
Abstract
Objective:
Prehypertension is a new category designated by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) in 2003. Managing prehypertension with nonpharmacological intervention is possibly beneficial to the prevention of hypertension. In this study, we observed the effect of slow abdominal breathing combined with electromyographic (EMG) biofeedback training on blood pressure (BP) in prehypertensives and assessed the changes of heart rate variability (HRV) in order to find an optional intervention to prevent hypertension and acquire some experimental data to clarify the underlying neural mechanism.
Methods:
Twenty-two (22) postmenopausal women with prehypertension were randomly assigned to either the experiment group or the control group. The experiment group performed 10 sessions of slow abdominal breathing (six cycles/min) combined with frontal electromyographic (EMG) biofeedback training and daily home practice, while the control group only performed slow abdominal breathing and daily home practice. BP and HRV (including R–R interval and standard deviation of the normal–normal intervals [SDNN]) were measured.
Results:
Participants with prehypertension could lower their systolic blood pressure (SBP) 8.4 mm Hg (p < 0.001) and diastolic blood pressure (DBP) 3.9 mm Hg (p < 0.05) using slow abdominal breathing combined with EMG biofeedback. The slow abdominal breathing also significantly decreased the SBP 4.3 mm Hg (p < 0.05), while it had no effect on the DBP (p > 0.05). Repeated-measures analyses showed that the biofeedback group + abdominal respiratory group (AB+BF) training was more effective in lowering the BP than the slow breathing (p < 0.05). Compared with the control group, the R–R interval increased significantly during the training in the AB+BF group (p < 0.05). The SDNN increased remarkably in both groups during the training (p < 0.05).
Conclusions:
Slow abdominal breathing combined with EMG biofeedback is an effective intervention to manage prehypertension. The possible mechanism is that slow abdominal breathing combined with EMG biofeedback could reduce sympathetic activity and meanwhile could enhance vagal activity.
Introduction
Some reports demonstrated that prehypertensives have a greater risk of cardiovascular events than normotensives. 2 –4 Early intervention significantly prevents or delays progression to hypertension or to other cardiovascular events. Lifestyle changes have been recommended for most prehypertensives by the JNC7, but there is limited evidence for its effectiveness. 5 This may be related to the diversity of factors affecting blood pressure (BP), among which stress exerts the most important influence. 6 –8 Therefore, relaxation trainings, such as autogenic training, progressive muscle relaxation, visualization and breathing exercises, qigong, and yoga, can be used for high BP intervention and have achieved some positive results. 9
Clinical trials documents reveal that slow abdominal breathing reduces BP, 10 –12 but there are also contradictory reports. 13 This may be partly because abdominal breathing lacks homologous physiologic feedback; therefore, the trainees cannot make accurate adjustments based on visualized signals of their physiologic feedback. This shortcoming may be corrected through biofeedback-assisted relaxation training, which is commonly used for relaxation training. With real-time visualization techniques, trainees can monitor changes in their physiologic signals instantly, which improves training skills and effectiveness. At present, biofeedback-assisted relaxation training has achieved significant efficacy in the treatment of hypertension. 14 –18 A meta-analysis carried out by Nakao indicated that biofeedback intervention decreased systolic (SBP) and diastolic blood pressures (DBP) more than nonintervention controls; however, only the relaxation-assisted biofeedback and not the simple biofeedback significantly decreased both SBP and DBP compared with sham or nonspecific behavioral interventions. 14 Kaushik et al. 19 found that biofeedback-assisted diaphragmatic breathing and systematic relaxation could prevent the starting event of vasoconstriction and counter the stress-mediated response in migraine by leading to parasympathetic stimulation and decrease in sympathetic overactivity. However, we find no clinical trials documenting biofeedback combined with slow abdominal breathing to prevent or delay progress to hypertension in prehypertensives.
Based on these evidences, we assume that abdominal breathing combined with electromyography (EMG) biofeedback-assisted relaxation training could exert positive effects in reducing BP. We approach this problem by observing the changes of BP during abdominal breathing combined with electromyographic (EMG) biofeedback training in prehypertensives so as to provide experimental evidence for early intervention of prehypertension. Meanwhile, we analyzed the influence of abdominal breathing combined with EMG biofeedback on heart rate variability (HRV), 20,21 a noninvasive indicator used to reflect cardiac autonomic nervous function, in order to explore the underlying neural mechanisms.
Materials and Methods
Participants
Twenty-six (26) postmenopausal women (right handed, ages 45–60 years, and averaged 52.55 ± 3.81 years) with prehypertension from two communities of Guangzhou enrolled in this study. They were randomly assigned to two groups: experimental group (n = 13, biofeedback group + abdominal respiratory group, AB + BF) and control group (n = 13, simple abdominal breathing group). During the experiment, 4 patients (1 from the AB + BF group and 3 from the control group) dropped out because of conflicting schedules. Twenty-two (22) participants completed this study. All participants stopped using any drugs during the month prior to initiation of the experiment. Exclusion criteria were cardiovascular and cerebrovascular diseases, respiratory diseases, autoimmune diseases, diabetes, neuropathy, and other autonomic neuropathies.
This study was performed in the Laboratory of Biofeedback, Department of Physiology, Zhongshan School of Medicine, Sun Yat-sen University, People's Republic of China. The protocol was approved by the local ethics committee. Informed written consents were obtained from all participants.
Procedure
Before the experiment began, all participants received slow abdominal breathing training to grasp the essential skills. The participants were asked to lie supine with an inductive belt (JD/PW-5; Boda Electron Co., Beijing, China) connecting their abdomens to a personal computer (Lenovo, M4600 P3.0HT 25640VN), and raised their hands to the abdomen and chest to feel each breathing pattern: abdominal or thoracic breathing. Then, they were instructed to apply abdominal breathing, and subsequently, they were instructed to reduce their respiratory rate to six times per minute gradually while increasing respiratory amplitude. The amplitude and frequency of abdominal movement could be instantly viewed from a screen in front of the participants in order to guide their adjustments in breathing patterns and frequencies (respiration biofeedback). After participants mastered the slow abdominal breathing essentials, the experiment could proceed to the next section.
Both groups of participants received 10 sessions of treatment once every 3 days. Each session lasted 25 minutes; the initial 5 minutes of the session were set aside for baseline recording and the remaining 20 minutes for treatment. An electrocardiogram (ECG) was recorded simultaneously. The participants were asked to refrain from alcohol, caffeine, tea, and spicy food on the day before each appointment. All participants were instructed to rest for 20 minutes to adapt to the laboratory before each session. The treatment was conducted at the same time of day in a quiet laboratory, with controlled air temperature (24°C–26°C) and relative humidity (60%–70%).
The subjects in the AB+BF group were treated by coupling the slow abdominal breathing with the frontal EMG biofeedback-assisted relaxation training. The relaxation techniques were similar to autogenic training and guided imagery, including relaxing the frontal muscle, mimetic muscles, masseter, shoulders, and limbs gradually, imagining the arms and legs limp and heavy, and imagining the hands and feet getting warmer and warmer. 21 During the AB+BF training, participants were instructed to lie in a comfortable bed, and three electrodes (one reference electrode and two recording electrodes) were fixed over the frontal muscle and connected to a biofeedback machine (JD/PW-5; Boda Electron Co.). The participants were then instructed to take the abdominal breathing described above (six cycles/min, with respiration biofeedback) and to attempt to relax with the relaxation techniques to lower the amplitude of their frontal EMG signal (feedback signal), which was displayed in the monitor of the biofeedback machine 1 m above their eyes. The frontal EMG signal was displayed as a yellow cursor that moved rightward when the amplitude of the frontal EMG signal increased, and vice versa. The target level was set 5% below the baseline value of the EMG signal. When the EMG signal decreased below the target level, the color of the cursor would change to green. The participants were encouraged to relax with the relaxation skills and make the yellow cursor move leftward and change to green. If the EMG signal decreased below the target level and lasted for 2 minutes, a new target level was reset automatically 2% below the prior target by the biofeedback machine. During the interval between each session, the participants in the AB+BF group were asked to perform the same procedure (without biofeedback) twice every day at home, with each period lasting 20 minutes.
Participants in the control group underwent the same protocol as the AB+BF group with the exception of the relaxation-assisted biofeedback treatment. Specifically, participants in the control group were simply instructed to perform the slow abdominal breathing (six cycles/min, with respiration biofeedback) during each session, while participants in the biofeedback group were instructed to perform the slow abdominal breathing and the EMG biofeedback with relaxation techniques. During the interval between each session, the participants in the control group were asked to perform the slow abdominal breathing (six cycles/min, counted by themselves without respiration biofeedback) twice every day at home, with each period lasting 20 minutes.
BP was measured before and after each session by the same research assistant using a mercury sphygmomanometer according to the standard guidelines. 1 At least three measurements were made. The mean of the last two stable readings was recorded. The BP measured at the beginning of the first session was regarded as the pretreatment value, and the BP measured at the beginning of the 10th session was regarded as the post-treatment value. One (1) and 3 months after the study was completed, the BP of the participants was measured and designated as the follow-up value.
The ECG was recorded simultaneously during each session to evaluate the HRV. The ECG (lead II) signal, amplified by a preamplifier (Cl-810232, Gould Inc., OH) and processed via a 12-bit analog-to-digital converter (BL-420, Taimeng Technology Corp., Chengdu, China), was recorded by a computer with a sampling rate of 1 kHz. The ECG recorded at the initial 5 minutes in the first session was regarded as the baseline for pretreatment (prebaseline data). The ECG recorded during the initial 5 minutes of the 10th session was regarded as the baseline for post-treatment (postbaseline data), and the recordings during the last 5 minutes in the 10th session were collected as the treatment data for post-treatment (training data).
HRV analysis
All ECG data were carefully checked through visual screening. Artifacts were edited following the user's manual for the BL-420. No beats were manually deleted so as to avoid bias. Since the HRV analysis software could only process the R-R interval text file, the primary ECG data were transformed and saved as an R–R interval text file using software edited with MATLAB software platform, version 7.1 (The MathWorks Inc., Natick, MA). In the editing process, the peaks of the R-wave were automatically labeled and each R–R interval was calculated by the software. If the EEG baseline shifted, the R–R interval may not be accurately calculated as the peaks of the R waves could not be labeled at the precise position and hence should be adjusted manually.
The HRV analysis software (HRV Analysis Software, version 1.1 SP1) designed and donated by Biomedical Signal Analysis Group (Department of Physics, University of Kuopio, Finland) was utilized to assess several measures of HRV, including R-R interval and SDNN [standard deviation of the normal–normal intervals].
Statistical analyses
Data were analyzed using SPSS, version 12.0 (SPSS Inc., Chicago, IL). Results are presented as mean ± standard deviation. A p value <0.05 was considered significant.
Independent samples t test was applied to examine the baseline demographic characteristics of participants. Paired t test and repeated-measures analyses of variance were applied to examine the changes of BP. In the repeated-measures analyses of variance, the within-subjects factor was time (BP measured at different times), and the between-subjects factor was treatment (AB+BF and control). The Greenhouse-Geisser correction was used for the analyses to correct type I error created by the violation of the sphericity assumption. Paired t test and independent samples t test was used to assess the changes of HRV during the experiment.
Results
The characteristics of participants
Table 1 shows the baseline demographic characteristics of 22 participants allocated to two different groups. There was no significant difference between the two groups.
Values are expressed as mean ± standard deviation; AB+BF, abdominal breathing combined with biofeedback; BMI, body–mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; TABP, type A behavior pattern scale; TH, time hurry; CH, competitive and hostility.
BP changes after the experiment
Paired t test was applied to assess the BP variance after 10 sessions of training. With the progression of training, the SBP and DBP of the participants in both groups decreased gradually. After 10 sessions of training, the AB+BF training significantly decreased the SBP by 8.4 mm Hg (from 133.58 ± 4.46 to 125.17 ± 5.54 mm Hg, p < 0.001) and the DBP by 3.9 mm Hg (from 81.92 ± 4.83 to 78.00 ± 3.19 mm Hg, p < 0.05). At the follow-up of 1 and 3 months after the experiment, the SBP was also kept at a low level (125.25 ± 4.39 and 125.08 ± 4.85 mm Hg, compared with the baseline, p < 0.001, respectively), but the DBP changed differently (78.67 ± 2.87 and 79.17 ± 2.41 mm Hg, compared with the baseline, p < 0.05 and p > 0.05, respectively). The slow abdominal breathing also significantly decreased the SBP 4.3 mm Hg (from 133.90 ± 4.56 to 129.60 ± 4.28 mm Hg, p < 0.05) after 10 sessions of training. However, it had no remarkable effect on the SBP at the follow-up of 1 and 3 months. The slow abdominal breathing had no effect on the DBP either after 10 sessions of training or during the follow-up.
Repeated-measures analyses of variance were applied to assess the different influence of the two trainings (abdominal breathing plus EMG biofeedback versus abdominal breathing) on the BP. The results showed that there were remarkable main effects of treatment and time on SBP; the treatment × time interaction for SBP was also significant (Table 2). The results of the repeated-measures analyses of SBP indicated that AB+BF training was more effective in lowering the SBP than slow breathing alone. Although neither main effect of time on DBP nor treatment × time interaction for DBP was found, the main effect of treatment on DBP was significant (Table 2). Under this situation, evaluating the difference between the two groups was based on the main effect of treatment. Therefore, this result also indicated AB+BF training was also more effective in lowering the DBP than slow breathing alone.
BP values are expressed as mean ± standard deviation. SBP, systolic blood pressure; AB+BF, abdominal breathing combined with biofeedback; DBP, diastolic blood pressure.
HRV changes during the training
The R-R interval baseline of the participants in both groups did not change remarkably after the experiment, but the R-R interval increased significantly during the training in the AB+BF group (p < 0.01, Fig. 1). And, during the training, the difference of R-R interval between the two groups is remarkable (p < 0.05, Figure 1). No remarkable change was found in the SDNN baseline of both groups after the experiment. However, during the training, it increased remarkably in the AB+BF group (p < 0.01, Fig. 2); it also increased significantly in the control group (p < 0.05, Fig. 2). No remarkable difference was found between the control group and the AB+BF group during the training (p > 0.05, Fig. 2).

Effect of different training on R–R interval. *p < 0.01, training versus postbaseline; Δ, p < 0.05, AB+BF group versus control group; AB+BF, abdominal breathing combined with biofeedback; prebaseline, baseline for pretreatment; postbaseline, baseline for post-treatment.
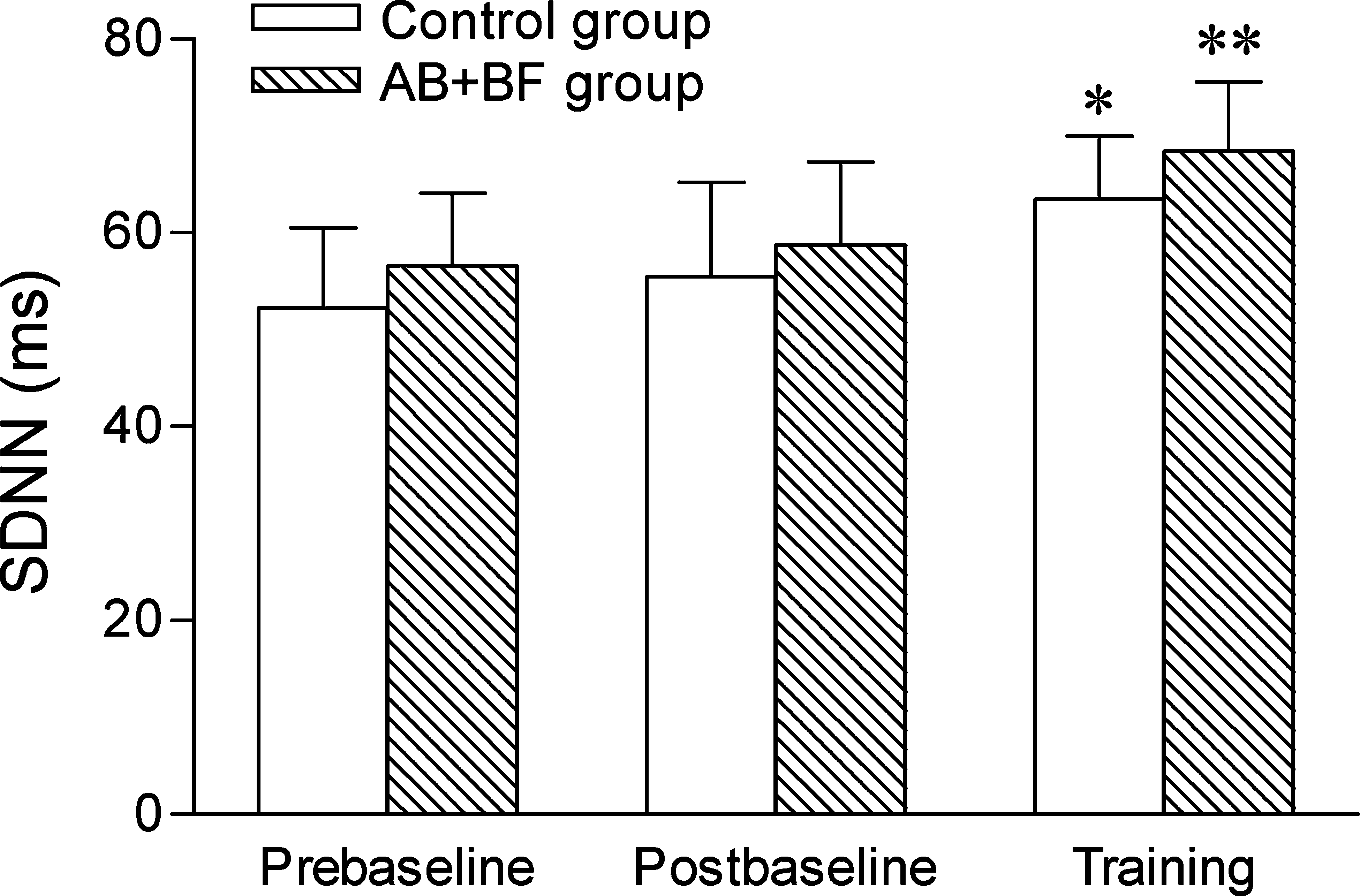
Effect of different training on SDNN. *p < 0.01, **p < 0.01, training versus postbaseline; SDNN, standard deviation of the normal-normal intervals. AB+BF, abdominal breathing combined with biofeedback; prebaseline, baseline for pretreatment; postbaseline, baseline for post-treatment. SDNN, standard deviation of normal–normal intervals.
Discussion
According to the present diagnostic criteria of hypertension, prehypertension is regarded as a normal BP that need not be treated. However, the increasing of BP and the increasing of cardiovascular disease is a slowly evolving process. An increasing body of research has shown that those with prehypertension are at a higher risk for hypertension 22 and cardiovascular disease. 2,3 Compared with the normotensive individual (office BP <120/80 mm Hg), the common carotid artery intima-media thickness and left ventricular mass of prehypertension are significantly higher, which shows that prehypertension status is cross-sectionally associated with subclinical atherosclerosis and target-organ damage. 4 Therefore, it is essential to find a nonpharmacological way to treat prehypertension.
In general, biofeedback has been more successful in the treatment of hypertension when respiratory therapies have been a component of the biofeedback. 23 McGrady 24 has established that certain types of patients with hypertension with a high degree of sympathetic arousal fare better with biofeedback than others. We found that AB+BF could lower the SBP by 8.4 mm Hg and DBP by 3.9 mm Hg on prehypertension. This BP-lowering effect could last 3 months at least. This was similar to the effects on BP by simple breathing training 10 –12 and by simple biofeedback training. 16,25 However, results of the self-matching comparison showed that slow abdominal breathing relaxation only had a relative long-term effect on the systolic pressure, but it had no remarkable effect on the SBP in the follow-up, and it has no significant effect on the diastolic pressure, which is pertinent with the results observed by Altena et al. 13 but not consistent with all other studies. 10 –12
The mechanism by which biofeedback and slow abdominal breathing regulates the BP is still unclear. As is known, the autonomic nervous system is responsible for the regulation of BP. In this study, we applied HRV analyses that reflect cardiac autonomic nervous function to explore the potential mechanism underlying the BP changes.
We found that slow abdominal breathing at six cycles/min had no effect on R-R interval (Fig. 1) while it increased SDNN (R-R interval fluctuations, Fig. 2). This is consistent with the results reported by Joseph et al. 26 and Bernardi et al. 27 The increase of R-R interval fluctuations has some effects of improving arterial baroreflex sensitivity, 26,28 reducing sympathetic activity, 29,30 and reducing chemoreflex sensitivity (deriving from the activation of the Hering-Breuer reflex induced by the increased tidal volume), which in turn enhances the baroreflex sensitivity. 27 All of them may contribute to lower BP. It has been demonstrated that slow breathing has a short-term effect of reducing BP. 26 In this study, we found that slow breathing had a relative long-term effect of reducing SBP, but it has no significant effect on DBP. This can be explained by the relatively short practice time. Much longer practice than this study, such as in qigong and yoga, might be expected to gain a better result. Another reason for it may be due to the lack of corresponding feedback signals that reflect the body's state in slow abdominal breathing relaxation. Without the feedback signals, participants could not make proper adjustment to get a greater relaxation state, thus achieving a relatively lower effect in reducing the BP. To achieve a more effective power, another intervention that could provide feedback signals, such as EMG biofeedback, should been coupled with slow breathing training.
EMG biofeedback-assisted relaxation, as a nonpharmacological therapy, is commonly used for relaxation training. In this study, slow abdominal breathing combined with EMG biofeedback had a more powerful effect of reducing BP (Table 1), and also increased the R-R interval (Fig. 1) and SDNN remarkably (Fig. 2). It is consistent with the prior report, which showed that the combination of respiratory and cardiac biofeedback training biofeedback increased HRV (SDNN) in patients with coronary artery disease, and the increasing of SDNN indicated that patients' status was improving from the “unhealthy” range to the “compromised health” range. 31
The induction and maintenance of hypertension proved to be closely related to stress 6 –8 and increased tension of the sympathetic nervous system. 32 –34 Biofeedback, as a nonpharmacological intervention, proved to have the effect of improving vagal tone as it inhibits sympathetic activity. 21,35,36 Therefore, the effect of slow breathing on BP will be enhanced when combined with EMG biofeedback. Meanwhile, with the feedback signals provided by the EMG biofeedback machine, participants feel their psychophysiologic status, which benefits them to perform the slow breathing with more relaxation. In view of these, we suggest that slow abdominal breathing combined with EMG biofeedback, by reducing sympathetic tone, may improve vagal nerve tension, resulting in inhibiting stress reaction as well as lowering BP.
A limitation of this study is that all participants were postmenopausal women. Postmenopausal women are inclined to have an increasing incidence of hypertension; therefore, they are more concerned about their own health, and their willingness to participate in this study is higher than in their counterparts. In addition, in order to avoid possible effects of changes of sex hormone levels on BP, this study used as subjects women in the older age group. Another limitation is the relatively small sample. In light of this, we only designed two groups, which led to the result that only an additive effect of slow breathing combined with EMG biofeedback on BP was found. To determine the predominant effect, a nonintervention control group and/or a simple biofeedback group should have been included. Nevertheless, the results of this study suggest that one nonpharmacological intervention assisted with another may improve the therapeutic efficacy.
In summary, consistent with other nonpharmacological intervention to lower the BP in hypertensive, slow abdominal breathing combined with EMG biofeedback can effectively reduce BP in those suffering from prehypertension. This occurs possibly by increasing the excitability of the vagus nerve and reducing the excitability of sympathetic nerves.
Conclusions
Slow abdominal breathing combined with EMG biofeedback is an effective intervention to manage prehypertension. This effect lasted at least 3 months. The possible mechanism is that slow abdominal breathing combined with EMG biofeedback could reduce sympathetic activity, enhance vagal activity.
Footnotes
Acknowledgments
This study was supported by Guangdong province Science Foundation (no. 2007J1-C0171). We gratefully acknowledge the efforts of all of the volunteers. The help of the technical staff Weidong Li is highly appreciated.
Disclosure Statement
No competing financial interests exist.