
Abstract
Objectives:
The authors present 3 cases of various pathologically confirmed malignancies (one gallbladder, one periampullary, and one liver). These patients underwent Psorinum therapy as the primary cancer treatment. Psorinum therapy is a homeopathic approach to treat patients with cancer.
Subjects:
According to the American Joint Committee on Cancer tumor, nodes, metastasis system, all 3 patients were diagnosed at Stage IV. Their Karnofsky performance status was between 20% and 50% and their Eastern Cooperative Oncology Group score status was between 3 and 4. In these cases, conventional cancer treatments could not be initiated due to the advanced stage of their disease, poor general health performance status, and their financial constraints.
Interventions and outcome:
In these patients, Psorinum-6x was administered orally at a dose of 0.02 mL/kg body weight/day on an empty stomach for a complete course duration of 2 years, along with allopathic and homeopathic supportive treatment. According to the Response Evaluation Criteria in Solid Tumors criteria, complete tumor response occurred in 1 case and partial tumor response occurred in the other 2 cases. All 3 patients remained alive and maintained a stable quality of life for at least 2 years. The patients reported no adverse side-effects from Psorinum-6x.
Conclusions:
This report indicates the clinical efficacy of Psorinum therapy in treating those 3 patients. Thorough basic research and well-designed clinical trials should be conducted for further investigation of this homeopathic cancer treatment in order to integrate it into the mainstream of oncology treatments.
Introduction
Case Reports
Case 1
A 72-year-old woman came to our cancer center on February 12, 2006 with severe abdominal pain, loss of appetite, nausea, vomiting, and abdominal distension. An upper abdominal CT scan on February 15, 2006 reported a mass in the gallbladder region, extending to the liver, with regional lymph node involvement, peritoneal metastasis, and ascites. Fine-needle aspiration cytology (FNAC) from February 16, 2006 showed adenocarcinoma of the gallbladder. Ascitic fluid cytology on February 17, 2006 reported metastatic adenocarcinoma. In this case, the American Joint Committee on Cancer (AJCC) tumor, nodes, metastasis system (TNM) staging was T3N1M1 or Stage IV, Karnofsky scale status was 20%–30%, and the Eastern Cooperative Oncology Group (ECOG) score status was 4. Conventional cancer treatments could not be initiated due to the advanced stage of the disease, poor general health performance status, and financial constraints of the patient's family.
At that time, the patient's life expectancy was less than 6 weeks. Psorinum therapy was started on February 18, 2006. Signed informed consent was obtained from the patient before starting the Psorinum therapy. Psorinum-6x was administered orally at a dose of 0.02 mL/kg body weight/day on an empty stomach for a complete course duration of 2 years. The dosing of the Psorinum was fixed according to the body weight of the patient measured at baseline. Supportive care for control of infection, pain, electrolytic imbalance, and nutritional deficiencies were taken from the allopathic stream. Analgesics were used to control pain; antibiotics were used to control infections; blood transfusions and nutritional supplements were provided according to the requirements. In case of homeopathic supportive care, mother tincture of Chelidonium majus and mother tincture of Carduus marianus were used to improve the liver function. Lycopodium 200c and Medorrhinum 200c were used to control cancer-related pain when required.
The patient was checked upon clinically at a regular interval of 4 weeks. Her symptoms and quality of life gradually improved. Improvements were also noted in routine blood tests (complete blood count [CBC], liver function tests [LFT], and so on). A follow-up CT scan was done on January 12, 2007, in which there was no evidence of previous abnormalities (i.e., gallbladder and liver mass, regional lymph nodal involvement, and ascites). Abdominal paracentesis was not done in this case. A complete response was observed here according to the Response Evaluation Criteria in Solid Tumors (RECIST). The patient stopped taking Psorinum after a 2-year full course on February 17, 2008. According to the last follow-up (May 16, 2009) she was alive and well without complaints of nausea or abdominal pain. At that time, her Karnofsky status was between 80% and 90% and ECOG status was 1 (Table 1 and Fig. 1).
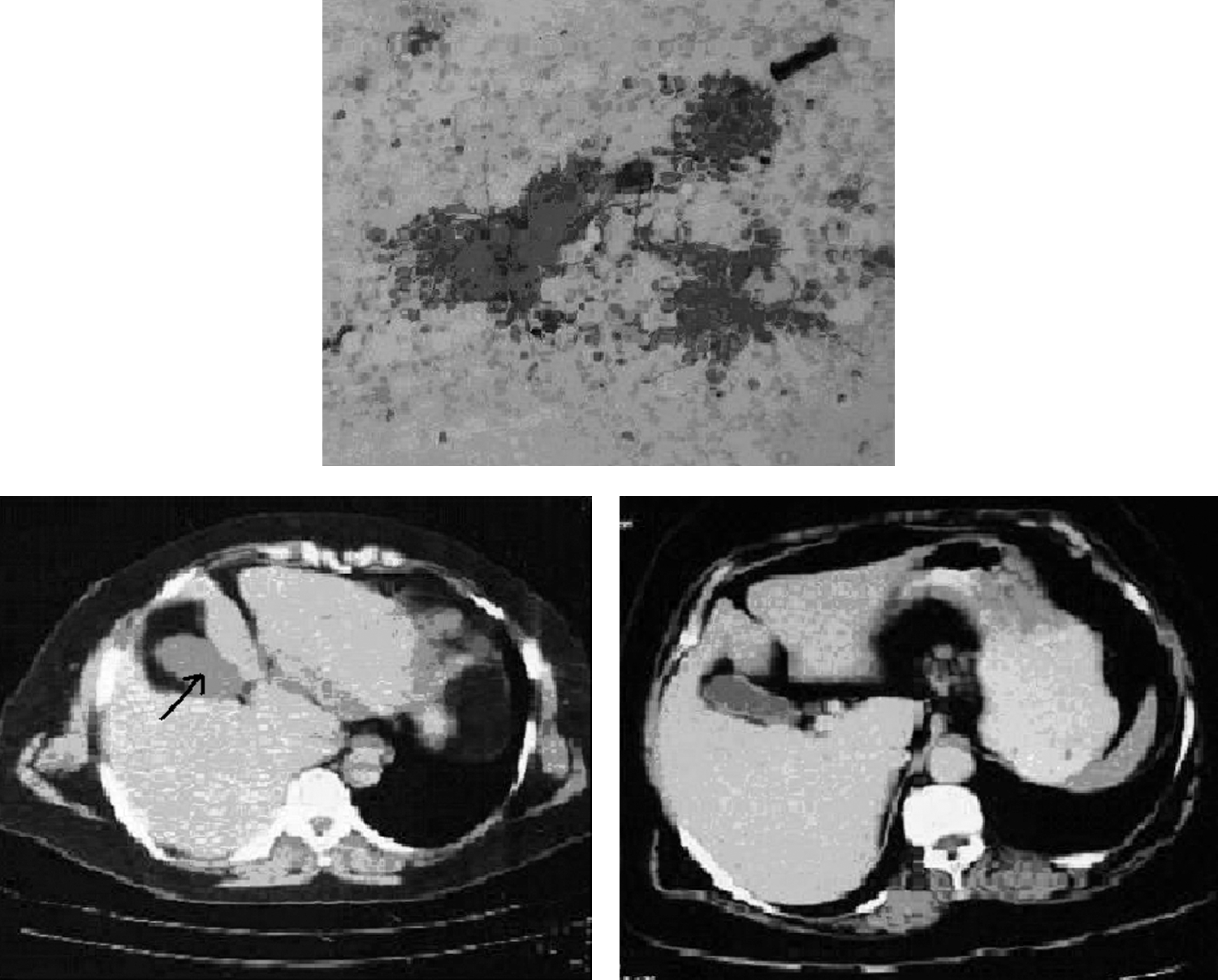
Case 1. Gallbladder cancer.
AJCC, American Joint Committee on Cancer; TNM, tumor nodes metastases; RECIST, Response Evaluation Criteria in Solid Tumors; FNAC, fine-needle aspiration cytology; GB, gallbladder; CT, computed tomography; CR, complete response; PR, partial response; SOL, space occupying lesion.
Case 2
A 60-year-old woman came to our cancer center on September 20, 2005 with jaundice, severe pain in the upper abdomen extending to the back, nausea, vomiting and general weakness. An upper abdominal CT scan of September 26, 2005 reported a dilated biliary tree and pancreatic duct, periampullary tumor growth, involvement of regional lymph nodes and a space-occupying lesion (SOL) in the left lobe of the liver. Endoscopic retrograde cholangiopancreatography (ERCP) was done on October 5, 2005 and a metallic stent was inserted into the common bile duct. ERCP revealed a periampullary tumor. CA 19.9 on October 14, 2005 was 2500 U/mL. Histopathology examination of the periampullary tissues on October 17, 2005 revealed adenocarcinoma. In this case, the AJCC TNM staging was T2N1M1 or Stage IV. Her Karnofsky scale status was between 40% and 50% and ECOG score status was 3. At that time, the patient's life expectancy was less than 8 weeks. Conventional cancer treatments could not be initiated due to the advanced stage of the disease, poor general health performance status of the patient, and financial constraints of the patient's family. Psorinum therapy was started on October 21, 2005. Signed informed consent was taken from the patient before starting the Psorinum therapy. Psorinum-6x was administered orally at a dose of 0.02 mL/kg body weight/day on an empty stomach for a complete course duration of 2 years. The dosing of the Psorinum was fixed according to the body weight of the patient measured at baseline. Supportive cares for control of infection, pain, electrolytic imbalance and nutritional deficiencies were taken from the allopathic stream. Analgesics were used to control pain; antibiotics were used to control infections; in addition, blood transfusions and nutritional supplements were provided according to the requirements. In case of homeopathic supportive cares, mother tincture of Chelidonium majus and mother tincture of Carduus marianus were used to improve the liver function. Medorrhinum 200c and Conium 200c were used to control cancer-related pain when required. The patient was checked upon clinically at a regular interval of 4 weeks. Her symptoms and quality of life gradually improved.
Improvements were also noted in the routine blood test (CBC, LFT, and others). CA 19.9 on August 5, 2006 decreased to 50 U/mL. A follow-up upper abdominal CT scan was done on August 8, 2006 and compared to the previous CT scan (September 26, 2005); there was significant regression of the periampullary growth and regional lymph node involvement, with no evidence of the previous liver SOL. In this case, a partial response was observed according to the RECIST response criteria. The patient stopped taking Psorinum after a 2-year full course on September 26, 2007. According to the last follow-up (July 12, 2009) she was still alive and well without complaints of jaundice, nausea, and upper abdominal pain. At that time, her Karnofsky status was between 80% and 90% and ECOG status was 1 (Table 1, Fig. 2).

Case 2. Periampullary carcinoma.
Case 3
A 55-year-old woman came to our cancer center on April 28, 2006 with nausea and vomiting, abdominal pain, and abdominal distension. She had been receiving antitubercular therapy for tubercular peritonitis since October 10, 2005. She was also a diagnosed case of hepatitis C (anti-hepatitis C virus positive). She had esophageal variceal band ligation for esophageal varices and portal hypertensive gastropathy. An upper abdominal CT scan of May 3, 2006 reported a large, irregular SOL in the liver involving segment V, VI, and VIII and showing extension into the porta region with thrombus of the right portal vein reaching just up to the portal vein confluence. Regional lymph node involvement and presence of ascites were also noted. Her α-fetoprotein (AFP) level on May 3, 2006 was 94,992.0 IU/mL. Cytology (FNAC) of the liver mass dated May 4, 2006 revealed hepatocellular carcinoma. TNM staging was T3N1M1, or Stage IV, the Karnofsky status was between 40% and 50% and ECOG status was 3. At that time, the patient's life expectancy was less than 6 weeks. Conventional cancer treatments could not be initiated due to advanced stage of the disease, poor general health performance status of the patient and financial constraints of the patient's family. Psorinum therapy was started on May 6, 2006. Signed informed consent was taken from the patient before starting Psorinum therapy. Psorinum 6x was administered orally at a dose of 0.02 ml/kg body weight/day on an empty stomach for a complete course duration of 2 years. The dosing of the Psorinum was fixed according to the body weight of the patient measured at baseline. Supportive treatments for control of infection, pain, electrolytic imbalance, and nutritional deficiencies were taken from allopathic medicine. Analgesics were used to control pain; antibiotics were used to control infections; blood transfusions and nutritional supplements were provided according to requirements. In case of homeopathic supportive care, mother tincture of Chelidonium majus and mother tincture of Carduus marianus were used to improve the liver function. Conium maculatum 200c was used for heart troubles and abnormal blood pressure. Medorrhinum 200c and Bryonia alba 200c were used to control cancer-related pain when required. The patient was checked upon clinically at a regular interval of 4 weeks. Her symptoms and quality of life gradually improved.
Improvements were also noted in the routine blood tests (CBC, LFT, and others). AFP level on May 23, 2006 decreased to 53,320.0 IU/mL. The AFP level on June 12, 2009 decreased to 15,800.0 IU/mL. Ascitic fluid cytology on June 19, 2006 revealed metastatic adenocarcinoma. AFP level on June 27, 2006 decreased to 13,766.0 IU/mL. A follow-up upper abdominal CT scan was done on July 22, 2006 and compared to the previous CT scan (May 3, 2006). There was significant regression of the liver mass, lymph node involvements, and ascites. Abdominal paracentesis was not done in this case. A partial response was observed here according to the RECIST response criteria. AFP level on August 26, 2006 decreased to 1000 IU/mL and on October 12, 2006 further decreased to 450 IU/mL. The patient stopped taking Psorinum after a 2-year full course on May 5, 2008. According to the last follow-up (May 21, 2008), she was alive and well without complaints of nausea or abdominal pain. At that time, her Karnofsky status was between 80% and 90% and ECOG status was 1 (Table 1, Fig. 3).
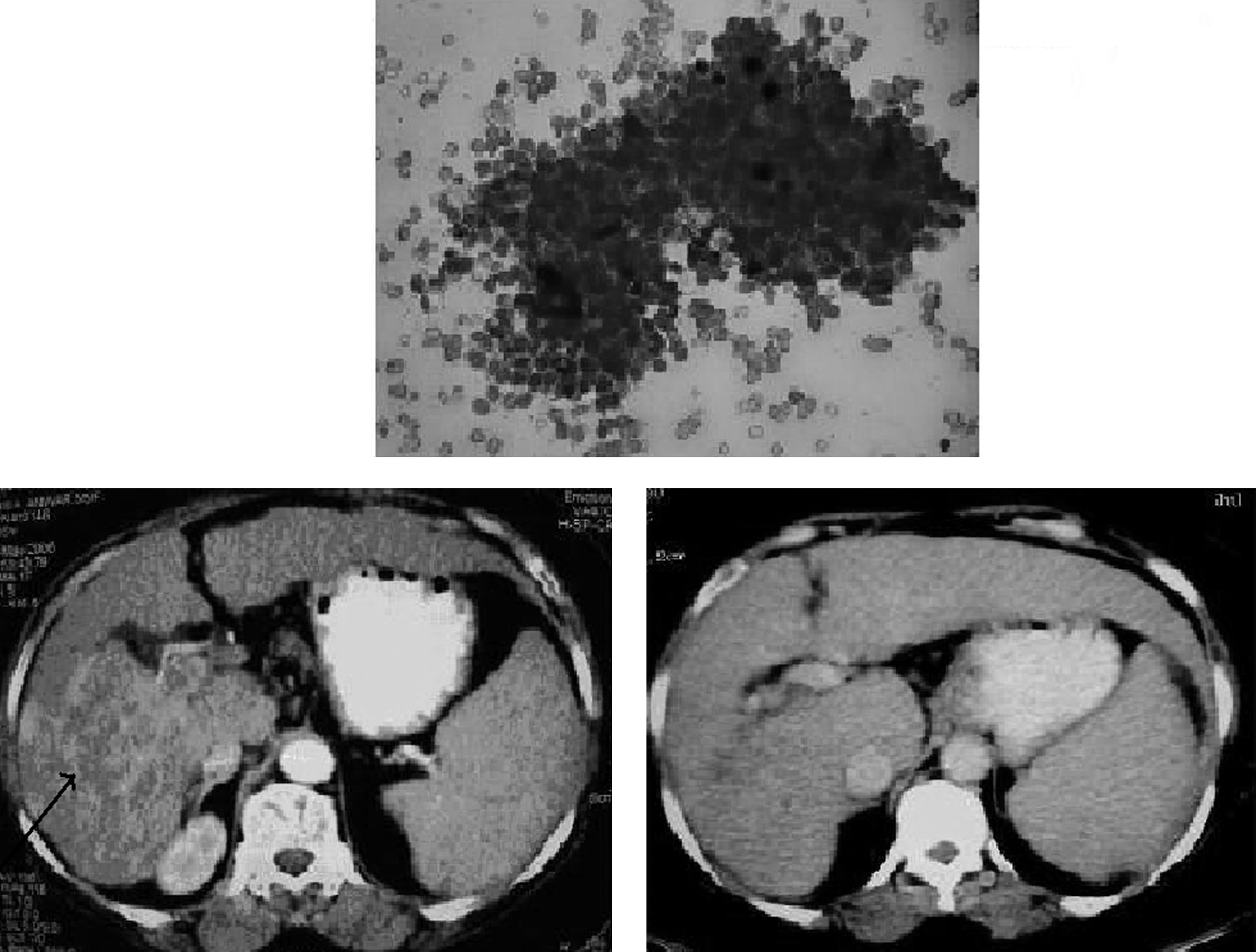
Case 3. Hepatocellular carcinoma (HCC).
Discussion
The three cases that have been discussed here are among the very few well-documented cases involving complementary and alternative medicine (CAM) therapies in treating advanced malignancies that have resulted in complete or partial tumor regression. 26 –28 All 3 patients reported no side effects from Psorinum 6x. It should be noted that these are not the only cases of Psorinum Therapy that had been successfully treated at this clinic, but these are among the well-documented cases where the pathological slides were verified by an independent pathologist of an external institution in order to reconfirm the diagnosis of cancer, and the radiological films were verified by an independent radiologist of an external institution in order to reconfirm the radiologic tumor response. Dr. Arpita Bhakta who is attached to the Department of Microbiology and Pathology of AMRI, Kolkata, India verified the pathological slides of these three cases. Dr. Anup Sadhu, who is at the Department of Radiology of Echo Diagnostic Centre, Kolkata, India, verified the radiological films of these three cases. Impressive clinical evidence is also available in peer-reviewed medical literatures regarding the efficacy of Psorinum therapy in treating various malignancies. A phase II, single-arm clinical trial was conducted to evaluate the efficacy of this alternative cancer treatment in treating patients with stomach, gallbladder, pancreatic, and liver cancers. 14,29 The primary outcome measures of the study were to evaluate the radiological tumor response rates and overall 5-year survival rates.
One hundred and fifty-eight (158) pathologically confirmed participants (42 of stomach, 40 of gallbladder, 44 of pancreas and 32 of liver cancers) were included in the final analysis at the end of the study. Those participants received the drug Psorinum-6x at 0.02 mL/kg body weight/day along with allopathic and homeopathic supportive care. They did not undergo any other conventional or investigational cancer therapeutics. Among them, complete tumor response occurred in 28 (17.72%) and partial tumor response occurred in 56 (35.44%) cases; 62 of them survived for at least 5 years. Another clinical trial was conducted to evaluate the efficacy of Psorinum therapy in treating non-small-cell lung carcinoma (NSCLC). 30,31 Ninety-five (95) pathologically confirmed NSCLC participants were included in the final analysis at the end of that study. Among them, complete tumor response occurred in 19 (20%) cases and partial tumor response occurred in 28 (29.47%) cases; 42 (44.21%) of them survived for at least 5 years. In both of the clinical trials, daily oral administration of Psorinum-6x at doses up to 0.02 mL/kg body weight for 2 years resulted in no adverse side-effects.
Conclusions
A retrospective clinical study on Psorinum therapy in treating 245 participants with oral, lung, liver gallbladder, pancreatic, and stomach cancers advocate in favor of this alternative cancer treatment. 24 An interview-based study was conducted on 300 biopsy-proven cancer patients of Psorinum therapy. The primary purpose of the study was to ascertain the patients' and/or their caregivers' views on this CAM therapy. The survey showed that the patients had tried Psorinum therapy mainly due to no other available treatment options, financial constraints, frustration with the conventional cancer treatments, and belief in the efficacy of the Psorinum therapy. According to the survey, among the 300 patients with cancer, 195 (65%) had consulted their oncologists before trying the therapy. 17 The limitation of this study is that the effects of the implemented allopathic and homeopathic supportive measures in the observed results cannot be ruled out. However, the strength of the study lies in the meticulous documentation of these 3 cases. This article provides potential information for the health care professional who wishes to evaluate and integrate these therapies into present patient-care protocols. It is imperative that this potential be further evaluated and confirmed through well-designed clinical trials. Equally important is the more thorough basic research in the future that will aim at elucidating the cellular and molecular mechanisms by which the drug works against cancer.
Footnotes
Acknowledgments
We acknowledge Dr. Arpita Bhakta, associated with the Department of Microbiology and Pathology, AMRI, Kolkata, India for reviewing the pathological slides of these three cases; and Dr. Anup Sadhu associated with the Department of Radiology, Echo Diagnostic Centre, Kolkata, India for reviewing the radiological films of these three cases. Dr. Sudin Bhattacharya of CNCI, India and Dr. Mikael Nordfors of Humlegarrden, Denmark are acknowledged for their suggestions in writing the article.
Disclosure Statement
No financial conflicts exist.