
Abstract
Objectives:
Controversy exists regarding the efficacy of ligament prolotherapy in alleviating sacroiliac joint pain. The inconsistent success rates reported in previous studies may be attributed to variability in patient selection and techniques between studies. It was hypothesized that intra-articular prolotherapy for patients with a positive response to diagnostic block may mitigate the drawbacks of ligament prolotherapy. The purpose of this study was to evaluate the efficacy and long-term effectiveness of intra-articular prolotherapy in relieving sacroiliac joint pain, compared with intra-articular steroid injection.
Design:
This was a prospective, randomized, controlled trial.
Settings/location:
The study was conducted at an outpatient pain medicine clinic at Chonnam National University Hospital in Gwang-ju, Korea.
Subjects:
The study included patients with sacroiliac joint pain, confirmed by ≥50% improvement in response to local anesthetic block, lasting 3 months or longer, and who failed medical treatment.
Interventions:
The treatment involved intra-articular dextrose water prolotherapy or triamcinolone acetonide injection using fluoroscopic guidance, with a biweekly schedule and maximum of three injections.
Outcome measures:
Pain and disability scores were assessed at baseline, 2 weeks, and monthly after completion of treatment.
Results:
The numbers of recruited patients were 23 and 25 for the prolotherapy and steroid groups, respectively. The pain and disability scores were significantly improved from baseline in both groups at the 2-week follow-up, with no significant difference between them. The cumulative incidence of ≥50% pain relief at 15 months was 58.7% (95% confidence interval [CI] 37.9%–79.5%) in the prolotherapy group and 10.2% (95% CI 6.7%–27.1%) in the steroid group, as determined by Kaplan-Meier analysis; there was a statistically significant difference between the groups (log-rank p < 0.005).
Conclusions:
Intra-articular prolotherapy provided significant relief of sacroiliac joint pain, and its effects lasted longer than those of steroid injections. Further studies are needed to confirm the safety of the procedure and to validate an appropriate injection protocol.
Introduction
To relieve SI joint pain, several techniques have been reported. Among them, intra-articular corticosteroid injection can be helpful, but some patients gain only short-term benefits. 4,5 Radiofrequency (RF) denervation of the SI joint can be an effective treatment, but the exact details of the joint's innervation are unclear, and reported success rates are inconsistent. 6,7
Prolotherapy may also be efficacious for SI joint pain, 5,8 but questions regarding its benefits have also been raised. 9 The inconsistent results of ligament prolotherapy may be explained by the variability in techniques and patient selection, as well as pain emanating from inaccessible ventral structures. 3,8,10
We hypothesized that diagnostic SI joint block may guide patient selection for prolotherapy. Thereafter, a modified intra-articular technique of prolotherapy may compensate for the weaknesses of the conventional periligamentous injection, thus improving the efficacy of prolotherapy in ameliorating SI joint pain. However, to date, there has been no published study examining the efficacy and benefits of sacroiliac intra-articular prolotherapy. The purposes of this study were to assess the efficacy of intra-articular prolotherapy in relieving SI joint pain, using dextrose water, and to evaluate the long-term effectiveness of this technique versus intra-articular steroid injections.
Materials and Methods
This study was approved by the institutional review board of Chonnam National University Hospital. Initial diagnosis was based on a history of pain lasting 2 months or longer in the buttock, groin, or thigh, regardless of associated lower extremity symptoms. Positive physical examination included tenderness over the area just below the posterior superior iliac spine, the Patrick test, or Gaenslen's test. Because these tests lack specificity, 11 a diagnostic local anesthetic intra-articular injection using 2.5 mL of 0.25% levobupivacaine was performed to confirm SI joint pain. A decrease in pain intensity of at least 50%, measured by the numeric rating scale (NRS, 0 = no pain, 10 = maximum pain), was deemed a positive response. Patients diagnosed with SI joint pain and who failed medical treatment for an additional 1 month were prospectively enrolled. Exclusion criteria were cancer, fractures, inflammatory arthritis, infection, unresolved litigation or workers' compensation claims, fibromyalgia, and pregnancy.
After informed consent was obtained, the patients were randomly assigned to receive intra-articular prolotherapy or intra-articular steroid injection according to a computer-generated randomization schedule. Patients and the outcome-measuring physicians were blinded to the treatment group throughout the study. The therapeutic injection was done by a different physician who was not otherwise involved in the study and not blinded to the treatment group. For the prolotherapy group, we injected 2.5 mL of 25% dextrose solution into the SI joint every other week and repeated this up to three times. The dextrose solution was prepared by diluting 50% dextrose water with 0.25% levobupivacaine. If a patient's symptoms were improved by more than 90% by NRS on the second or third visit, the next procedure was canceled. A similar treatment schedule was administered in the steroid group, but the injected drug was triamcinolone acetonide 40 mg (Triamcinolone,® Dong Kwang Pharm, Seoul, Korea) in 0.125% levobupivacaine 2.5 mL (Chirocaine,® Abbott Korea, Seoul, Korea). For managing postprocedure pain, an oral tramadol and acetaminophen combination tablet (Ultracet,® Janssen Korea Ltd, Seoul, Korea) and tizanidine hydrochloride were prescribed for 7 days to all patients. Analgesics being administered before the study were stopped prior to the first session and for the duration of the study. However, adequate medications were provided for patients with recurring severe SI joint pain.
SI joint intra-articular injection
SI joint injection was conducted using fluoroscopic guidance, as described below. Patients were positioned prone, with the C-arm slightly tilted cephalad, to displace the posteroinferior portion of the SI joint inferiorly from the anterior aspect. 12 Then, the C-arm was orbited back and forth such that the medial joint line (the posterior portion of SI joint) and the edge of the sacrum are clearly identified. 13 After the skin was draped and anesthetized slightly caudal to the most inferior aspect of the SI joint, a 22-gauge spinal needle was inserted into the joint. Then, the needle was advanced upward into the base of the joint while being checked for the depth of the tip on the lateral fluoroscopic view. After confirmation of the intra-articular position using an arthrogram, with 0.2–0.5 mL of contrast medium, the drug for diagnosis or therapy was injected. All procedures were performed in an outpatient setting by a specialist in interventional pain management certified by The Korean Pain Society; this specialist had over 5 years' experience as a pain physician (WMK).
Outcome measures
For assessment, a physician unaware of the patient's study group recorded the NRS for pain and the Oswestry disability index (ODI) before and 2 weeks after the completion of a series of treatment. The main outcome measure was the cumulative incidence of sustained pain relief, defined as maintenance of a 50% or more improvement in NRS from baseline, without analgesic medication, at the monthly follow-up session.
Sample size calculation
The sample size calculation was based on the main outcome measure. We assumed that the incidence of sustained pain relief of the prolotherapy group was approximately 0.65 and that of the steroid group was 0.35, according to the report of Chakraverty and Dias, 5 in which the demographics of the populations and the standards used for the diagnosis of SI joint pain were relatively consistent with our pilot study. Thus, a sample size of 45 in each group was determined using Freedman's sample size table 14 for detecting an improvement in survival rate of 0.3, over a baseline value of 0.35, to achieve a statistical power of 80% at a two-sided significance level of 0.05.
Interim analysis
To assess the efficacy of the two treatment methods, an interim analysis was conducted 12 months after starting the recruitment of the patients. From February 2008 to January 2009, 23 and 25 patients were recruited for the prolotherapy and steroid groups, respectively. The interim analysis revealed a significantly higher incidence of sustained pain relief in the prolotherapy group (log-rank p < 0.005). Thus, further recruitment of patients was terminated, but follow-ups were continued on the participating patients for an additional 3 months (Fig. 1).

Flow diagram of participants in the study. Tx, treatment; SI, sacroiliac.
Statistical analyses
Continuous variables were compared between groups using an unpaired t-test and are expressed as means ±standard deviation. Categorical data were analyzed using Fisher exact test, and are reported as percentages. Within-group comparison of the NRS and ODI, before and after treatment, were conducted using the paired t test. Kaplan-Meier survival analysis with the log-rank test was performed to compare the cumulative incidence of sustained pain relief between the two groups. All analyses were performed using SPSS software (version 17.0; SPSS Inc., Chicago, IL). P values of <0.05 were deemed to indicate statistical significance.
Results
Baseline demographics
A total of 50 patients enrolled; 24 were assigned to the prolotherapy group and 26 were to the steroid group. One (1) subject in the prolotherapy group refused further intervention after the second treatment session due to postinjection soreness lasting 7 days and received oral opioid analgesics to relieve her SI joint pain. The other 1 in the steroid group was lost to follow-up at 1 month after completion of treatment. Thus, the remaining 48 patients were followed until recurrence of SI joint pain or the end of the study.
The baseline demographic data of the two groups were comparable and are presented in Table 1. There was no significant difference in the duration of symptoms, pretreatment medication, or baseline NRS and ODI between the groups. The number of injections in the steroid group was significantly lower than that in the prolotherapy group (p < 0.01). One (1) or two injections was sufficient to achieve pain relief ≥90% from baseline for the 22 patients (88%) in the steroid group, whereas three injections were needed for the 16 patients (70%) in the prolotherapy group (Table 2).
SD, standard deviation; NSAIDs, nonsteroidal anti-inflammatory drugs; NRS, numeric rating scale; ODI, Oswestry disability index.
p < 0.01, versus prolotherapy group.
Not applicable, because above 50% of subjects in this group remained improved >50% from baseline at the time of the study end.
NRS, numeric rating scale; SD, standard deviation; CI, confidence interval; ODI, Oswestry disability index.
Effectiveness at 2 weeks' follow-up
The NRS was significantly decreased from baseline in both groups at 2 weeks after the completion of the treatment series, from 6.3 ± 1.1 to 1.4 ± 1.1 for the prolotherapy group and from 6.7 ± 1.0 to 1.9 ± 0.9 for the steroid group (p < 0.001). At that time, all patients in both groups experienced ≥50% reduction in pain. In addition, the ODI score was significantly improved from the pretreatment value, 33.9 ± 15.5 to 11.1 ± 10.0 for the prolotherapy group and from 35.7 ± 20.4 to 15.5 ± 10.7 for the steroid groups (p < 0.001). There was no significant difference between the two groups with regard to the post-treatment NRS or ODI (Fig. 2). Transient aggravation of pain lasting several days was reported in some patients without significant difference between groups. None of the participants reported serious adverse event such as long-lasting exacerbation of pain, numbness or weakness, or signs of skin infection.
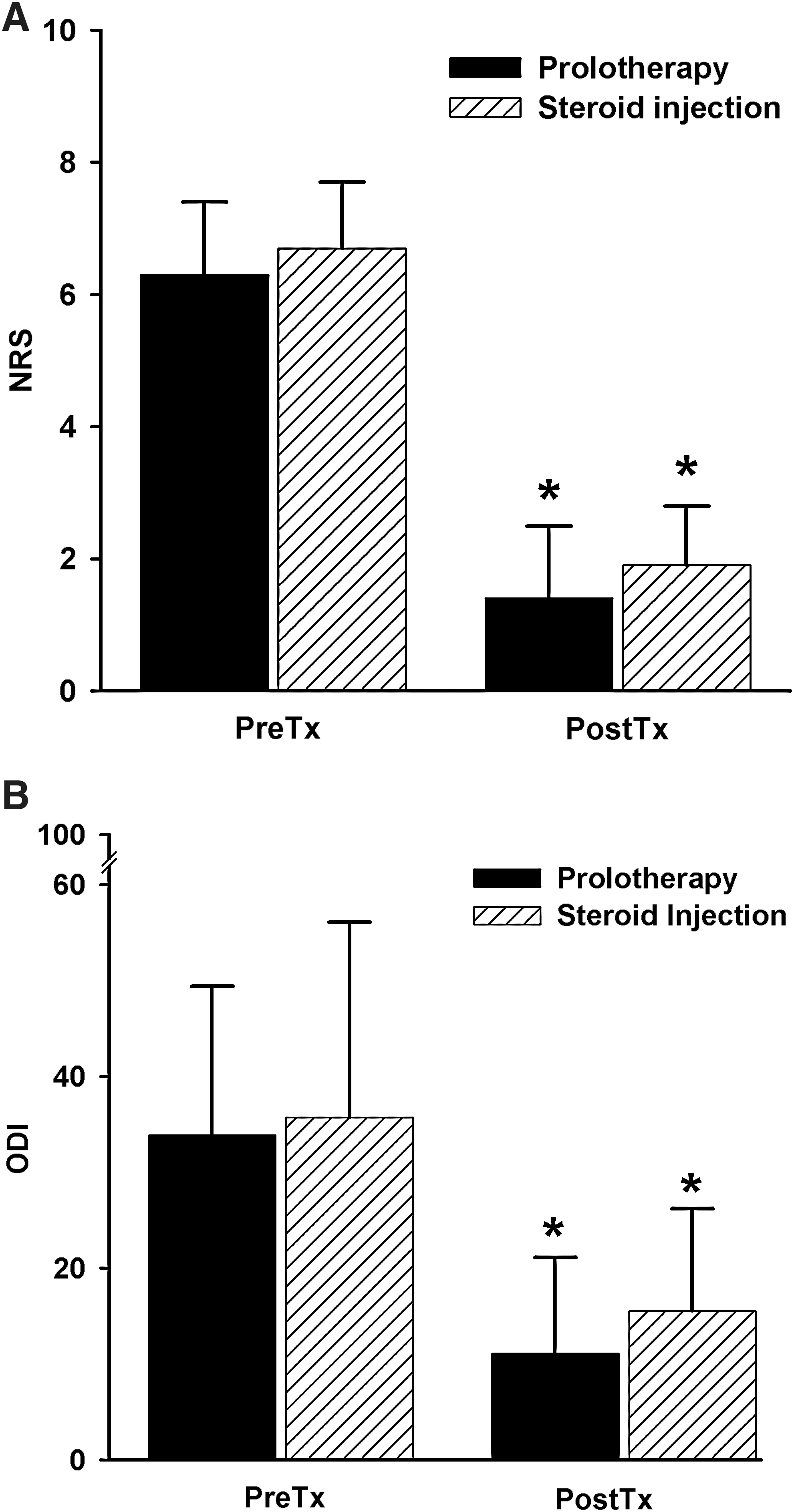
Numeric rating scale (NRS)
Long-term follow-up data
At 6 months after treatment, 63.6% of patients in the prolotherapy group remained 50% or more improved from baseline, whereas it was 27.2% in the steroid group (Table 2). The cumulative incidence of sustained pain relief at 15 months was 58.7% (95% confidence interval [CI] 37.9%–79.5%) in the prolotherapy group and 10.2% (95% CI 6.7%–27.1%) in the steroid group (Table 2); there was a significant difference between the two survival curves (p < 0.005; Fig. 3). No serious complication was reported during the follow-up period.
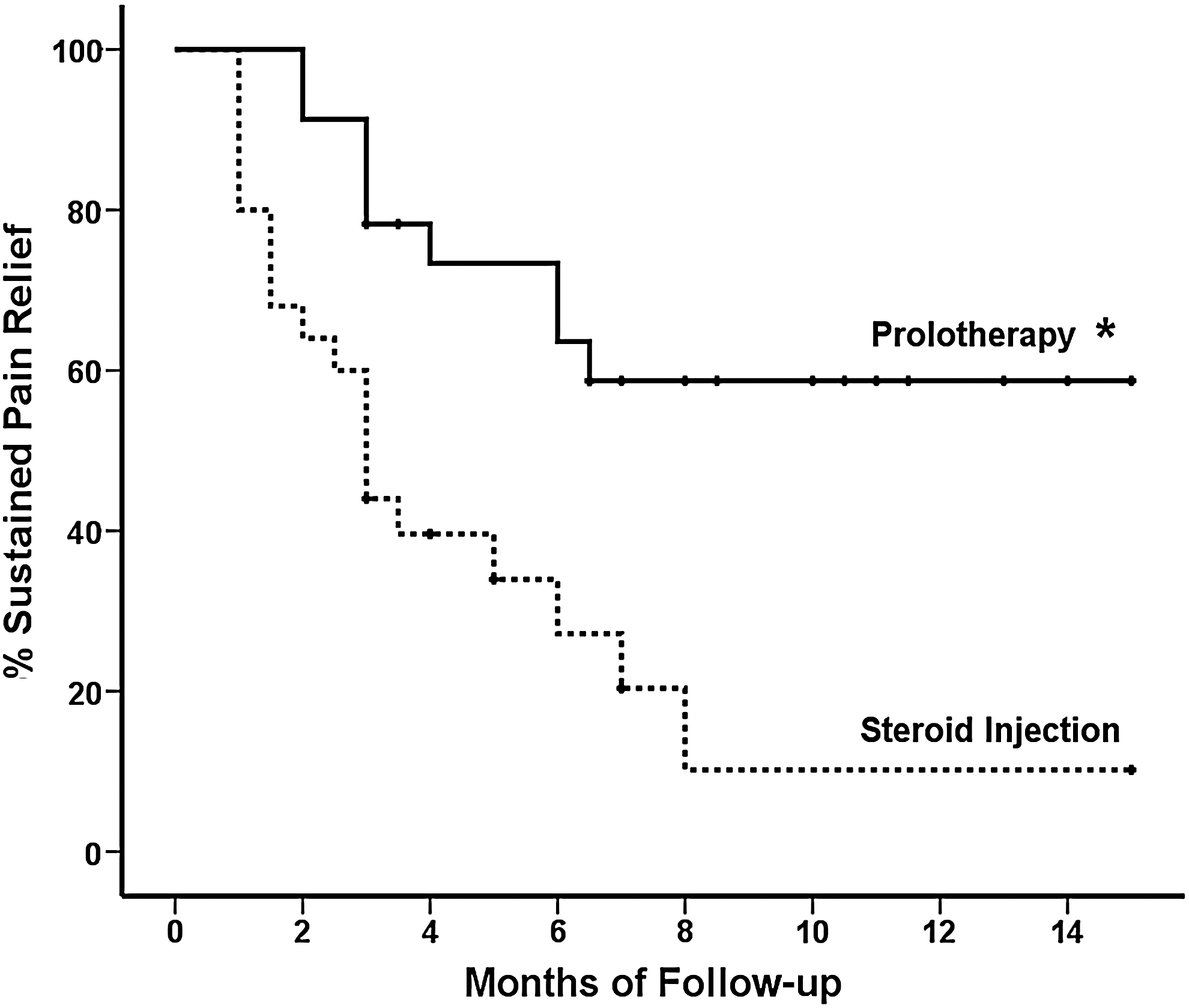
Kaplan-Meier plot showing cumulative incidence of sustained 50% or greater relief of pain, which was significantly higher in the prolotherapy group compared with the steroid group, as analyzed by log-rank test. *p < 0.005, versus steroid injection group.
Discussion
In this study, intra-articular prolotherapy provided significant relief from SI joint pain, and its effect lasted longer than that of steroid injections. Key findings of this study are a patient-selection method for prolotherapy using a diagnostic SI joint block and the proliferant injection technique using a reproducible arthrogram.
Although various methods have been suggested to relieve SI joint pain, we suggest that intra-articular prolotherapy, as documented in this study, may have advantages over other techniques, such as periligamentous prolotherapy, RF denervation, and steroid injection. First, this method may reduce variability in patient selection and in the injection technique used in prolotherapy. In the systematic review of Yelland et al., there was no evidence that prolotherapy injections alone were more effective than control injections. 15 However, these findings may be attributable to the lack of a specific diagnosis for patient selection and variations in the proliferant injection technique. Cusi et al. pointed out the importance of patient selection and treatment protocol, noting that there was no evidence that the proliferation of soft tissue was analgesic per se. 8 That is, the results of prolotherapy for SI joint pain are likely to vary, depending on the experience and skill of the practicing physician. Patient selection in this study was based on a specific procedure that has been suggested as the “gold standard” for diagnosing SI joint pain, 16 and the injection method was not a blind technique, but a fluoroscopically guided, reproducible one, thus reducing variability in patient selection and injection technique. As a result, these advantages of the intra-articular prolotherapy technique may have led to the favorable results reported here.
Second, intra-articular prolotherapy may provide some beneficial effects on the ventral structures of the SI joint. Schwarzer et al. 3 reported that ventral capsular pathology was shown to account for 69% of all computed tomography (CT) pathology in patients with positive responses to diagnostic block. However, these are inaccessible to ligament prolotherapy or RF denervation.
Finally, there is a need for a repeated needle puncture technique into multiple sites for ligament prolotherapy 17 or RF denervation, 6 in contrast to intra-articular prolotherapy, which uses theoretically a single injection for each session, thus minimizing patient discomfort during the procedure.
The rationale for prolotherapy is that it may produce dense fibrous tissue to strengthen the attachment of ligaments, tendons, joint capsules, and other fascial structures at their fibro-osseous junctions. 18 Prolotherapy is the injection of an irritant proliferant solution into the abovementioned structures. However, the concept of intra-articular dextrose prolotherapy has also been reported. In a study by Hooper et al., 19 intra-articular zygapophysial joint prolotherapy using 0.5–1 mL of dextrose solution improved pain and function in patients with chronic whiplash. Reeves et al. 20,21 reported that intra-articular dextrose prolotherapy resulted in clinically and statistically significant improvements in knee osteoarthritis, with or without anterior cruciate ligament laxity, at the 1- and 3-year follow-up. There was consideration that sacroiliac intra-articular prolotherapy might also work, based on the absent or rudimentary posterior capsule, 22 which may allow spreading of the injected drug, allowing it to reach the dorsal SI ligamentous structures. Moreover, taking into account the significance of ventral capsular pathology, 3 it was hypothesized that intra-articular prolotherapy would be more efficacious than a periligamentous injection.
The cumulative incidence of sustained pain relief in response to steroid injection in this study was 27.2% and 10.2% at 6 and 15 months, respectively, and the median duration of survival to recurrence of severe SI joint pain was 3 months, which is rather low or short, compared with other reports. 23,24 The long-term effectiveness of SI joint steroid injection has been reported, with the proportion of subjects with sustained pain relief at 6 months being 58%, 23 or the average duration of sufficient pain relief being 9.3 months. 24 However, the former was assessed in patients with spondyloarthropathy in which the inflammatory component could have been more important than the mechanical one, and the latter was determined by the time between injections, which may have overstated the duration of the response. Additionally, different definitions of a positive response to a diagnostic block can affect the sensitivity of the diagnostic block, which may in turn affect the success rate of the therapeutic injection. Diversity in the demographics of the study population and the duration of follow-up between studies may also explain the different results reported.
The results of this study indicated that intra-articular prolotherapy may be useful as a treatment modality for SI joint pain. However, this study also has some limitations. There was a need for more frequent intervention by intra-articular prolotherapy than by steroid injections to achieve pain relief of ≥90% from baseline, indicating that the therapeutic effect of the former may appear later than the latter. However, from the viewpoint of long-term effectiveness, intra-articular prolotherapy may provide adequate pain relief with less frequent intervention than steroid injections. Further investigations are necessary to evaluate the long-term safety of repeated intra-articular injection of dextrose water and the adequacy of the volume and number of injections, although no patient here reported a serious adverse event.
Conclusions
Intra-articular prolotherapy with 5% dextrose water may be useful for the long-term relief of SI joint pain. Further studies are needed to confirm the safety of the procedure and to validate an appropriate injection protocol.
Footnotes
Acknowledgments
No financial support was provided for this study.
Disclosure Statement
No competing financial interests exist.