
Abstract
Objective:
The purpose of this study was to find out which experiences adults are making while treating children with complementary and alternative medicine (CAM) therapies in German-speaking Switzerland.
Design and subjects:
A cross-sectional survey was performed on adults accompanying the children presenting to an urban, tertiary pediatric emergency department in Zurich; 71% of the distributed questionnaires (1143 of 1600) could be used for data analysis. The respondents were asked about their experiences while treating the child with CAM and—for comparison reasons—with conventional medicine (CM).
Results:
The respondents perceived the effectiveness of CAM therapies in general to be inferior to that of CM, although 49% of all respondents stated that CAM therapies were more effective than CM in certain cases/against certain diseases and 13% that CAM therapies were as effective as CM. Higher frequency of use and lower compliance were observed in the case of CAM, relatively to CM. Respondents described the direct costs for the patient of both types of medicine to be comparable. Ninety-three percent (93%) of the respondents experienced no side-effects with CAM therapies, whereas only 52% of the respondents stated the same about CM therapies; the observed side-effects of CAM were weaker than those of CM. Homeopathy was the most frequently used form of CAM (77% of all CAM users), followed by herbal medicine (64%), anthroposophic medicine (24%), Traditional Chinese Medicine (13%), Ayurveda (5%), and others (34%).
Conclusions:
From the respondents' point of view, the most marked difference between CAM- and CM therapies concerns the frequency and intensity of side-effects, which were markedly higher in the latter case. The respondents made use of a wide variety of CAM therapies.
Introduction
CAM is often used in Switzerland. 12 –15 A survey published in 2002 described that 30% of the Swiss people did use some form of CAM: 12% had used homeopathy, 11% had used Traditional Chinese Medicine (TCM) or acupuncture, 5% herbal medicine (phytotherapy), 2% anthroposophic medicine, and 1% neuraltherapy. 16 The use of CAM in Switzerland, its efficacy, appropriateness, and cost-effectiveness have been evaluated within the frames of a federal program (Complementary Medicine Evaluation Program, PEK), which revealed that CAM was associated with a higher patient satisfaction, weaker/less frequent side-effects, and lower costs than conventional medicine (CM). 15,17 –20 The use of CAM by children in Switzerland has just started to be unveiled. A previous study performed at the intensive care unit of the Children's Hospital of Zurich revealed that 18% of the parents of critically ill pediatric patients applied some form of CAM. 21 In a previous report about the present survey, which was performed at the emergency department of the same hospital, 58% of all respondents (665 of 1143) stated that their child was using/had used some form of CAM therapies. 22
The aim of the present work was to reveal the experiences that adults—mainly parents—accompanying pediatric patients presenting to a pediatric, urban, tertiary emergency department were/are having while treating their child with CAM. The questionnaires used included items on (1) perceived effectiveness, (2) side-effects, (3) patients' compliance, (4) frequency of use, (5) costs, (6) reimbursement by health insurance, and (7) description of the CAM therapies used. Although the survey mainly addresses the experiences with CAM, in some cases and for comparison reasons, the respondents were asked to describe their experiences with CM as well.
Subjects and Methods
The present work is an analytical cross-sectional survey of the adults—mainly parents—accompanying the children presenting to the pediatric emergency department of the University Children's Hospital of Zurich between October 2006 and March 2007. The study was approved and conducted in accordance with the ethical standards set by the Hospital Ethical Review Board. Questionnaires were offered by the ward clerk to parents (or other caretakers) while these individuals were registering the child. Caretakers were asked to fill out the questionnaire, sign the consent form, and hand it back to the ward clerk, the nurse, or the front desk before leaving the department. German, English, French, and Italian versions of the patient information sheet, consent form, and questionnaire were available. The questionnaire included 34 multiple-choice questions, addressed the situation of pediatric patients, and was completely anonymous. 22 Exclusion criteria were (1) previously filled-out questionnaire; (2) inability of the respondent to read or write German, English, French, or Italian; (3) respondent was accompanying resuscitation/emergency patients; (4) lack of respondent (i.e., pediatric patient unaccompanied by a parent or another caretaker); and (5) respondent was accompanying a patient with emotional issues such as child abuse or psychiatric problems. All other accompanying persons were eligible for the study.
A questionnaire comprising 34 multiple-choice questions was used in which homeopathy, herbal medicine, anthroposophic medicine, Traditional Chinese Medicine (including acupuncture), and Ayurveda were specified. A pilot questionnaire, distributed to 20 families, was conducted to ensure the readability and clarity of the questions. Thereafter, minor revisions of the questionnaire—mainly involving its layout—were made. Patients' and respondents' demographic characteristics as well as behavior toward vaccination of CAM users and nonusers have been published elsewhere. 22,23
Questionnaires returned with fewer than 50% of the questions answered or with no answers to the specific questions were excluded from the analysis. The remaining survey results were entered into a computerized database using Remark Office OMR 6.0.4 (Gravic Inc., Malvern PA). Data entry was performed using a Microsoft Excel database, and all data were analyzed using SPSS for Windows version 14 (SPSS Inc., Chicago IL). The data on ordinal multiple-choice answer to some questions have been converted to fit in a range from 0 to 1 and averaged, in order to obtain values representative of either CAM or CM. Pearson's χ2 and Mann–Whitney U tests (always two-sided) were used to determine statistically significant differences between the representative values of CAM and CM, with a p-value of less than 0.05 considered to be statistically significant. Throughout the article, quotation marks are used to refer to the original text of the questionnaire (English version).
Results
Demographic characteristics of the respondents
Between October 2006 and March 2007, 1143 questionnaires (71% of those distributed) were available for analysis, 95% of which were in German. Fifteen (15; 0.9% of those distributed) returned questionnaires were not entered into the database as fewer than 50% of the questions were answered. Questionnaires were filled out by patients' mothers (65%, n = 701), fathers (32%, n = 353), or others (1%, n = 12). The sociodemographic characteristics of the respondents—including a comparison between the characteristics of CAM-users and nonusers—have been previously published in detail. 22 In brief, the children corresponding to the respondents were 5.6 years old, the mothers were 34.7 years old, and the fathers were 37.4 years old. Fifty-five percent (55%) of the children were boys, 89% of all children lived in intact families, and 92% were born in Switzerland. Fifty-four percent (54%) and 45% of the respondents reported that the father and the mother, respectively, had a high school education.
Effectiveness and tolerability of CAM- and CM therapies
How often CAM therapies “did have an effect” was described as “always” by 38% of the respondents (n = 242), “sometimes” by 52% (n = 331), “rarely” by 3% (n = 19), and as “never” by 5% (n = 33); in parallel, how often CM therapies “did have an effect” was answered as “always” by 62% (n = 473), “sometimes” by 34% (n = 262), “rarely” by 1% (n = 11), and “never” by 2% (n = 14) of the respondents. When these results were translated in a 0-to-1 scale (range: “never” = 0 to “always” = 1; see Fig. 1), the mean values for CAM and CM were 0.76 and 0.85 (p < 0.001) (i.e., the respondents rated the perceived effectiveness of CAM therapies to be statistically significantly lower than that of CM therapies). When asked to judge CAM therapies in comparison with CM, approximately half of the respondents (49%, n = 370) reported CAM therapies to be “more effective in certain cases/against certain disorders,” 13% to have an “equivalent effect” (n = 99), and 23% (n = 174) to be “less effective” than CM therapies; 3% (n = 26) of the respondents stated that CAM therapies are “not effective.”

Respondents' perception of complementary and alternative medicine (CAM)- and conventional medicine (CM) therapies. Respondents were asked to rate perceived effectiveness, side-effects, frequency of use, compliance to, and direct costs of CM therapies (black columns) and CAM therapies (white columns). Data from ordinal multiple-choice answers have been converted to fit in a range from 0 to 1 and calculated as described under Subjects and Methods.
Noticed side-effects of CAM therapies were described as “strong” by 1.4% (n = 9) and “weak” by 6% (n = 38), whereas 93% of the respondents (n = 580) indicated “no side effects.” The side-effects of CM therapies were reported to be “strong” by 10% (n = 73) and “weak” by 38% (n = 284); “no side-effects” was crossed by 52% (n = 381) of the respondents. The averaged result (range: “no side-effects” = 0 to “strong side-effects” = 1) of CAM was 0.05 and that of CM was significantly and markedly higher, namely, 0.22 (p < 0.001, Fig. 1).
Frequency of use of and compliance to CAM- and CM therapies
Frequency of use of CAM therapies was specified as “every day” by 8% of the respondents (n = 57), “1–4 times a week” by 7% (n = 45), “1–3 times a month” by 13% (n = 89), “1–10 times per year” by 55% (n = 368), and “never” by 17% (n = 116). On the other hand, the frequency of use of CM therapies was described as “every day” by 9% (n = 75), “1–4 times a week” by 2% (n = 12), “1–3 times a month” by 6% (n = 51), “1–10 times per year” by 71% (n = 570), and “never” by 12% (n = 93) of the respondents. The averaged results (range: “never” = 0 to “every day” = 1) for CAM- and CM therapies were 0.36 and 0.31 (p < 0.001), respectively, showing a significantly higher use of CAM than of CM (Fig. 1).
To compare the compliance toward CAM and CM, the questionnaires included an item on whether the child did “really get/take the prescribed therapies.” Concerning CAM therapies, 8% of the respondents marked “no” (n = 53), 3% answered “rarely” (n = 19), 9% “in part” (n = 57), 25% (n = 160) “mostly,” and 54% (n = 342) “always.” In the case of CM therapies, 4% of the respondents answered “no” (n = 32), 2% “rarely” (n = 16), 5% (n = 36) “in part,” 23% (n = 178) “mostly,” and 56% (n = 492) “always.” The averaged result (range: “no” = 0 to “always” = 1) of CAM was 0.78 and that of CM was 0.86 (p < 0.001), indicating a significantly higher compliance toward CM (Fig. 1).
Costs of CAM and CM
The respondents were asked to estimate the annual direct costs of CAM and CM concerning the respective child, “without counting the contributions paid by their health insurance and without insurance premiums.” The direct costs of CAM therapies were “1–100 SFr” (Swiss Francs, SFr = 1.50 Euros) for 55% of the respondents (n = 361), “100–200 SFr” for 23% (n = 151), “200–500 SFr” for 15% (n = 101), “500–1000 SFr” for 3.8% (n = 25), and “more than 1000 SFr” for 3.2% (n = 21). The direct costs of CM were: “1–100 SFr” for 46% (n = 348) of the respondents, “100–200 SFr” for 24% (n = 181), “200–500 SFr” for 21.8% (n = 164), “500–1000 SFr” for 4.8% (n = 36), and “more than 1000 SFr” for 3.2% (n = 24). The averaged results (range: “1–100 SFr.” = 0 to “more than 1000 SFr” = 1) for CAM and CM were 0.15 and 0.20, respectively. Although the difference was not statistically significant (p = 0.289), there was a tendency for slightly higher costs in the case of CM- than in the case of CAM therapies (Fig. 1).
The questionnaires included an item on whether “the child's health insurance pay[s] for complementary therapies.” Thirty-six percent (36%, n = 373) of all respondents believed that nearly all costs of CAM therapies would be covered by their insurance, 22% (n = 232) knew that at least a part of the CAM therapies were balanced, 5.7% (n = 59) described that no CAM therapies were balanced by their insurance, and 36% (n = 375) did not know. Sixty-five percent (65%, n = 412) of all CAM users had an additional insurance for CAM, 18% (n = 114) had none, and 17% (n = 112) did not know whether they had one (Fig. 2). In contrast, only 37% (n = 154) of the non-CAM users had an additional insurance for CAM therapies, 25% (n = 105) had none, and 38% (n = 158) did not know whether they had one.

How the respondents had organized and thought about the reimbursement of complementary and alternative medicine (CAM) therapies. Respondents were asked if the patients' insurance would reimburse CAM therapies, if patients had additional insurance for CAM, and whether they thought CAM therapies should be included in the basic health insurance. Data from conventional medicine users (black columns) and CAM users (white columns) are shown separately, in both cases as percentage of all answers.
Thirty-two percent (32%, n = 313) of all respondents were convinced that all CAM therapies should be included in the basic health insurance, 29% (n = 289) stated that “only the most usual complementary therapies” and 33% (n = 324) that “only the ones prescribed or practiced by a doctor” should be reimbursed. However, almost all respondents (96% of the CAM users and 89% of the nonusers) were of the opinion that some complementary therapies should be included in basic health insurance. Only 6% (n = 64) of all respondents would refuse inclusion of any CAM in the basic health insurance.
Different types of CAM
Fifty-eight percent (58%, 665 of 1143) of all respondents admitted that their child had used some form of CAM. 22 Seventy-seven percent (77%) of these CAM users used homeopathy, 64% used herbal medicine, 24% used anthroposophic medicine, 13% used TCM, 5% used Ayurveda, and 34% used other CAM therapies (various answers possible). Respondents were also asked to specify which therapies exactly—within these wide categories—the pediatric patients had received, by marking or not a long list of items (Table 1).
Percentage of all CAM users.
CAM, complementary and alternative medicine; S/P-factor, ratio between self-medication and therapies prescribed by physician; TCM, Traditional Chinese Medicine.
Self-medication versus therapies prescribed by physicians
Respondents were asked to specify who had prescribed the respective therapies, with the possibility to mark “auto-medication (family members, friends).” A ratio between therapies used as self-medication and therapies prescribed by “pediatricians, family doctors, therapists, children's hospital doctors, emergency doctors/emergency calls” was calculated to quantify the relative rate of self-medication (Table 1) and is referred to in the present article as “S/P-factor.” High rates of self-medication (S/P-factor higher than 1.5) were found in some forms of homeopathy (mixed medicaments on sale and Bach flower remedies) and phytotherapy (only compresses), as well as in Ayurveda, whereas nearly three of four therapies were not prescribed by a medical doctor, and in several of the CAM therapies mentioned under others. CAM forms with lower rates of self-medication were phytotherapy (S/P-factor 0.8), classical homeopathy (1.0), anthroposophic medicine (1.3), and TCM (1.0).
Parental requirements concerning CAM therapies
The respondents were asked “which medical systems should be included in the basic health insurance” (Fig. 3), with the possibility to mark “classical medicine” (chosen by 89% of all respondents, n = 846), “homeopathy” (72%, n = 687), “phytotherapy (herbal medicine)” (43%, n = 407), “anthroposophic medicine” (23%, n = 218), “Chinese medicine (TCM), acupuncture” (50%, n = 476), neuraltherapy (17%, n = 164), and/or “others” (5.6%, n = 53).
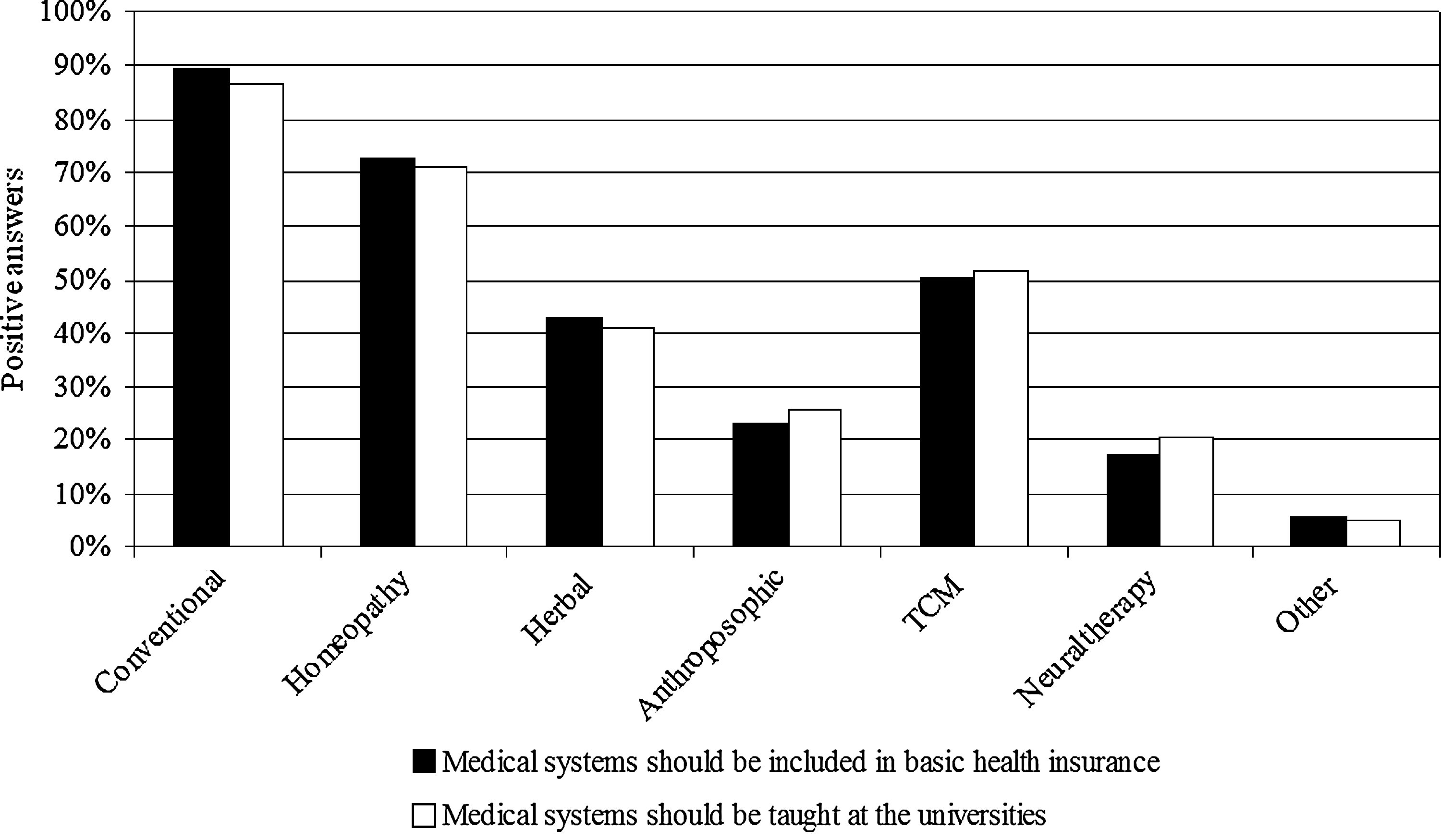
Respondents' opinions on which medical systems should be included in the basic health insurance and taught at the universities. Respondents were asked if conventional medicine, homeopathy, herbal medicine, anthroposophic medicine, Traditional Chinese Medicine (TCM), neuraltherapy, and others should be included in the basic health insurance (black columns) and taught at the universities (white columns). Data are shown as percentage of all answers.
Some of the respondents were convinced that some CAM therapies should be taught at the universities (Fig. 3), namely “homeopathy” (71%, n = 661), “phytotherapy (herbal medicine)” (41%, n = 382), “anthroposophic medicine” (26%, n = 239), TCM (52%, n = 481), “neuraltherapy” (20%, n = 190), and “others” (5.3%, n = 49). The answers of CAM users and nonusers were comparable (not shown).
Discussion
The present survey compared CAM with CM in terms of perceived effectiveness, side-effects, compliance, and costs, as these were experienced and communicated by the respondents. The results are based on the questionnaires filled out by adults—in 99% of the cases parents—accompanying pediatric patients presenting to the emergency unit, and reflect the experiences that they had so far. Most of them (58%, 665 of 1143) had experienced some form of CAM. 22
When asked to describe the perceived effectiveness of CAM and CM independently from each other, the respondents rated CAM as being somewhat less effective than CM. However, when asked to directly compare the perceived effectiveness of CAM therapies with that of CM, 62% of the respondents described CAM to be either “more effective in certain cases/against certain disorders than” or “equivalent effective to” CM. We interpret these results as indicating that although the respondents had the impression that in a general way CM is more effective than CAM, the majority of the respondents had already experienced situations in which CAM was at least as effective as CM.
The side-effects of CAM therapies turned out to be clearly more seldom and weaker than those of CM. This constitutes the most marked difference between the two types of therapies, which was revealed by the present survey, with the representative value for CAM being four times lower than the one for CM. Nevertheless, 6% of the respondents did notice weak side-effects and 1% even strong side-effects upon the use of CAM therapies, which is in disagreement with the widespread belief that CAM is harmless.
Taken together, the results on perceived effectiveness and tolerability suggest that although CAM might be slightly less effective than CM, its good performance in some clinical situations and the superior tolerability leads to a high satisfaction of the users, which might explain the widespread use of CAM among the respondents (58% 22 ). These observations seem to justify the recommendation of CAM therapies in certain situations, if accompanied by an individual assessment of the patient's risk situation by a medical doctor.
Slightly lower compliance and higher frequency of use were observed in the case of CAM, relatively to CM, suggesting different behaviors of the respondents toward the two types of medicinal systems. Interestingly, 12% of the children had never made use of CM and 17% did not use CAM therapies, revealing that either a considerable proportion of this population had been in very good health or that the parents refrained from going to a physician.
The direct costs for the patient of both types of medicine were comparable, with a tendency for higher costs being apparent in the case of CM. In Switzerland, the costs for CM are almost entirely covered by the obligatory health insurance. However, the costs for CAM are at present only reimbursed by the obligatory insurance in exceptional cases, and patients have to arrange for additional insurance if they wish CAM therapies to be reimbursed. Since a considerable number of the respondents did not have such an additional insurance for CAM, the present data on the direct costs of both types of medicine might indicate that in general CM is more expensive than CAM. Higher costs for CM relatively to CAM have been detected previously by PEK, when comparing the total annual costs of CM- and CAM physicians and the corresponding medication costs. 15
Fifty-three percent (53%) of the pediatric patients had an additional health insurance for CAM, corroborating the previously published value (approximately 50% 15 ) for the entire Swiss population. While this percentage was clearly higher in the case of CAM users, it is surprising that 37% of the nonusers possess this insurance as well. A possible explanation for this discrepancy might be that the insurance companies often offer an additional health insurance for CAM within a commercial package that comprises several other products. The majority of all respondents (96%) were in favor of the inclusion of some CAM therapies in the basic health insurance. This value outruns the results of a Swiss voting in favor of CAM, which took place in May 2009; the results of this voting in the region of Zurich showed that 62.4% of the voters had a positive attitude toward CAM. 24
One of our goals was to find out exactly which therapies the pediatric patients had used. While the questionnaire used in the present survey allowed us to identify a wide variety of CAM therapies, it should be noted that no attempt was made to mention only clearly therapeutic items; some items that might be considered under the category wellness/sports were allowed. The respondents mentioned a notorious variety of CAM therapies (depicted in Table 1) as having been used by the pediatric patients. A recent survey on family doctors in Switzerland shows that 30% of them do practice some form of CAM: 34% homeopathy, 34% herbal medicine (phytotherapy), 31% TCM/acupuncture, 11% anthroposophic medicine, 11% neuraltherapy, and 30% others. 25 Our data corroborate that homeopathy is the most used CAM therapy, followed by herbal medicine. The detected use of anthroposophic medicine (24% of all CAM users), however, was higher and that of TCM/acupuncture (13%) was lower in the present survey. Finally, neuraltherapy seems not to be practiced in children (0%).
A previous report on this survey showed that two thirds of the administered CAM therapies could be attributed to self-medication. 22 This high extent of self-medication might be worrying because side-effects, intoxications, and interactions between CAM and conventional therapies can occur. 26 –29 Some self-medication was reported in essentially all types of the CAM therapies; still, a few differences of the extent of self-medication among the various therapies were detected. The low numbers of respondents using some of the therapies mentioned under “others” prevent a proper interpretation of the corresponding data.
The major limitations of the study are the lack of clinical data and the exclusion of respondents who could not read or write German, English, French, or Italian. The limited number of available linguistic versions of the questionnaires might explain why Swiss people seem to be overrepresented in this survey: Whereas 21% of the people living in Canton Zurich are foreigners, 30 only 8% of the pediatric patients were not born in Switzerland. Another explanation is that due to the long process needed to acquire Swiss citizenship, the number of children classified as foreigners is probably much higher that the number of children actually born outside of Switzerland. Further limitations of our study might be a rather wide definition of CAM, the confinement of the survey to one emergency unit only, and the use of common language expressions—such as “all,” “never,” “sometimes”—without further (numerical) definition of what is exactly meant.
Strengths of the present survey are the high number of respondents and the elevated response rate, answering of the questionnaire in privacy, and the absolute protection of anonymity of the respondents. Because the approach followed in a survey is markedly different from those of interventional clinical trials, our data add qualitatively different information to several trials designed to compare defined CAM therapies and CM therapies with respect to effectiveness, side-effects, compliance, and/or costs.
Taken together, the data presented here show that for the respondents, adults accompanying pediatric patients presenting to the emergency department, the strongest difference between CM therapies and CAM therapies concerned the tolerability of the two types of medicinal systems, with clearly more seldom and weaker side-effects being experienced with CAM therapies. Within the wide range of CAM therapies that had been used by those pediatric patients, preferences for homeopathy, herbal medicine, and anthroposophic medicine could be detected.
Footnotes
Acknowledgments
We would like to thank the staff, parents, and children of the pediatric emergency department of Children's Hospital of Zurich for their time and cooperation. The multilingual translation of Anita Staubli is gratefully acknowledged. This publication was financially supported by the Paracelsus-Hospital of Richterswil (Switzerland) and the Johannes Kreyenbühl Academie.
Disclosure Statement
No competing financial interests exist.
This is a full-text article of an abstract accepted for presentation at ICCMR 2010 in Tromsø, Norway.