
Abstract
Objectives:
This study investigated subjective and physiologic responses of lying on a bed of nails (BN) called the Shakti-mat and of listening to relaxing instructions and music. The BN has 6210 sharp-edge 5-mm plastic nails about 5 mm apart.
Design:
Thirty-two (32) healthy participants went through four conditions in randomized orders combining BN and relaxing instructions.
Results:
The subjective pain ratings on the BN increased immediately and reached a peak within 30 seconds. The pain then subsided gradually, indicating a habituation effect. Self-rated relaxation increased over time in all conditions. Systolic and diastolic blood pressures were higher, heart rate was slower, and there was more high-frequency power heart rate variability (HRV), and signs of increasing circulation in the back on the BN. The relaxation instruction especially affected breathing and the HRV-indices standard deviations of normal interbeat intervals and low-frequency power, both known to be responsive to slow breathing. There were no differences in saliva cortisol.
Conclusions:
Healthy participants habituated to the induced pain on the BN and were able to subjectively relax. When on a BN, signs of both sympathetic and parasympathetic nervous system activity were observed. The pain may hypothetically have triggered a parasympathetic response.
Introduction
In the present study, we investigated (1) whether there are any differences in several physiologic and subjective parameters between lying on a bed of nails and a soft bed, and (2) whether there are any differences between listening to relaxation instructions on a CD versus no CD-instructions on the same parameters. The hypothesis of this study is that, on the BN, data will first show an increase in physiologic activation and then a pronounced decrease, subjectively expressed as well as physiologically observable. Our main focus is on activity in the autonomic nervous system (ANS) and its branches, the sympathetic nervous system (SNS), signaling a stress response, and parasympathetic (PNS), signaling recovery. Heart rate variability (HRV) has become one of the most important markers of ANS and especially the PNS. 3 In addition to the ANS, we focus on cardiovascular and respiratory measures relevant to stress. 4 We also measure saliva cortisol, which is sensitive to activity in the HPA-axis.
Materials and Methods
Study population
Thirty-two (32) healthy volunteers participated in the study. They were recruited by Internet ads and by posters at workplaces near the study location. To be included in the study, participants had to report that they were generally healthy, did not have any serious disease, were not currently on sick leave, and have not been on sick leave for more than 14 days during the past year. Further exclusion criteria were a BMI below 19 or above 30 and regular use of the BN. The participants were instructed to refrain from caffeine, nicotine, and any medication 12 hours prior to participation in the study. Participants who were novice to the BN experience were lent one BN and told to try it three times for 20 minutes each time prior to participation in the study. Twenty (20) of the participants were women; most of them had at least some college education and were born in Sweden. Their average age was 40 years and their BMIs and scores of self-rated physical and mental health were normal (Table 1).
SD, standard deviation; BMI, body–mass index.
Procedure
Participants were tested in a stress rehabilitation clinic in a town north of Stockholm, Sweden. One (1) experienced examiner conducted the tests in a room normally used for psychotherapy. Participants were provided with full information and signed an informed consent form before beginning. The study was approved by the local ethics committee.
Participants met with the examiner twice. During the first session, the participants completed the questionnaires, and underwent the first two of a total of four experimental conditions. The remaining two were scheduled for session two, at the same time, 7 days later.
Experimental conditions
The BN used was a Shakti-mat (Team Shakti, Hudiksvall, Sweden) which consists of a soft cotton fabric case filled with a foam rubber rectangle. The top of the mat is covered with 230 round groups of 27 sharp-edged plastic nails. The size of the mat is 16.5” × 25.5” × 1”. The height of the nails is 5 mm and the distance between nails is about 5 mm. The soft bed used was the backside of the same personal Shakti-mat, whose surface is all cotton.
The CD with relaxing instructions used consists of a female voice reading generally relaxing instructions including instructions to breathe slowly. The voice is accompanied by slow and soft synthesizer music. After 5 minutes, the 20-minute track consists mostly of music.
The four experimental conditions were as follows: Condition A—Lying on the BN in silence for 20 minutes. Condition B—Lying on the BN with the CD played through speakers at comfortable volume. Condition C—Lying on a soft bed for 20 minutes in silence. Condition D—Lying on a soft bed listening to the CD. The order of the conditions was randomized so that each session consisted of one BN-condition and one relaxing condition. There are eight orders that allow this: AD-BC, AD-CB, DA-BC, DA-CB, BC-AD, BC-DA, CB-AD, and CB-DA.
Measurements
Questionnaires
Information such as education and nationality was acquired via a questionnaire. Mental and physical health were measured with the SF-36 questionnaire, whose proven psychometric properties for measuring quality of life extend to the Swedish translation. 5,6
Psychophysiologic recording
The procedure started with a 10-minute adaptation period during which the participant was comfortably lying down on a bench, normally used for massage, and was hooked up to the equipment. Participants lay on terry towels, which also covered them for comfort. Recording began with a baseline of 3 minutes, during which participants were told to lie still and be quiet. Thereafter, they went through one of the four conditions described above and finally the participants lay on the terry towel–covered bench in silence for 3 minutes.
Throughout the procedure, end-tidal carbon dioxide (ETCO2), oxygen saturation (SpO2), respiration rate (RR), heart rate (HR), heart rate variability (HRV), skin conductance level (SCL), and back temperature (BT) were measured continuously using an Air-Pas oxycapnograph (PBM, Stockholm, Sweden), a J&J-Engineering I-330-C-2 Physiological Monitoring System (J&J Engineering, Poulsbo, WA), and cStress customized software (PBM, Stockholm, Sweden). In the end of baseline, after 3, 5, 10, 15, and 20 minutes of the experimental conditions, and in the end of the recovery phase, systolic and diastolic blood pressure (BP) and subjective ratings of relaxation on a scale from 0 (very stressed) to 10 (extremely relaxed) were recorded. Subjective ratings of pain were collected at the end of baseline, after every 30 seconds the first 5 minutes and then every 5 minutes throughout the experimental condition and at the end of the recovery phase. Saliva cortisol was sampled at minute 17 of all four experimental conditions. The examiner was in the same room but behind the participant during testing. All data were scanned manually for artifacts, which were edited out except for interbeat intervals (IBIs), which were replaced. All data were segmented in 5- or 3-minute epochs. Data from 1 participant were excluded because of a HR- and another because of an ETCO2-recording with more than 5% distortion during at least one segment. Three (3) saliva samples turned up dry to the lab and could not be analyzed.
The electrocardiogram was recorded from electrodes placed on the left and right wrist with a sampling rate of 1024 Hz. For HR and HRV, IBIs were calculated online using an R-wave peak detection algorithm and stored on a personal computer for offline processing. IBIs were scanned manually for ectopic beats, which were replaced using cubic spline interpolation. Fourier analysis was performed on the 5- and 3-minute segments of detrended data passed through a Hamming window. The HRV measures analyzed were high-frequency power (HF power; 0.15–0.4 Hz), low-frequency power (LF power; 0.04–0.15 Hz), and standard deviation of all normal to normal IBIs (SDNN). Inference testing was applied after logarithmic transformation of the HRV data due to skewed distributions.
CO2 in exhaled air was sampled from a nasal canula (ø = 5 mm) inserted 10 mm into the left nostril. ETCO2 is the peak of the CO2 concentration at the end of exhalation. ETCO2 corresponds well to arterial pCO2. 7 RR was calculated as breaths per minute from CO2 fluctuations. SpO2 as the estimated percentage of hemoglobin binding sites occupied by oxygen was recorded at 2 Hz from a finger sensor placed on the third digit of the left hand. SCL was measured from the middle phalanges of the digits 2 and 4 of the left hand using isotonic gel. BT was measured by a thermistor taped to the right side of the back at heart level. BP was taken with an Omron M5 device (Omron Corporation, Kyoto, Japan). Its cuff was placed on the right upper arm, and the unit at heart level.
Saliva cortisol
Saliva samples were collected using Salivette cotton rolls (Sarstedt, Rommelsdorf, Germany) placed in the mouths of the participants. After 2 minutes they were collected. Participants were told to make them soaked through. Samples were frozen (−18°C) until analyzed. Cortisol levels were measured using Spectria [125I]-Coated Tube Radioimmunoassay kits (Orion Diagnostica, Espoo, Finland). Cortisol levels were logarithmically transformed to avoid skewness.
Statistical analysis
Baseline differences were tested with one-way analyses of variance (ANOVA). Main results for the physiologic measures and subjective units were analyzed using three-way ANOVAs where the three main effects indicate (1) an overall effect of bed-type, (2) an overall effect of listening to a relaxing CD, and (3) an overall effect of time. The interaction effects of these factors were analyzed. No post-hoc analyses, except for the baseline differences, were conducted since they were not relevant to the hypotheses. The α level was set at p < 0.05, two-sided.
Results
Subjective ratings
As shown in Figure 1, there was a quick increase in mean pain rating during the first 30 seconds on the BN followed by a gradual decrease. These changes were highly significant (F = 159.1; p < 0.001). After 5 minutes the mean pain rating was about half of the peak level. The pain ratings on the soft bed were all 0. The mean pain rating did not decrease to 0 until the BN was removed. The two CD conditions were not different in this regard, but there was an interaction between time and CD instructions, indicating a more rapid rise and faster reduction in pain ratings when the CD was present (F = 1.95; p = 0.02).
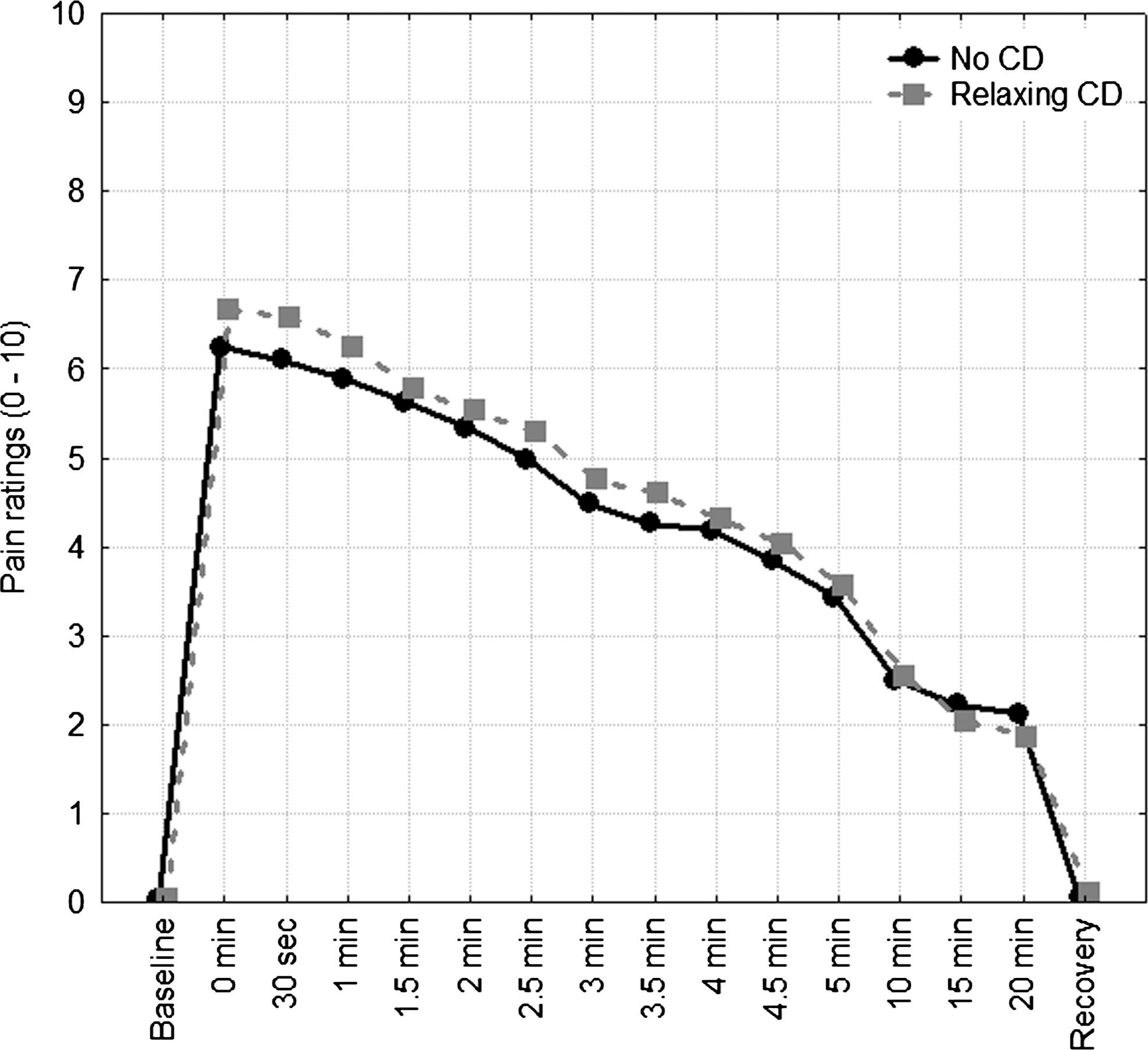
Mean ratings of pain during exposure to the bed of nails when listening to relaxing instructions and not listening (N = 32).
As shown in Figure 2, participants rated relaxation as increasing in all conditions (F = 49.7; p < 0.001). There was a difference in relaxation ratings depending on bed type (F = 5.6; p = 0.02), reflecting the fact that BN participants initially rated their relaxation as decreasing before it increased. On the soft bed, relaxation was increasing from the beginning. This interaction effect was significant (F = 8.8; p < 0.001). In all conditions, relaxation ratings were lower minute 20 than minute 15.
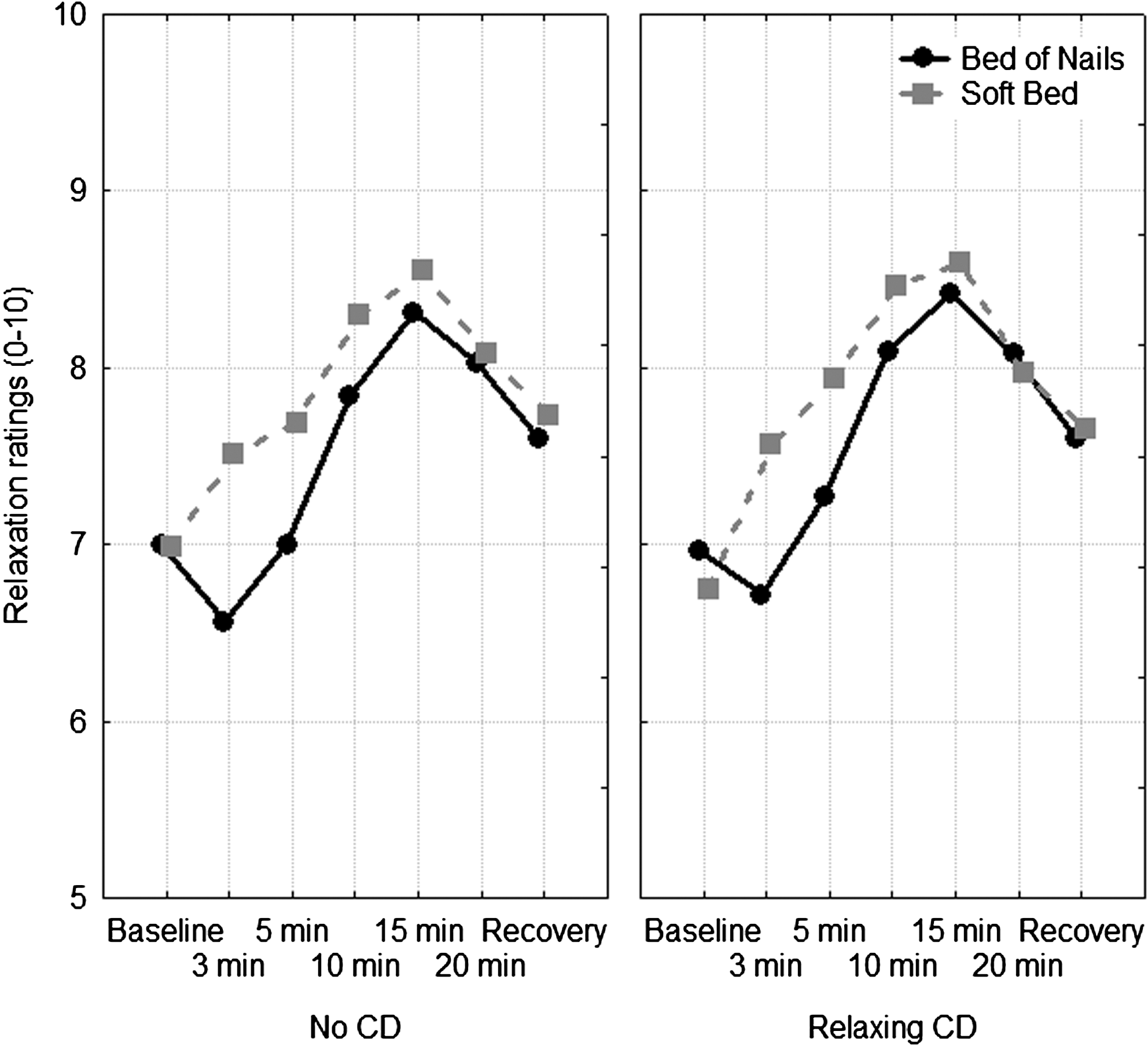
Mean ratings of relaxation during exposure to the bed of nails and the soft bed (N = 32). The two graphs show whether the relaxing CD was present or not. Vertical bars denote 95% confidence intervals.
Physiologic measures
There were no differences in physiologic measurements among the baselines before the various conditions (p > 0.05) with the exception of BT (Table 2). Post-hoc testing (Scheffe's) of the BTs reveal that conditions A and B differed from C and D (p < 0.01), but A was not different from B, and C was not different from D (p > 0.05). Thus, when the participants were about to lie on the soft bed, their BT were significantly higher. To test for possible order effects, we tested baseline differences in BT between participants who had been on the BN prior to the soft bed and those who had not, using two unpaired t tests. These differences were significant (p < 0.001 [before C] and p < 0.01 [before D]) with a higher temperature when preceded by a BN condition.
N = 31.
BL, baseline; SD, standard deviation; ETCO2, end-tidal CO2; SpO2, oxygen saturation; HRV, heart rate variability; SDNN, standard deviation of all normal to normal interbeat intervals; LF, low frequency; HF, high frequency.
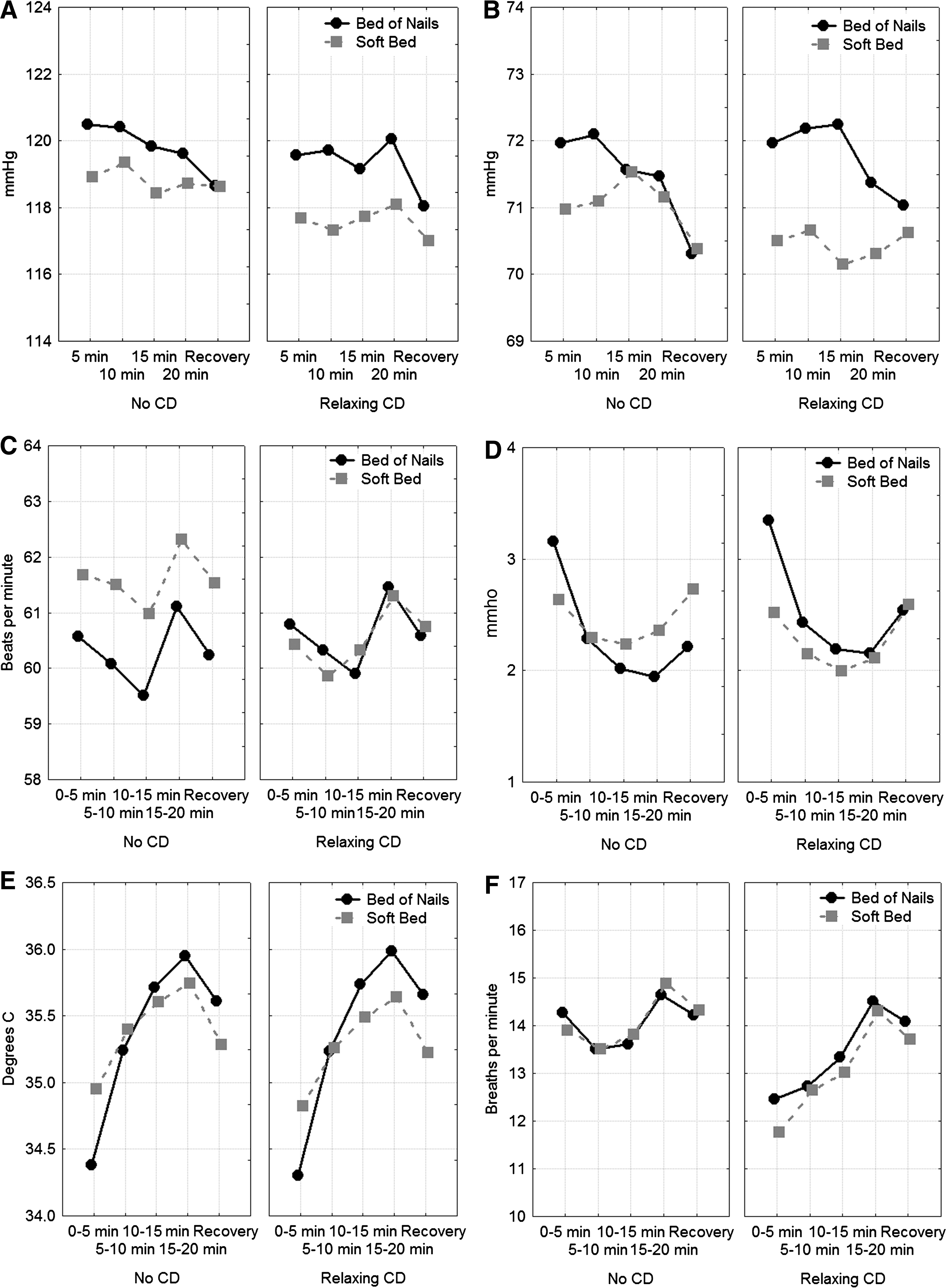
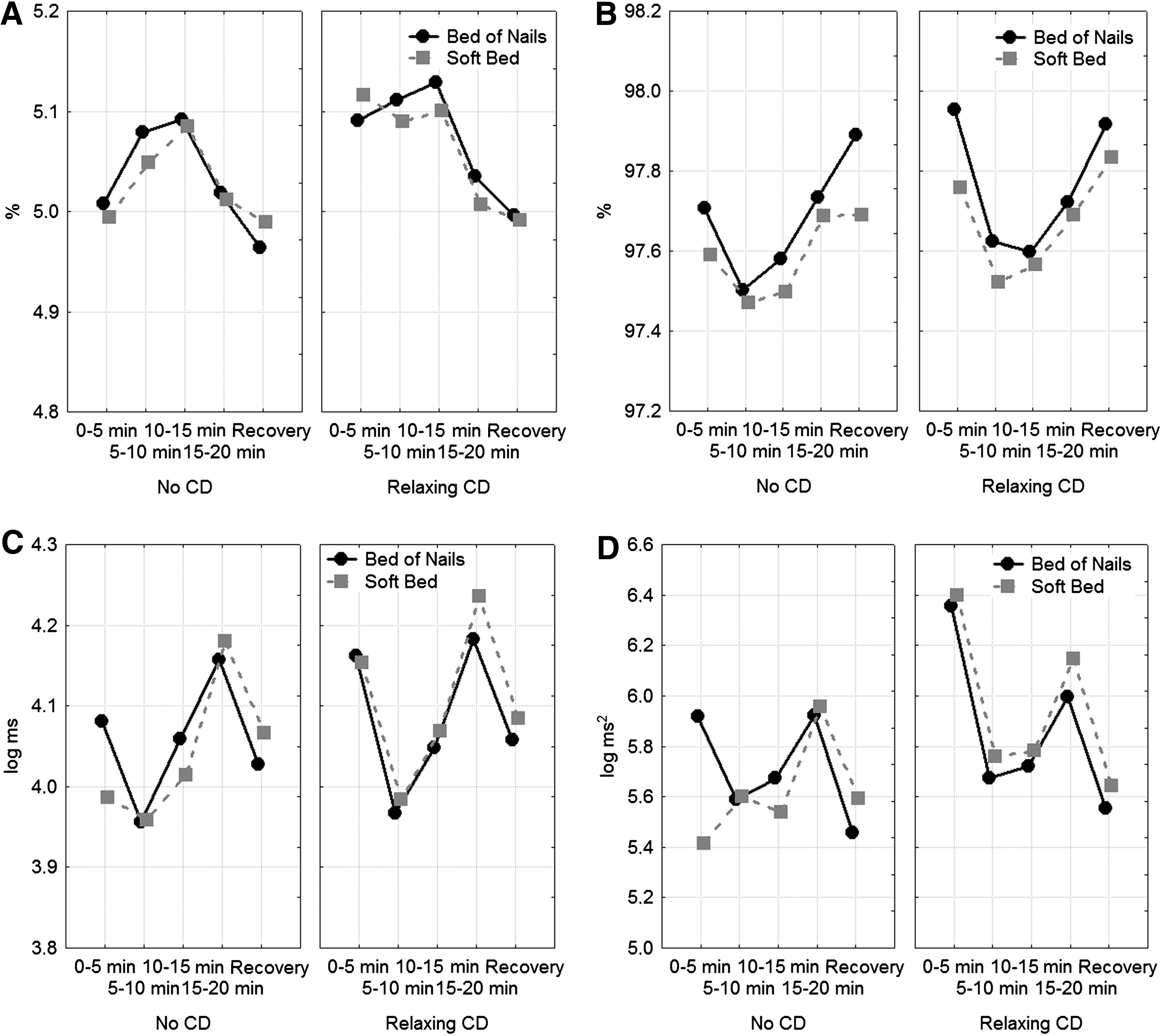
As shown in Figures 3 and 4, the participants had higher systolic and diastolic BPs, lower HR, and more HF HRV when on the BN. They had lower systolic BP, lower RR, higher ETCO2, more SDNN, and LF HRV when listening to relaxing instructions on CD. All physiologic measures, except HF HRV, changed over time. SCL decreased more and BT increased more over time while lying on the BN than on the soft bed. BT also increased more with relaxing instructions than without. Slower RR, higher ETCO2, and higher SpO2 occurred initially when listening to the relaxing instructions, but these differences disappeared over time. The same is true for the HRV variables SDNN and LF HRV. There was no interaction effect between bed type and whether the participants were listening to relaxing conditions or not, nor were there any three-way interactions (Table 3).
Means of
Means of

N = 31.
Rounded to 0.05. Actual ps = 0.047, 0.047 and 0.046, respectively.
ETCO2, end-tidal CO2; SpO2, oxygen saturation; HRV, heart rate variability; SDNN, standard deviation of all normal to normal interbeat intervals; LF, low frequency; HF, high frequency.
As shown in Table 4, there were no effects of either bed type or relaxing instructions on saliva cortisol.
Discussion and Conclusions
The subjective pain ratings on the BN increased immediately and reached a peak within 30 seconds. The pain then subsided gradually, indicating a habituation effect. Self-rated relaxation increased over time in all conditions. On the BN, relaxation decreased before it increased. Possibly the initial pain hindered relaxation. Listening to relaxing instructions had no significant effect on subjective relaxation. A drop in relaxation during the last 5 minutes of all conditions may indicate that people were disturbed by taking the cortisol sample at that time.
Both the systolic and the diastolic BPs were higher, HR was slower, and there was more high-frequency HRV when lying on the BN compared to the soft bed. In addition, there were greater decreases in SCL and increases in BT when on the BN. A short-term increase in BP is typically explained by SNS activity. A lower HR is an indication of PNS activity. The latter also was supported by more high-frequency HRV. 8 It is possible that the pain triggers a PNS response, which might have had evolutionary advantages (lie still when hurt). In SCL, we observe an initial SNS response on the BN, which subsides. This parallels the subjective reports of pain and relaxation. BT increased more on the BN. Moreover, there were baseline differences in BT that can be explained by the other session-paired condition. The soft bed conditions were secondary to a BN condition for half of the participants, while the BN conditions were always preceded by a soft bed condition. The results showed that the effect on BT of the BN remained and spilled over to the subsequent baseline conditions. The higher and increasing temperatures can be explained by increased circulation in the back.
The relaxing instructions lowered RR, raised ETCO2, and increased SDNN and low-frequency HRV. Furthermore, the initial difference with lower RR and higher ETCO2, SpO2, SDNN, and LF HRV when participants received instructions gradually disappeared over time. The breathing instructions, which was most frequent the first 5 minutes, is a probable cause since all the differences observed may be a direct effect of slower breathing. 9,10 It is known that slow breathing can have positive health effects. 10,11 There is no difference in saliva cortisol that can be referred to either bed-type or the relaxing instruction.
Limitations and Future Directions
Because all the participants were healthy and had normal physiologic values, the potential for improvements was small. There are floor and ceiling effects in all physiologic measurements. A study with a more unhealthy population may have produced more pronounced effects. However, since this is the first study of physiologic effects of a BN, the aim was to provide reference data from a healthy population.
Exposure to the BN within the study differs from the normal use of the device. Participants have a number of sensors attached to their bodies, and there were a total of 32 BPs taken and participants were repeatedly asked to provide saliva samples, and to estimate the pain levels and relaxation levels. However, an effort was made to make the situation comfortable with soft lighting and warming terry towels. Most participants reported high levels of relaxation and many seemed to slumber.
Since this is, to our knowledge, the first exploratory study of the physiologic effects of BN, the results should be interpreted with some caution. Some differences are small and the sample size is also small. Future studies may show whether these findings are replicable, stable, and whether any of the effects found were due to a too-high α value.
In conclusion, SNS-activity (BP and initially SCL) and the two most important signs of PNS activity (lower HR and more HF HRV) and increasing circulation in the back can be observed on the BN. This might be important for the use of the BN as a device for physiologic recovery and increased relaxation. However, whether it has a clinically significant effect must be studied more in details in clinical trials. The relaxation instruction affected breathing and to some extent the ANS. Much of the physiologic responses are in parallel with subjective ratings. These effects are partly in line with the initial hypotheses. Relaxing on a BN is possible.
Footnotes
Acknowledgments
This study was funded by Team Shakti AB, Hudiksvall, Sweden.
Disclosure Statement
No competing financial interests exist.