
Abstract
Objectives:
This study aims to determine the efficacy and safety of soy isoflavones in controlling the symptoms and signs of lower urinary tract symptoms due to benign prostate hyperplasia (BPH).
Design:
This was a prospective, randomized, double-blind, placebo-controlled pilot study.
Setting:
This trial was conducted at two hospitals in Hong Kong between May 2006 and September 2007.
Participants:
One hundred and seventy-six (176) participants diagnosed with BPH were recruited from outpatient clinics. Participants with lower urinary tract symptoms were recruited through newspaper and radio interviews, posters placed at government outpatient clinics, and a public seminar offered by the investigators.
Interventions:
Participants were randomly assigned to either intervention (40 mg of isoflavones daily from Soylife 40) or placebo groups in a double-blind fashion.
Main outcome measures:
The primary outcome parameter of peak urine flow rate and the second outcome parameters of postresidual urine volume, lower urinary tract symptoms, testosterone, prostate-specific antigen, quality of life, diet, and safety profile (liver and renal function) were collected. All parameters were assessed at baseline, 6 months, and 12 months in a 12-month study period except testosterone, prostate-specific antigen, and safety profile, which were assessed at baseline and at 12 months.
Results:
The peak urine flow rate (Qmax), postresidual urine volume, International Prostate Symptoms Scores (IPSS), and 36-Item Short Form Health Survey (SF-36) significantly improved from baseline to the 12th month within both groups. However, when compared between groups, Qmax (p=0.055) and incomplete emptying subscore in IPSS (p=0.05) were marginally/statistically different between the two groups from the 6th to the 12th months, in addition to the general health domain of SF-36 from the baseline to 12th month (p=0.02) and from the 6th month to the 12th month (p=0.055). Isoflavones were generally safe and well tolerated.
Conclusions:
This randomized control pilot study showed only slight superiority of isoflavones over placebo over 12 months with otherwise surprising beneficial effects in both groups. Tolerability of isoflavones was excellent; thus it has laid foundations for further studies of isoflavones in BPH with focus on dosage and possible specificity of the effect.
Introduction
Among 30 phytotherapeutic compounds available for the treatment of BPH, the extracts of Serenoa repens (American saw palmetto) and Pygeum africanum (African prune tree), β-sitosterol (the extract of South Africa star grass), and Cernilton (the extract of rye-grass pollen Secale cereale) are commonly used. Systematic reviews of randomized controlled trials using these compounds have demonstrated significant clinical effects of varying degrees in reduction in International Prostate Symptoms Scores (IPSS), peak urine flow rate, and/or residual volume, some comparable to α-reductase inhibitors but with fewer undesired effects and at lower costs. They are also generally well tolerated when compared to other prescription medicines. 7 –10 Nonetheless, all reviews warn that their long-term effectiveness and ability to prevent BPH complications are not known.
The two forms of isoflavones, aglycone and glucoside, are commonly used dietary supplements among patients with BPH. 11 These are polyphonic compounds found predominantly in soy food and red clover. Numerous studies have shown that isoflavones have effects on glandular epithelium in the prostate involving 5-α-reductase inhibition and uridine 5-diphospho-glucuronsyltransferase (UDP-glucuronsyltransferase, UGT) activation, and also have effects on stromal cell in the prostate including 17-phydroxysteroid dehydrogenase inhibition, aromatase inhibition, and estrogen-receptor antagonism. 12 –16 Some epidemiological studies also link a low incidence of BPH with a diet rich in isoflavones; for example, Japanese males who had a lower incidence of BPH had high levels of isoflavone phytoestrogens in plasma and urinary excretion, 17 and males from Hong Kong had higher levels of daidzein and a metabolite of daidzein, equol, in their plasma and prostate fluid compared to British and Portuguese men. 18 At the same time, when males from low BPH incident countries migrated to high incident counties and adopted local dietary customs, their risk of BPH rose significantly. 19 One study demonstrated a correlation between high consumption of soy milk and a reduced risk of BPH among Seventh Day Adventist men. 20
Despite the good evidence in both preclinical and epidemiologic studies, no randomized controlled trial has yet been reported to assess the effectiveness of isoflavones among men with benign BPH (i.e., those who chose not to have any active interventions for mild symptoms, or even moderate-to-severe symptoms without complications). The aims of this trial were to determine the safety and efficacy of soy isoflavones in controlling symptoms among this group of patients.
The primary outcome was The uroflowmetry with measuring the peak urine flow rate (Qmax).
The secondary outcomes were: The postresidual urine volume (PVR) The LUTS The quality of life using IPSS Any severe adverse events as a result of treatment.
Materials and Methods
This study was a randomized, double-blinded, placebo-controlled prospective pilot trial. This trial was conducted at Prince of Wales and Shatin Hospitals in Hong Kong between May 2006 and September 2007. Participants with watchful waiting BPH, which is defined as mild LUT symptoms (Qmax <15 mL and PVR ≥150 mL)
21
without complication and medical management required were recruited through newspaper and radio interviews, posters placed at government outpatient clinics, and a public seminar offered by the investigators. The inclusion criteria were the following: Chinese resident living in Hong Kong Age between 45 and 85 years IPSS > 8
23
Not on any concurrent or alternative medications for BPH or α-1 inhibitor (e.g., doxazosin for cardiac reasons) Mentally capable of giving informed written consent and willing to comply with study protocol.
A subject would be excluded for the following: Concurrent treatment for unstable chronic diseases including unstable angina, poorly controlled diabetes mellitus (hemoglobin A1c >7.5%), less than 3 months post–myocardial infarction or frequent exacerbation of chronic obstructive airway diseases •Known to have prostate cancer •Known kidney and/or liver failure •Urinary symptoms due to known causes other than BPH including neurogenic bladder, urinary tract infection, bladder cancer, bladder stone, urethral stricture; •Previous history of prostatic surgery •Illiterate or having difficulty in filling in a patient diary; •Known hypersensitivity to soy.
Based on the efficacy of finasteride from a previous clinical trial, a minimal difference of 2 mL/sec in Qmax between two groups was used to estimate the sample size in this study. 22 Eighty-eight (88) subjects in each group were required to achieve 80% power at 0.05 significance level, assuming a 10% dropout rate as per a previous alternative medicine study in BPH. 24
Randomization was generated using a computer random number table in blocks of four by the pharmacist (JY) who was also responsible for the preparation of the drugs, but unknown to any of the doctors or research staff. The studied drug, containing 40 mg aglycone-equivalent isoflavones in each capsule, was prepared from Soylife 40 (Acatris, The Netherlands). The placebo used starch and was the same color, size, and shape capsule as the studied drug. Few guidelines are available on optimal dose and length of treatment for patients with LUT, 25 but Japanese males are estimated to consume 20 mg of isoflavones per day, 26 and Kumar et al. used 60 mg of isoflavones in a randomized controlled trial with significant reduction in prostate-specific antigen (PSA). 27 Hence, 40 mg of isoflavones was suggested for this study with regard to the tolerability consideration.
All subjects were followed up every 3 months over a 12-month period. In each visit, the subjects completed questionnaires on demographics, IPSS, and SF-36 that had previously been translated and validated in Chinese. 28 A well-trained male nurse who was blinded to the study group allocation would then perform an uroflowmetry measuring Qmax, an ultrasound scan of the bladder for PVR, and urinalysis on the urine sample. Blood was taken for total testosterone, liver function test, and full blood count at baseline, 6 months, and 12 months, and for PSA and renal function at baseline and 12 months.
Once enrolled, each participant was asked to record their dietary information in a patient diary for 1 week immediately preceding the clinic visit to allow comparison of soy consumption. Assessment of dietary intake was made using the 7-day diet recall (7DDR). 29 Briefly, the 7DDR was a validated, self-administrated instrument designed to measure energy and macronutrient intake during the previous 7 days. Questions on portion size and number of times consumed were asked for 10 soy-food items. Questionnaires data were converted to nutrient data by using the Nutrition Data System database as the unit of grams/day. Dietary food intake of soy isoflavones was compared between two groups at each visit. The content of soy food such as one bowl of tofu or a half bottle of soy milk was transformed into grams in order to be standardized. Participants were also asked to record any adverse reactions noted or concurrent medications (including rescue medications) in the case-report form. These were reviewed by a doctor at each visit when physical examination and compliance check was conducted.
This study was approved by the joint Clinical Research Ethics Committee of the Chinese University of Hong Kong and Hospital Authority, Hong Kong. Written informed consent was obtained from all subjects, and they were able to terminate the participation of the trial at any stage. They were also encouraged to contact the research team for any inquiries during and after the trial. Any subject not returning as scheduled was contacted by telephone to determine his reasons for defaulting or to rearrange another appointment within 7 days. Failure to attend the rescheduled visit was regarded as withdrawal from the study.
Data entry and management was performed using SPSS 11.0. Due to the pilot character of the trial, evaluation was done only with descriptive statistics. Baseline comparisons for the Qmax, PVR, IPSS, SF-36, PSA, and testosterone levels between the isoflavones group and the placebo group were first performed by using Wilcoxon rank sum test. The mean differences at 12 months between the two groups were compared by using independent t tests for normal distribution variables and Mann–Whitney for non-normal distribution variables. The change during the intervention between two groups was compared by using repeated the analysis of covariance test. Normality checking for all outcome measures was performed, and the power was also computed for each comparative analysis. All the analyses were based on intention-to-treat by using the “last observation carried forward” method.
Results
Following recruitment, 551 patients were evaluated for potential enrollment. Three hundred and seventy-five (375) participants did not meet the inclusion and exclusion criteria or refused to participate in the trial: 210 patients had Qmax larger than 15 mL/sec; 130 postresidual volume smaller than 150 mL; and 35 refused to participate in the study due to the frequent study visits required. One hundred and seventy-six (176) patients who met the inclusion and exclusion criteria were randomly assigned to two groups. After 1 year of follow-up, a total of 30 patients had withdrawn from the study, of whom 16 were from the treatment group. The randomization and reasons for withdrawal are detailed in Figure 1.
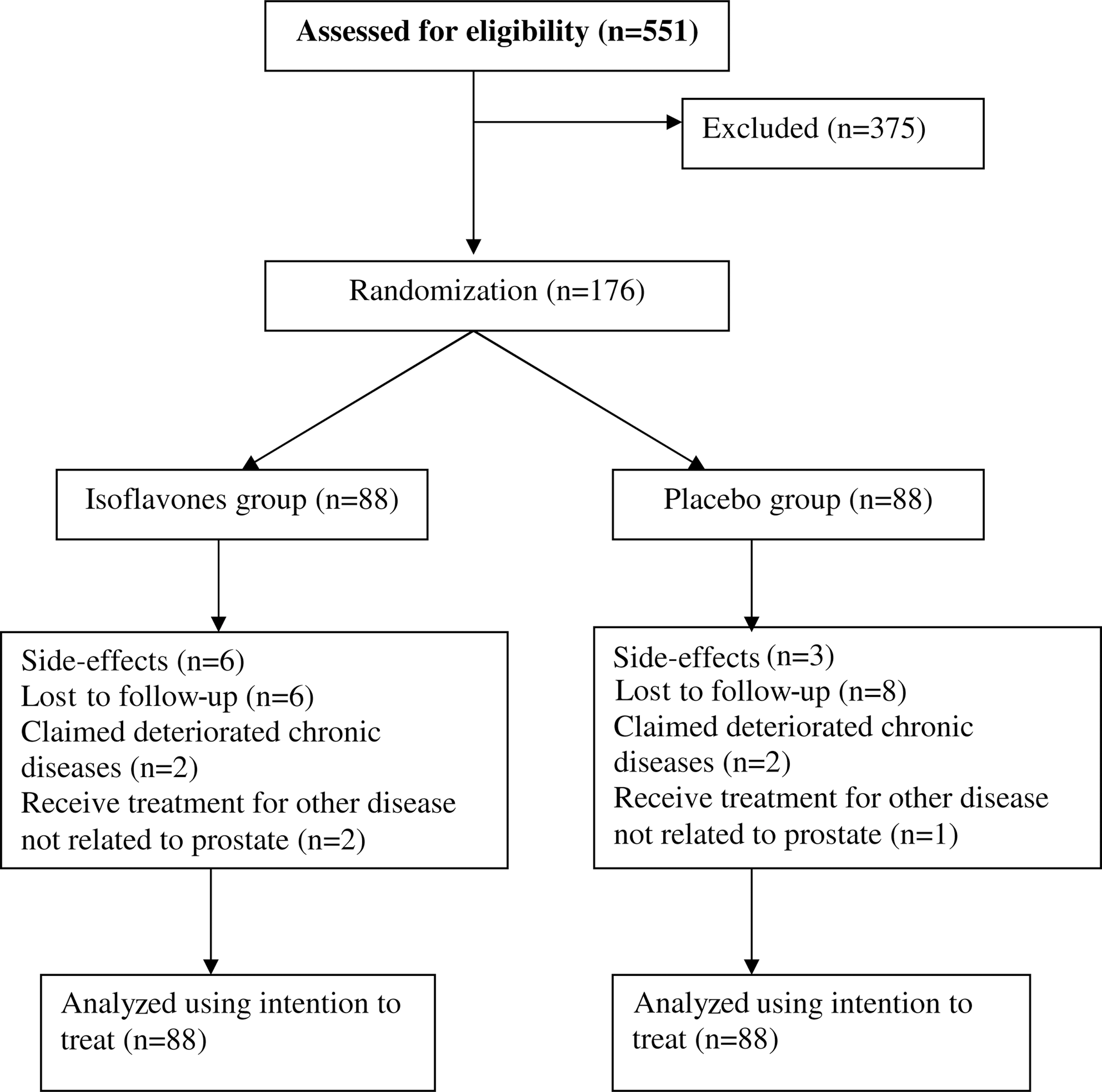
Flow chart showing the randomization, participation, and completion of the study.
The demographic characteristics of the participants are presented in Table 1. The mean age of the patients in the isoflavones group was 65.0±9.4 years, whereas the mean age of the placebo group was 65.1±9.2 years. The mean weight, height, and blood pressure appeared to be similar in both groups. Similar proportions of co-morbidity were also found between the two groups: 85.2% (75/88) in the isoflavones group and 81.8% (72/88) in the placebo group. In addition, the means of IPSS score in the isoflavones and placebos groups were 20.2±6.4, and 19.5±7.0, respectively (p=0.4) (Table 2). The means of Qmax were 10.0±2.5 mL/sec and 10.3±3.0 mL/sec (p=0.3), whereas those of PVR were 125.9±132.1 mL and 107.5±77.5 mL in the isoflavones and placebo groups, respectively (p=0.8). No statistical difference in each domain of SF-36 scores was observed between the two groups. There was also no significant difference in serum PSA and testosterone levels at the beginning of the trial. (PSA 1.7±0.9 ng/mL in the isoflavones group versus 1.6±0.8 ng/mL in the placebo group [p=0.5]; the serum testosterone level was 15.9±5.0 ng/mL in the isoflavones group versus 15.8±6.4 ng/mL in the placebo group [p=0.5]). Therefore, both groups were rather comparable at baseline.
SD, standard deviation; BP, blood pressure.
SD, standard deviation; IPSS, International Prostate Symptoms Scores; QOL SF-36, Quality of Life 36-Item Short Form Health Survey; PSA, prostate-specific antigen.
At the end of the year, Qmax increased and PVR decreased significantly within both groups (p<0.001) (Table 3). The mean changes of Qmax and PVR were 1.7±3.8 mL/sec and 49.0±121.4 mL in the isoflavones group, and 1.3±3.4 mL/sec and 40.0±76.0 mL in the placebo group, respectively. During the second half of the intervention (i.e., from the 6th month to the 12th month), the change in Qmax was marginally different between the two groups (p=0.055) but no significant change from the baseline to 12th month was found between the two groups (p=0.64). There was no significant change of PVR from the baseline to the 6th month (p=0.79) or from the 6th to the 12th month (p=0.18) between the two groups. The change trends of Qmax and PVR from the baseline to the 12th month (p=0.77 and p=0.13, respectively) or from the 6th to the 12th month (p=0.65 and p=0.16, respectively) were not statistically significant (Figs. 2 and 3).
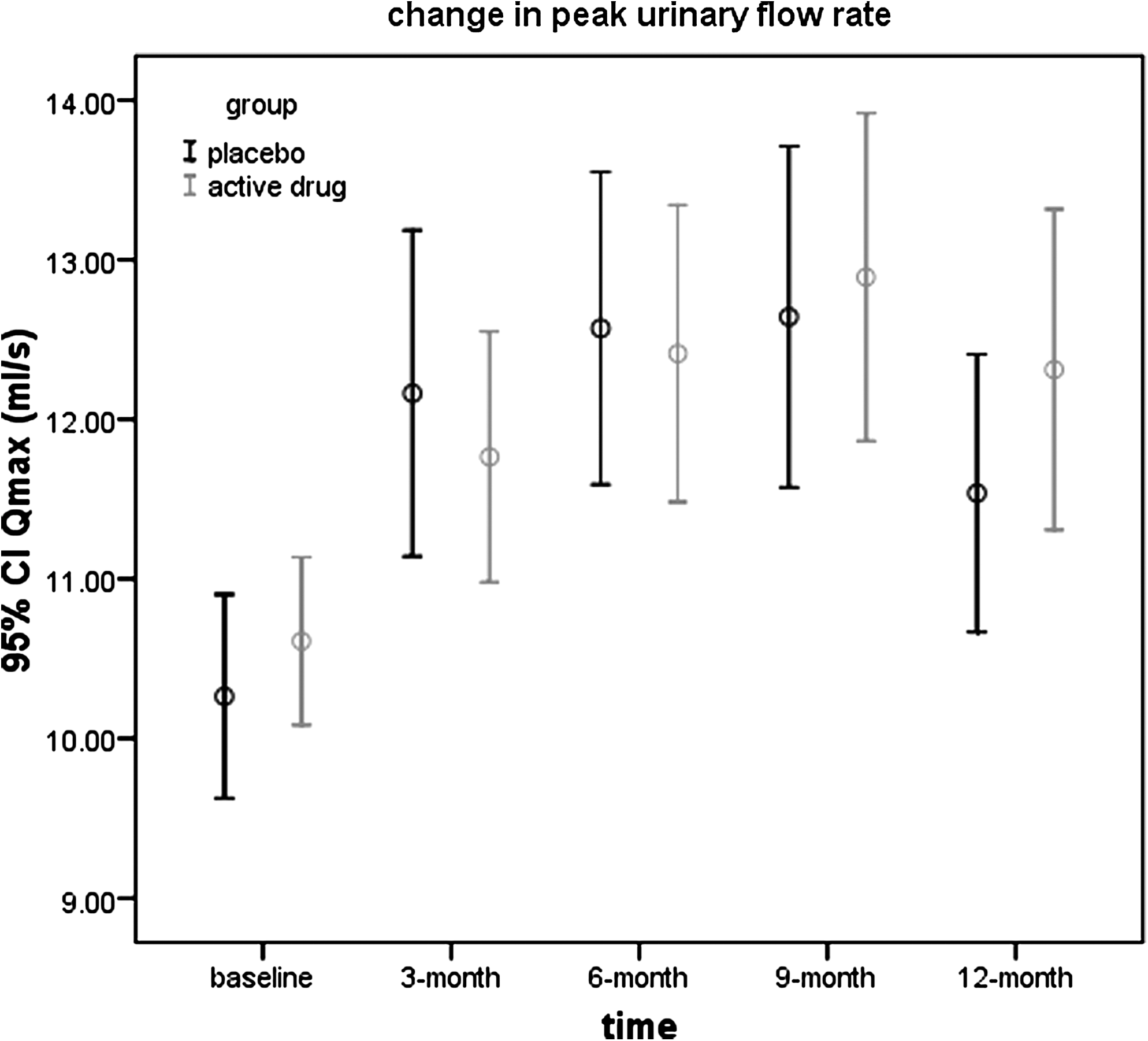
The change trend in peak urinary flow rate (Qmax) of both intervention and control groups over 12 months. CI, confidence interval.

The change trend in postresidual urinary volume (PVR) of both intervention and control groups over 12 months. CI, confidence interval.
P1, the change within groups from baseline to the 12th month; P2, the change between groups from the baseline to the 12th month; P3, the change between groups from the 6th month to the 12th month; Trend P1, the change of trend between groups from baseline to the 12th month; Trend P2, the change of trend between groups from the 6th month to the 12th month; IPSS, International Prostate Symptoms Scores; QOL SF-36, Quality of Life 36-Item Short Form Health Survey; PSA, prostate-specific antigen.
Similarly, the overall IPSS (p<0.001) and the great majority of IPSS items decreased significantly from the baseline to the 12th month in both groups. The change of incomplete emptying scores between the two groups from the 6th to the 12th month was found to be significantly different (p=0.05). The change trend between the two groups from baseline to the 12th month (p=0.75) and from the 6th to the 12th month (p=0.72) was not significantly different with the exception of the “incomplete emptying” score (p=0.05). However, the changes of the general health domain of SF-36 between the two groups from the baseline to the 12th month (p=0.02) and from the 6th month to the 12th month (p=0.055) were (marginally) significantly improved (Table 3).
Since the dietary intake of soy products may affect the result of this trial, participants from both the intervention and control groups were asked to record 7-day food intake in the patient diary every 3 months during the study period for comparison of the soy consumption. There was no significant difference in soy consumption in both groups at each visit (Table 4). However, both groups had an obvious decrease of soy food intake in their daily diet. Because there was no difference in dietary soy isoflavones intake between the two groups at each stage of the trial and adjusted analysis by controlling the soy food intake at each stage of the trial had not shown the significantly different results, the interference effect of soy food intake on the result was disregarded.
SD, standard deviation.
The proportion of patients experiencing any adverse events was not significantly different between the isoflavones group and the placebo group (Table 5). There was no occurrence of severe adverse event in either group during the study period. The nonserious adverse events mainly included skin problems, followed by gout, loss of libido, and generalized pain. No within-groups or between-groups statistical difference of serum PSA, testosterone levels, renal function, liver function, and full blood count were found at the 12th month.
Discussion
Pharmacological therapies including α-adrenergic blockers and/or 5-α reductase inhibitors are the major medical treatments for those who have moderate to severe LUTS/BPH. However, evidence shows that both preparations have many undesired effects. 30 Therefore, many patients who suffer from bothersome symptoms of LUS/ BPH but are worried about the undesired effects of pharmacological therapies may turn to CAM as an alternative treatment. This patient-centered approach is in line with the American Urologic Association's recommendation of “informed patient decision making” as the standard for BPH management. 21 This study shows that isoflavones significantly improve the Qmax and incomplete emptying in IPSS.
Qmax, PVR IPSS, and some of SF-36 scores significantly improved between baseline and 1 year in both the intervention and control groups. Nonetheless, only Qmax (p=0.055) and incomplete emptying subscore in IPSS (p=0.05) were marginally, respectively significantly different between the two groups from 6 to 12 months, in addition to the general health domain of SF-36 from baseline to 12 months (p=0.02) and from 6 months to 12 months (p=0.055). Surprisingly, both groups improved in IPSS and Qmax continually up to month 9, with an increase between months 0 and 3, but both decreased between months 9 and 12. The unusual and unexpected strength of placebo effect observed here needs further investigation. In other words, both groups had similar and sustaining placebo effects up to 9 months, but after that, apparently still existing symptoms overrode expectations. A study in 722 patients aged 50–80 years old with symptomatic BPH using doxazosin showed a significant improvement in IPSS score (decreased by 8.4 points from baseline) and Qmax (increase 2.2 mL/sec from baseline) (p<0.001) in the group using doxazosin. 31 However, a significant improvement was also noted in the placebo group; the IPSS decreased by 6.1 points from baseline and Qmax increased 0.8 mL/sec from baseline. 31 It would be also interesting to know whether the placebo effects in trials of BPH are exceptionally large, and whether the placebo effects are larger with Chinese and other Asian populations than with whites. However, phytotherapy has many questions that remain unanswered concerning the composition, extraction, and mechanism of action of these compounds.
Since the dietary intake of soy food and one's own perception of taking an “actual” medication have strong associations with the effectiveness of the intervention, confounding biases may occur when imbalanced intake of soy food between two groups takes place. Despite there was no statistical difference occurring in soy intake between the two groups, the possibility that effect differences might be attributed to background or subconscious change of dietary soy after entering into the trial cannot be ignored.
This trial has also successfully established the safety profile in this group of patients with BPH and has set the foundation for further longer-term studies on the combined effects of conventional medicines and isoflavones or the role of isoflavones in the primary prevention of BPH, as suggested by the BPH European Urology Guidelines. 32 Conducting randomized controlled trials on CAM faces challenges such as dietary effect. Attempts have been made to minimize them by the add-on dietary intake survey conducted among patients, asking them to guess the group assignment as a way to assess the dietary intake of soy food during the trial. Moreover, while the conventional trials focus on the specific objective outcomes of a symptom or disease, most CAM studies emphasize holistic recovery; hence the consistent improvements in general health domain in quality of life seen in this study may be more meaningful endpoints for this group of medications.
Conclusions
This double-blind pilot clinical study has successfully established the safety of isoflavones. Similar improvement in IPSS and Qmax was present in both the isoflavones and placebo groups up to month 9, and subsequently there was no more improvement in the verum group between months 9 and 12. As incomplete emptying and certain subscales of SF-36 were slightly superior for isoflavones, which might have a specific effect in this situation. These findings set the foundation for further studies with isoflavones in BPH, which should focus on possibly more favorable effects of higher doses and better control of placebo effects.
Footnotes
Acknowledgments
We sincerely thank the Research Grant Council of the University Grant Committee of the Hong Kong Special Administrative Region (Reference No. CUHK 4453/05M), which supplied governmental funding to support the tests, drugs, and manpower of this study. We also thank all the participants who volunteered in this study.
Protocol Registration No.:
Disclosure Statement
No competing financial interests exist.