
Abstract
Objectives:
The purpose of this study is to assess the effect of manual acupuncture on experimental pain parameters in healthy participants.
Design:
The experimental design was a repeated-measures, three-group pre- and postprocedure. All subjects participated in a control, sham, and acupuncture procedure, separated by 1 week, in a counterbalanced sequence to forestall an order effect.
Settings/location:
Data were collected in a laboratory environment.
Subjects:
The participants included 12 healthy young men (mean age 21.3 ± 2.6 years; height 183.8 ± 5 cm; weight 77.7 ± 9.5 kg).
Interventions:
The control procedure comprised assessing the experimental pain parameters before and after a quiet rest for 20 minutes. The sham procedure was performed with the needle inserted bilaterally 1–1.5 cm outside each acupoint. The manual acupuncture procedure was performed at two bilateral acupoints of LI–4 (Large Intestine 4, Hegu) and ST-44 (Stomach 44, Nei Ting).
Outcome measures:
Pain parameters assessed included the pain threshold, nociceptive reflex threshold, and nociceptive reflex amplitude.
Results:
Repeated-measures analysis of variance between pre- and postcontrol, sham, and acupuncture procedures for pain threshold, nociceptive reflex threshold, and nociceptive reflex amplitude revealed no significant difference.
Conclusions:
Manual acupuncture at bilateral acupoints LI–4 and ST–44 did not show a change in pain threshold, nociceptive flexion reflex threshold, or the nociceptive reflex amplitude in healthy participants.
Introduction
Previous studies on manual acupuncture for the inhibition of experimental pain in healthy participants have revealed inconsistent results. The manual acupuncture procedure was observed to inhibit pain in different regions of the body based on the acupoints applied. 5 An increase in pain threshold following manual acupuncture was observed intrasegmentally compared to sham procedure. 6 Manual acupuncture has been shown to increase the dental pain threshold compared to a control group of healthy participants. 4,7 In a study on experimental thermal pain, the noxious thermal pain ratings were reduced in 3 of 11 participants following manual acupuncture. 8 In the results, 2 participants responded only to electro-acupuncture and not to manual acupuncture. Furthermore, the study reported that the reduced thermal pain response following acupuncture varied with the type of treatment (electro or manual acupuncture) and that many participants did not respond to any type of acupuncture treatment. In another study on cold pain threshold and hot pain threshold following manual acupuncture, the results showed no difference in thresholds compared to control or sham procedure. 9 Sharp pain threshold was increased to levels above a sham procedure; however, 2 participants did not respond to manual acupuncture. 10
The neuropathways for the attenuation of pain by manual needle acupuncture are uncertain. 11 In the experimental setting, pain inhibition by spinal segmental mechanisms is induced by the activation of low-threshold afferents and is the neuronal basis of gate control theory. 12 Intense painful stimuli can also activate a wide systemic nonsegmental inhibition of pain, which is the basis for diffuse noxious inhibitory controls. 13 It has been proposed that acupuncture may attenuate nociceptive transmission through the spinal cord by the activation of low-threshold afferents and may also dampen central pain perception in the brain by launching diffuse noxious inhibitory controls. 14
The transmission of nociceptive stimuli through the spinal cord from electrocutaneous stimulation is experimentally assessed by the nociceptive flexion reflex (NFR). 15 The threshold for the NFR is a reliable neurological assessment of the experimental pain threshold. 16 Previous research has shown that an electroacupuncture procedure inhibits pain report and the NFR at homotopic and heterotopic acupoints. 11 Currently, there is a paucity of data that show the effect of manual acupuncture on pain-related nociceptive reflex events in healthy participants. Therefore, the purpose of this study was to assess the responses of the NFR and pain threshold following manual acupuncture in healthy young participants.
Materials and Methods
Participants
The participants included 12 healthy young men (mean age 21.3 ± 2.6 years; height 183.8 ± 5 cm; weight 77.7 ± 9.5 kg) with no previous experience with a manual acupuncture procedure. Participants were screened with a health questionnaire and a physical activity profile. The exclusion criteria included the acute use of analgesics and anti-inflammatory medications, prior history of leg/knee injury or surgery, and acute/chronic disease. The study was conducted with the approval of the Charles Sturt University Ethics in Human Research Committee (approval number 2009/001), and each subject signed a letter of informed consent. The participants attended the laboratory on three separate occasions, and at the same time of day. All participants were unfamiliar with manual acupuncture; however, one participant included in the study had a previous shoulder injury treated by electro-acupuncture. Each participant was requested to perform their regular daily activities for the duration of the study.
Study design
The experimental design was a pre and post three-group repeated-measures procedure. Each subject participated in a control, sham, and acupuncture procedure and was randomly assigned by the corresponding author in a counterbalanced sequence to avert an order effect. The control procedure was applied in the design to assess the effect of repeated application of experimental pain stimuli on the pain threshold 17 and the NFR. Participants were blinded to whether the acupuncture or sham procedure was performed. Each session required the assessment of the NFR threshold and pain threshold before and 20 minutes after the acupuncture procedure, sham procedure, and control procedure. Each session was 1 hour in duration and separated by 1 week. Recruitment of participants was performed over 4 weeks and data collection was performed over 8 weeks.
Participant preparation
Participants were supine in the anatomical position with the hands pronated on a padded therapeutic table (Metron, Carrum Downs, VIC) throughout the session. The placement of electrodes required verifying the dominant leg, identifying the anatomical site for electrode placement, and dermal preparation for each electrode site. The electrocutaneous stimulation site was located between the lateral malleolus of the fibula and the tendo Achillis, on the retromalleolar pathway of the sural nerve. The electromyographic (EMG) recording site was on the biceps femoris long head muscle. This was located by identifying the biceps femoris tendon insertion on the lateral aspect of the popliteal space and measuring one third of the distance to the ischial tuberosity toward the midgluteal fold. The reference electrode site was located on the lateral malleolus of the contralateral fibula. The electrode sites were prepared by shaving, dermal abrasion, and degreased with ethanol solution.
Two (2) disposable (Ag/AgCl) adhesive press-stud electrodes (Meditrace, Chicopee; 30-mm diameter with 22-mm-diameter electrogel contact surface area) were applied at the electrostimulation site and EMG site. The electrodes were vertically aligned 30 mm apart from the center of the disc, separated by the rim of the adhesive disk. The cathode was connected inferior to the anode electrode. A single adhesive (Ag/AgCl) disposable press-stud electrode was positioned at the reference site following dermal preparation, on the contralateral malleolus of the fibula. The electrodes remained in position for the session. A 10-second baseline EMG signal was recorded when participants were comfortably settled.
NFR and pain threshold assessment
The NFR threshold and pain threshold were determined by a modified staircase method. 15 This procedure requires delivering a set of five 20-V electrostimuli at random intervals of 5–15 seconds apart. The five stimuli each comprised a volley of eight 1-millisecond rectangular pulses with an interspike interval of 2 milliseconds and delivered over 22 milliseconds. Following each set of five electrostimuli, participants were requested to verbally rate the intensity of the sensation using a 0–10 category scale. The numerical anchors and verbal descriptors were graded as 0 = no sensation, 2 = slight sensation, 4 = moderate sensation, 6 = pain sensation, 8 = strong pain sensation, and 10 = pain tolerance. Participants were informed that a rating of 6 on the category scale represented the point at which the sensation was no longer tactile and was painful. A rating of 6 represented the pain threshold.
Following the first set of five 20-V electrostimuli and sensation scale rating, each subsequent set was increased by 20 V. The 20-V increments continued until the NFR threshold and pain threshold were determined, or an upper limit of 7 on the sensation scale was observed. The threshold for the NFR was defined by (1) a nociceptive reflex signal amplitude from biceps femoris muscle of at least 1.65 standard deviations (SDs) of the mean baseline resting EMG activity, 18 (2) the voltage intensity that evoked at least three NFRs from a set of five electrocutaneous stimuli, 19 and (3) a poststimulus reflex signal within a 90–150-millisecond time frame. 20 A signal latency window of 90–150 milliseconds is often applied in NFR research to preclude signal contamination by non-nociceptive reflexes, startle, and/or voluntary responses. 21 Upon the initial observation of the NFR, a decrement of 10 V was applied to assess the consistency of the NFR signal at reduced electrocutaneous intensity. This procedure differs slightly from the up–down staircase method for measuring the NFR threshold; however, this minimizes pain-induced stress. 19
Acupuncture, sham, and control procedure
The manual acupuncture procedure required a fine-needle insertion at two bilateral acupoints located intrasegmentally and extrasegmentally from the experimental pain stimulus. The intrasegmental site was ST-44 (Stomach 44, Nei Ting), located on the dorsum of the foot at the proximal end of the web between the second and third digits. The extrasegmental site was LI-4 (Large Intestine 4, Hegu), located on the dorsum of the hand at the midpoint of the second metacarpal bone in the belly of the first interosseus dorsalis muscle. Following skin cleansing by alcohol swab, a disposable needle (Viva, Helio Medical Supplies, San Jose, CA) was inserted at each acupoint by a qualified practicing acupuncturist to a depth of 10–30 mm transversely through the dermis. The de qi was elicited following the needling insertion at each acupoint. The acupuncture needles and the sham needles remained inserted in each point for 20 minutes, after which the NFR and pain threshold were reassessed.
The sham procedure required an acupuncture needle inserted bilaterally 1–1.5 cm outside each acupoint. The purpose of the sham procedure was to assess the potential effect of needle insertion at nonacupoints on pain parameters. The sham needles remained inserted for 20 minutes. The pain parameters of pain threshold, NFR threshold, and NFR amplitude were assessed before and after the sham needle procedure.
The purpose of the control procedure was to determine the repeated application of experimental pain parameters without the insertion of acupuncture needles. The pain parameters of pain threshold, NFR threshold, and NFR amplitude for the control procedure were assessed before and after a 20-minute rest interval (Fig. 1).
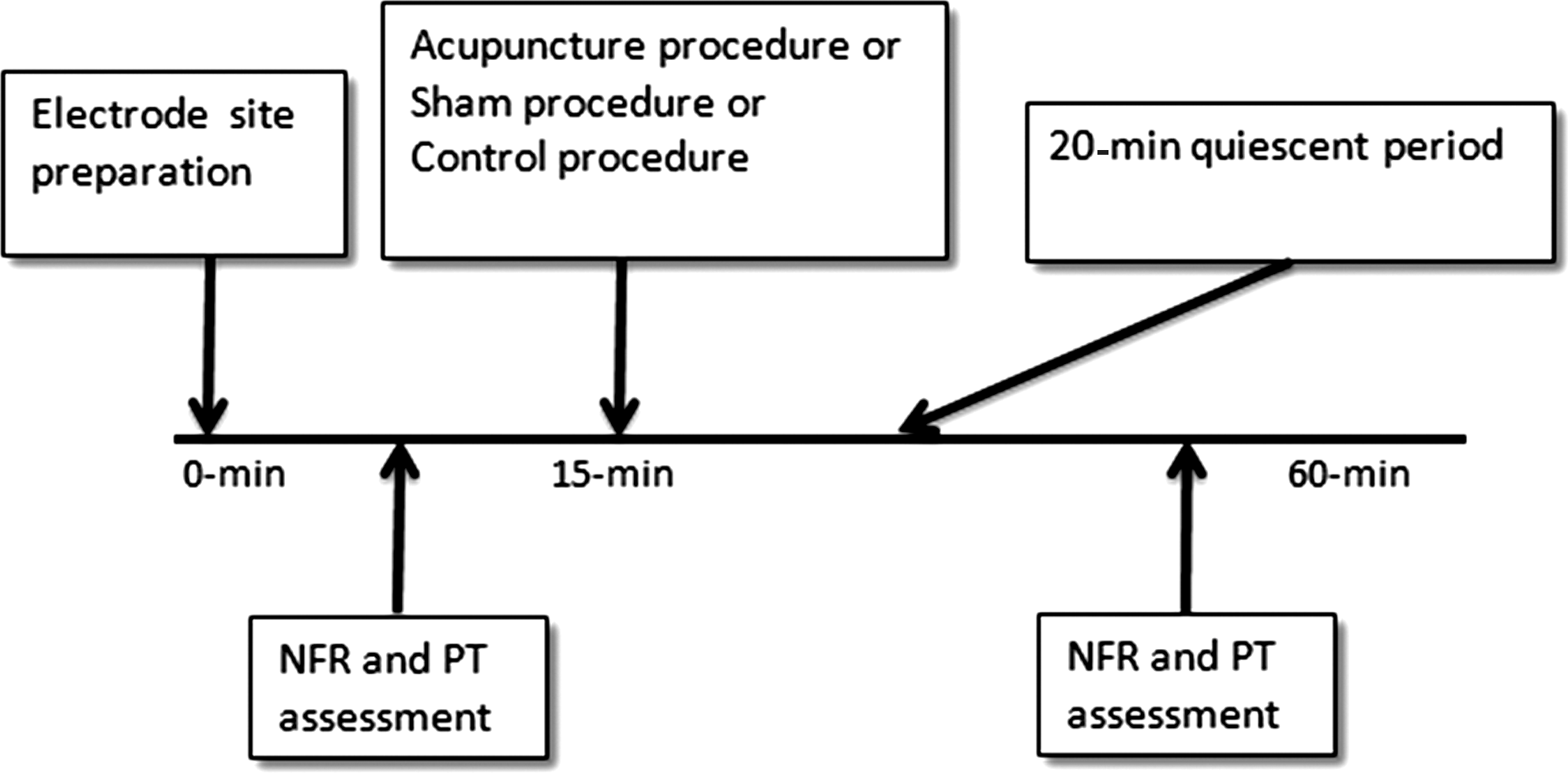
Timeline representing the sequence of events for the assessment of the nociceptive flexion reflex (NFR) and pain threshold (PT) before and after the control procedure, sham procedure, and acupuncture procedure.
Laboratory apparatus
The EMG signal from biceps femoris muscle was digitally sampled at 2000 Hz using an analog-to-digital converter (Amlab, MR01C, Sydney, Australia). The raw EMG activity was low-pass filtered (25 Hz; second-order quasi-butterworth filter with a slope of −40 dB/Decade). Similar filter parameters have been previously applied to assess the NFR signal. 22 The digital sampling procedure simultaneously recorded the onset of electrostimulation and the EMG signal. The electrocutaneous stimuli were delivered by a constant-voltage peripheral nerve stimulator (Digitimer D185 MKIIa, Hertfordshire, UK) connected to a high-grade electrical cable (Digitimer D185-HB4, Hertfordshire, UK).
Signal analysis
The offline signal analysis included the measurement of the amplitude of the NFR signal. The mean NFR signal amplitude was determined from a standard voltage for each participant before and after the acupuncture, sham, and control procedure.
Statistical analysis
Data are presented as mean ± SD. Comparisons between the pre- and post-NFR threshold, pain threshold, and NFR amplitude were assessed by repeated-measures analysis of variance (ANOVA), with significance level set at p < 0.05. The observed power was 1.0.
Results
The mean ± SD for the NFR threshold, the pain threshold, and the NFR amplitude are shown in Figure 2.
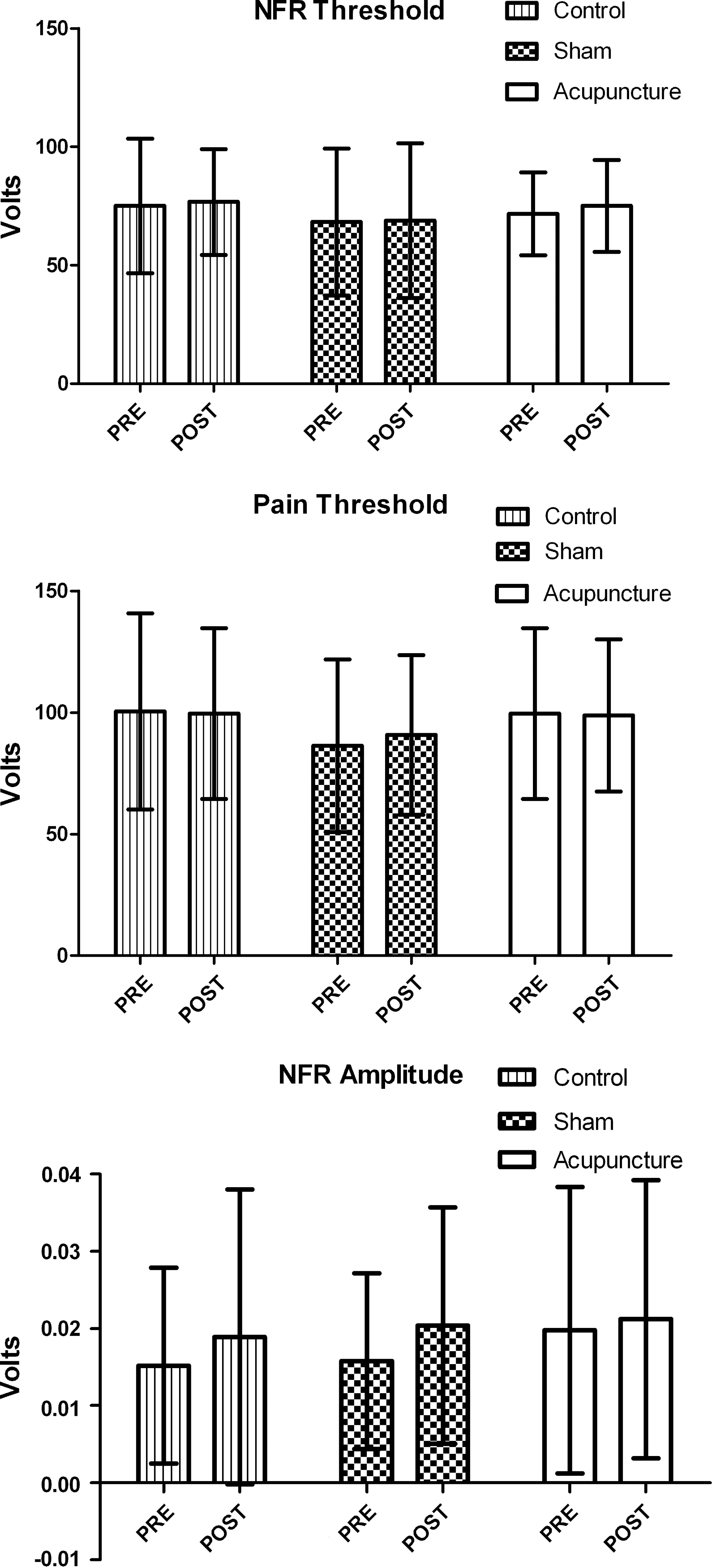
The mean and standard deviation of pre- and postnociceptive flexion reflex (NFR) threshold, pain threshold, and NFR amplitude for control, sham, and acupuncture procedure in healthy participants.
Repeated-measures ANOVA between pre- and postcontrol, sham, and acupuncture procedure for the NFR threshold revealed no significant difference at p = 0.586, p = 0.908, and p = 0.220, respectively.
Repeated-measures ANOVA for pre- and postcontrol, sham, and acupuncture procedure for the pain threshold revealed no significant difference at p = 0.871, p = 0.317, and p = 0.406, respectively.
Repeated-measures ANOVA for pre- and postcontrol, sham, and acupuncture procedure for the nociceptive reflex amplitude revealed no significant difference at p = 0.277, p = 0.243, and p = 0.406, respectively.
Discussion
Early research has shown that acupuncture can increase the experimental pain threshold. 23 The present results show that a single session of manual acupuncture procedure did not increase the pain threshold or the NFR threshold in healthy participants. In addition, manual acupuncture did not show a change in the signal amplitude of the NFR from a repeated electrocutaneous stimulus. Several reasons may explain why the present results did not show a change in the experimental pain parameters following the acupuncture procedure.
Acupuncture is performed using either electroacupuncture or manual needle acupuncture procedures. While previous research has shown mixed results for manual acupuncture in altering experimental pain thresholds, electroacupuncture procedures have revealed more consistent changes in experimental pain parameters. 24 Previous research on electroacupuncture has shown an increase in both the thresholds for pain and the NFR. 11 The electroacupuncture procedure is able to modulate the electrostimulus, whereas manual acupuncture does not have this type of input. Furthermore, the sensation of de qi appears to be qualitatively and quantitatively different between manual and electrical acupuncture procedures. 25 Additional studies comparing the effect of electroacupuncture and manual acupuncture on experimental pain will address this.
Manual needle acupuncture requires different sets of acupoints in the treatment of pain and other conditions. The present study applied a set of bilateral acupoints identified as Large Intestine 4 and Stomach 44. Large Intestine 4 has been previously used in experimental pain research, 26 and Stomach 44 is clinically applied for the treatment of acute pain conditions 27 and in experimental pain research. 4 One early study revealed that manual acupuncture at the Large Intestine 4 acupoint increased the pain threshold. 28 In another study, an increase in the dental pain threshold was observed in a control group of healthy participants using acupoints ST-2 (cheek), LI-4 (hand), and ST-44 (foot). 4 It is possible that differences in the effect of the acupoints applied may explain why manual acupuncture did not alter experimental pain parameters in the present study. The efficacy of alternate acupoints in a manual acupuncture procedure could be investigated further in future studies on experimental pain parameters.
The current study included acupoints that were located at extrasegmental (LI-4, hand) and intrasegmental (ST-44, foot) sites from the experimental pain. It has been previously observed that manual acupuncture increased the pain threshold when the acupoint was applied intrasegmentally. 6 In contrast, the present results did not show an intrasegmental increase in pain threshold or the NFR. One possible reason why the present study did not find an intrasegmental inhibition of experimental pain is that the acupoint was located distally to the nociceptive pathway. Future studies could assess the effect of manual acupuncture on experimental pain by applying acupoints that are positioned along the nociceptive leg flexion reflex pathway such as ST-36.
The number of acupuncture treatments in the present study may also be a plausible reason for the noneffect of manual acupuncture procedure on pain parameters. Acupuncture often requires several treatment sessions. The treatment procedure for chronic low-back pain typically consists of 11 sessions held twice weekly. 29 The present study applied a single-session manual acupuncture procedure on experimental pain and nociceptive thresholds. Moreover, the present study induced the sensation of de qi once during the acupuncture needle insertion. Therefore, it is plausible that several acupuncture sessions with the sensation of de qi may be required to observe changes in experimental pain parameters.
The present study included young healthy participants to assess the effect of manual acupuncture on experimental pain parameters. An acupuncture procedure, however, is more widely accepted as a treatment for persons with short-term and chronic pain conditions. Meridian theory proposes that pain is attributed to a disease-induced blockade of meridian channels that are unblocked by acupuncture therapy. 30 Therefore, it is possible that manual acupuncture procedure is not suitable for detecting changes in experimental pain parameters in healthy participants.
The postacupuncture assessment of pain parameters in the present study was performed at 20 minutes after manual needle acupuncture procedure. The optimum time for assessing experimental pain parameters following acupuncture has been reported to be between 20 and 40 minutes. 31 In one study, the pain threshold was assessed at 45 minutes postacupuncture; however, there was no change in experimental pain parameters. 4 Similarly, no change in pain parameters were observed at 25 minutes postacupuncture. 9 The present study further re-assessed pain parameters at 35 minutes postacupuncture in 6 participants (unpublished data); however, there remained no difference in the pain and nociceptive thresholds. A markedly diminished sharp pain sensation was observed 5 minutes following manual acupuncture of the knee. 32 Future studies would need to measure experimental pain parameters at regular intervals immediately after acupuncture to assess the optimum temporal effect of manual acupuncture.
Conclusions
The present results show that the manual acupuncture procedure did not reveal a change in experimental pain parameters. Manual acupuncture using bilateral acupoints LI-4 and S-44 with de qi sensation performed at needle insertion and with the needles inserted for 20 minutes did not show a change in the pain threshold or the NFR in healthy participants.
Footnotes
Acknowledgments
We are deeply grateful to Lamar Gunter for the acupuncture treatment procedure and to Dr. Eric Drinkwater for advising on the statistical analysis procedures. The study was financially supported by a Charles Sturt University Faculty of Education Small Grant Scheme 2009.
Disclosure Statement
No competing financial interests exist.