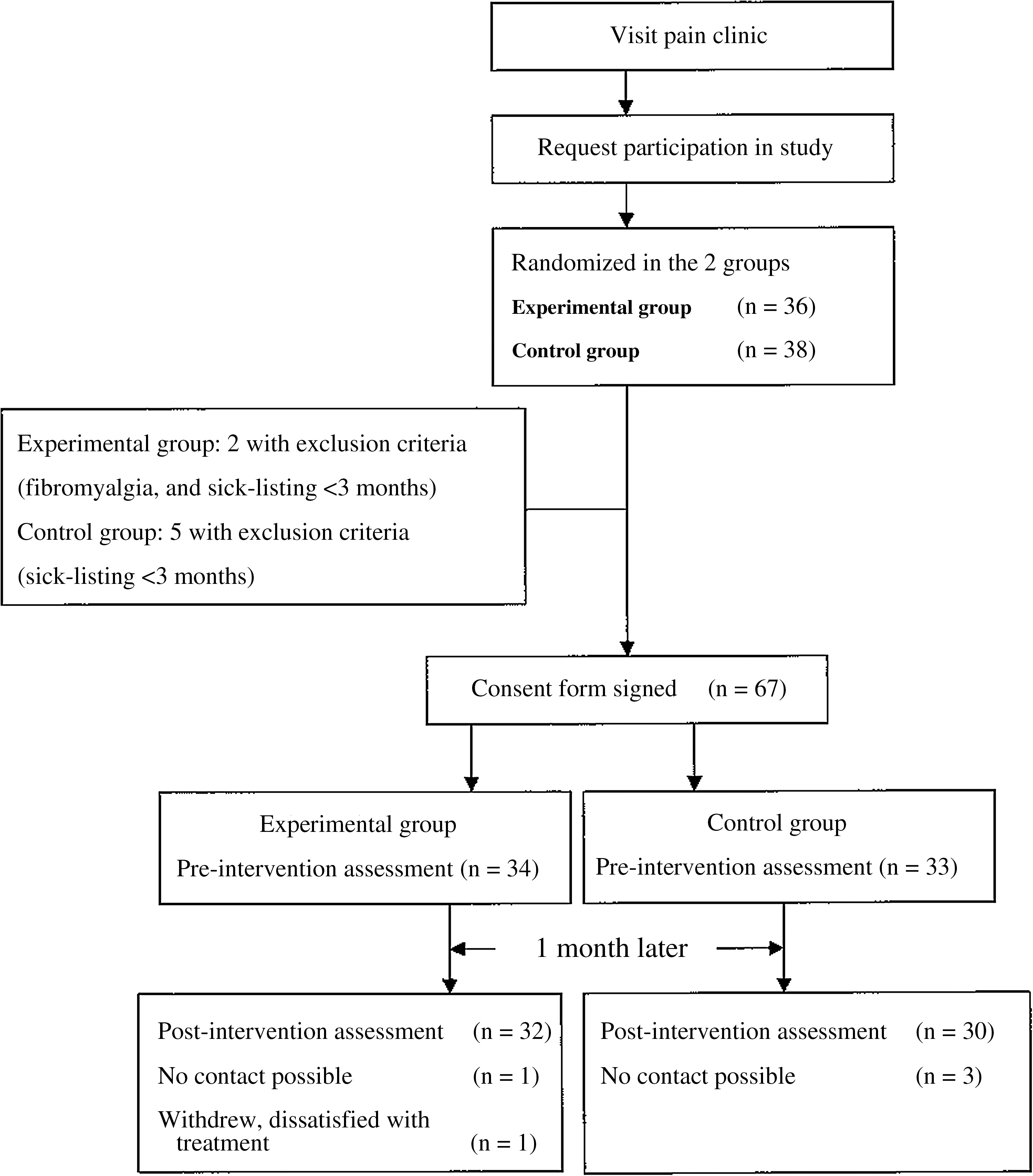
Progression of participants through the trial, including those with exclusion criteria, those who withdrew, and those with whom there was no follow-up.
Correct placement was confirmed by reproduction of recognizable pain or observation of local twitch response. The needle was then partially withdrawn and repeatedly inserted into the muscle until the pain and twitching stopped. By deactivating trigger points and reducing referred pain, the specialist could then passively stretch the affected muscle to its normal length. All patients were instructed in performing the muscle-stretch exercise protocol developed by Travell and Simons. 1
Two (2) trained research assistants collected all data from both groups in this study; the same researchers also delivered the education program to the experimental group. Baseline data were collected for both groups as follows: BPI-T at the pain clinic; follow-up BPI-T by telephone interview 1 month later. Patients in both groups completed questionnaires at the pain clinic. The experimental group was then given the multimedia MPS VCD and handouts tailored to their individual needs. The experimental group was encouraged to ask questions about the multimedia VCD and the muscle-stretch method. The control group received an 8-minute briefing on general intervention only; the research assistant provided additional information only when the patients asked questions.
Statistical analysis
Demographic and clinical characteristics were analyzed by descriptive statistics. A χ2 and t test were used to compare homogeneity between the two groups. Paired t test was used to test the effects of the educational program on pain relief. For group comparisons, effect size (ES) was used to standardize the extent of change measured by the BPI-T. An ES of 1.0 equals a change of 1 standard deviation in the sample. ESs of 0.2, 0.5, and 0.8 are typically regarded as indicating small, medium, and large changes, respectively. 17 A bootstrapping variance estimation was used to determine 95% confidence intervals for estimates of relative precision. 18
The improvement predictors of three domains of BPI-T (i.e., intensity of worst and present pain, aggregated pain interference) were calculated by backward regression analyses in which demographic variables, clinical characteristics, and baseline pain intensity and pain interference were entered into the regression equation. To avoid multicollinearity, the variance inflation factor (VIF) value was calculated for each independent variable. Variables were included if VIF <3. All data were analyzed using SPSS for Windows, version 15.0.
Results
The flow diagram in Figure 1 shows the number of participants at each phase of the trial (i.e., enrollment, randomization, exclusion, follow-up, and analysis). Table 1 details the demographic data for the two groups after randomization. The two groups did not significantly differ in baseline patient characteristics.
Low education corresponds to primary school training, middle to low level of high school training or college, high to high level of university or professional school education.
SD, standard deviation.
Table 2 also presents the baseline results for the BPI-T. Pain intensity and pain interference were assessed at baseline and again 1 month later. A notable finding of the paired t test for BPI-T after dry needling and the education intervention period was a significant positive change in pain intensity, including worst, least, average, and present pain in the experimental group (p < 0.05). However, after dry needling, the control group revealed a significant positive change in intensity of worst pain and average pain but no significant change in least pain or present pain. The experimental group had significantly reduced interference with general activity, mood, walking ability, normal work activity, relationships, sleep, and enjoyment of life (p < 0.05). In the control group, the only significant change was interference of pain with mood and sleep.
SD, standard deviation.
The ES refers to the method used for standardizing the extent of pain, pain intensity, and pain interference in comparisons between the experimental group and the control group (Table 3). In the experimental group, mood had the largest ES (–1.26); in the control group, worst pain had the largest ES (–0.71).
Effect size of pain intensity and pain interference = [mean (posttest) – mean (pretest)]/standard deviation (pretest).
95% confidence interval (CI) obtained by bootstrapping.
Differences are statistically significant if the 95% confidence intervals (95% CI) do not include 0. After bootstrapping, the 95% CI revealed that two subscale pain intensity scores (including present pain and least pain) and five subscale pain interference scores (including general activity, mood, walking ability, normal work, and relationships) were significantly reduced in the experimental group (Table 3).
Baseline worst pain, shoulder pain, and aggregated pain interference were significantly associated with improvement in worst pain (Table 4a). Baseline present pain, shoulder pain, and age were significantly related to improvement in present pain (Table 4b). The baseline aggregated pain interference, age, marital status (married versus single), and shoulder pain were significantly associated with improvement in aggregated pain interference (Table 4c).
Adjusted R 2: 0.54.
Aggregated pain interference score was computed by [(pain interference of general activity + mood + walking ability + normal work + relationship + sleep + enjoyment of life)/7].
Shoulder pain: Present versus absent.
Adjusted R 2: 0.55.
Shoulder pain: Present versus absent.
Adjusted R 2: 0.65.
Aggregated pain interference score was computed by [(pain interference of general activity + mood + walking ability + normal work + relationship + sleep + enjoyment of life)/7].
Marital status: Married versus not married; shoulder pain: Present versus absent.
Discussion
This study is apparently the first to explore the effects of a pain education program for patients with MPS. The efficacy of this study is reflected in the reduction of two subscale scores for pain intensity (worst pain and average pain) and two subscale scores for pain interference (mood and sleep) in both groups.
Worst pain is a common clinical indicator of treatment outcome and is highly correlated with pain interference. Pain severity also impacts quality of life; thus, worst pain is considered a good indicator of quality of life. 19 Consequently, improved worst pain may also improve pain interference and quality of life. In the experimental group in this study, reductions in worst pain and pain interference correlated with positive changes in general activity, mood, walking ability, normal work activity, relationships, sleep, and enjoyment of life. Worst pain did not significantly differ between the experimental and control groups, but the experimental group revealed significantly reduced interference of pain with general activity, mood, walking ability, normal work and relationships. The considerable improvement in interference of pain was likely due to the educational intervention comprising the instructional VCD about MPS self-care and personalized handouts describing the muscle-stretch exercises. The MPS VCD emphasized patient responsibility and the importance of psychosocial factors (e.g., coping). The patients were instructed in currently recommended techniques for elongating the affected muscle and restoring it to full-stretch length. 13 Unlike standardized interventions, the handouts in this study were individualized for each patient. 20,21 Despite the additional time required to produce the tailored handouts, they proved extremely valuable in this intensive approach to patient education. Dworkin et al. 22 demonstrated that carefully structured minimal interventions emphasizing self-management are highly beneficial to patients with temporomandibular disorders.
Strategies for managing pain, which is a constant problem in MPS treatment, usually emphasize patient education. Table 5 compares the results of four education intervention studies. 20,21,23,24 Two (2) studies reported success in reducing worst pain and low-back pain by increasing the duration of training periods and extending the professional training. A large-scale, long-term study discovered that education programs do not significantly improve worst pain and interference of pain with general activity, sleep, or mood. 21
Mood symptoms are extremely common in patients with MPS. In the experimental group, mood had the largest ES (–1.26). Present pain was also significant; in the experimental group, the ES of present pain (–0.78) was larger than that of worst and least pain intensity. The education intervention effectively reduced interference of pain with mood and present pain. These experimental results are consistent with Eich et al., 25 who reported an association between altered mood and self-reported present pain in patients with MPS. Affect is an important component of the pain experience, and present pain may have assimilative effects on memory that parallel those produced by emotions. Memory of past physical pain intensity such as maximum, usual, and minimum pain depends primarily on the intensity of present pain. 25 Feine et al. 26 noted that patients who report low levels of current pain tend to underestimate their pretreatment pain levels while those who report high current pain tend to overestimate their past pain. This finding implies that worst pain and average pain had a larger ES in the experimental group than in the control group.
The three regression models showed that shoulder pain is a significant predictor of improvement. Shoulder pain is a common health problem in Western societies 27 as well as in Taiwan. 28 Reports of pain in the general population vary substantially; 50% of all patients treated for shoulder pain by primary care physicians recover within 6 months without further treatment. 27 Both chronic and recurrent symptoms are common. Physiotherapy may reduce repeated primary care consultations for shoulder disorders, and steroid injections have marginal short-term effects on pain; alternative managements for shoulder pain include deactivating MTrPs and eliminating perpetuating factors. The MTrPs may be deactivated by stretching the involved muscle after cooling the skin with ethyl chloride spray, by trigger-point needling with an acupuncture needle, or by injecting local anesthetics. Hsieh et al. 29 demonstrated that dry needling of shoulder zone MTrPs effectively alleviates shoulder pain; in this study, patients with shoulder pain exhibited significantly improved pain intensity and interference after trigger point needling followed by stretching of the involved muscle.
Table 4a summarizes the worst pain regression models, which show that baseline aggregated pain interference correlates with improvement in worst pain. Worst pain impacts both patient quality of life and interference due to pain, so this finding may indicate that pain interference is an important predictor of improved worst pain.
Tables 4b and 4c show that age is negatively associated with improvement in present pain and aggregated pain interference. This conclusion is consistent with the findings of Turk et al., 30 who demonstrated that age-related differences in the mediatory role of cognitive factors are directly associated with pain and depression in elderly patients but not in young patients. These correlations suggest that the relationship between pain and depression varies according to age. Table 4c also shows that spousal support is positively associated with pain interference. Yu et al. 31 performed a cross-sectional study of the interference of pain with daily life and risk factors for chronic pain in an elderly Taiwan population. Their data indicated that single females and elderly subjects may be at risk for chronic pain and interference of pain with daily life. Although the findings of the current study should not be interpreted as indicating that older patients and single patients should expect poor improvement in pain interference, they do indicate the need for further research to elucidate this association.
The following limitations of this study are acknowledged. First, the sample size was inadequate for demonstrating improvement in all measurements taken. Second, although patient follow-up in this study revealed significantly greater pain improvement in the experimental group than in the control group, the pooled results of all statistical tests could not confirm whether the improvements were due to the treatment protocol. Third, the high cost of treating chronic pain associated with MPS was not discussed.
Conclusions
This study confirmed that a multimedia VCD and tailored handouts are effective for instructing patients in MPS management. In MPS therapy, the key strategies for minimizing recurrent or chronic pain are identifying etiological lesions that activate MTrPs, eliminating factors that perpetuate chronic pain, and providing patients with adequate educational programs and instructional materials. The experimental pain education program in this study proved effective for reducing pain intensity and pain interference.
Footnotes
Disclosure Statement
No competing financial interests exist.