
Abstract
Objectives:
This study is aimed to evaluate the therapeutic efficacy and safety of CCH1, modified from an ancient herbal formula in Traditional Chinese Medicine, for the residents with constipation in long-term care.
Methods:
In this randomized, double-blind, placebo-controlled trial, 90 residents from three long-term care units were randomized to 8 weeks of treatment with CCH1 or placebo and then the subjects were followed up for an additional 4 weeks.
Results:
The mean numbers of weekly spontaneous bowel movement in the CCH1 group were greater than in the placebo group during the treatment phase of 8 weeks (p < 0.05); the greatest difference was during weeks 1–4 (6.2 ± 2.2 versus 3.4 ± 2.1, p < 0.001). Smaller mean numbers of weekly rectal treatments were observed with CCH1 compared with placebo during weeks 1–8 (p < 0.05). The mean numbers of weekly rescue laxative tablets of magnesium oxide were significantly less in the CCH1 group than in the placebo group during the entire 12-week period (p < 0.01), with the greatest difference during weeks 5–8 (14.4 ± 16.3 versus 33.4 ± 23.5, p < 0.001). No significant safety concerns were noted.
Conclusions:
The six-herb formula (CCH1), compared with placebo, is effective on the treatment of constipation in long-term care. However, its maintenance effect needs further trial. Comparison of efficacy or cost-effectiveness with current laxatives is encouraged.
Introduction
Laxative use is very common in the elderly, and they are prescribed to about 75% of institutionalized patients for bowel regulation. 6 Although there are a large number of laxative preparations available, there is only limited evidence supporting the use of many therapeutic agents, 7 including commonly used saline laxatives, stimulant laxatives, many bulking agents, enemas, and suppositories. 8,9 In addition, the newer laxative agents are more expensive, but not necessarily more effective or safe. 10 As a result, approximately 50% of patients with self-reported chronic constipation are dissatisfied with current therapies. 9,11 Professionals also noticed that there have been few advances in laxative therapy in half a century. 12
In a recent survey in Taiwan, up to 40% of Chinese patients with chronic gastrointestinal disorders sought complementary or alternative treatment, and 96.6% of them used Chinese herbal medicine with the risks of unknown efficacy and safety. 13 A high-quality systematic review of constipation management in North America also found a lack of quality randomized controlled trials that have evaluated herbal supplement treatment. 14 Although Traditional Chinese Medicine (TCM) is the primary system of medicine in Asia for thousands of years, the scientific basis of TCM needs to be established. Therefore, this study aimed to evaluate the efficacy and safety of a Chinese herbal formula on the treatment of constipation in long-term care.
Participants and Methods
Participants
The study was performed at three long-term care units in Taiwan from September 2006 through February 2008. Eligible participants were men and women aged 20 years and older with known chronic constipation at the screening visit and confirmed by at least one of the following criteria during the last month before enrollment: intake of magnesium oxide (MgO, 250 mg/tablet) ≥750 mg per day, intake of bisacodyl ≥5 mg per day, concurrent use of at least two classes of laxatives, receiving enema or suppository at least once a week, and spontaneous bowel movement (SBM) less than 3 times a week.
Patients were excluded from entering the study for the following reasons: known cause of colorectal obstruction or structural lesions (e.g., intestinal neoplasm, anal abscess, anal fistula, anal fissure, rectocele, megacolon), inflammatory bowel diseases, irritable bowel syndrome, hypothyroidism, spinal cord injury, muscular dystrophy, known severe hepatic or renal insufficiency (e.g., liver cirrhosis or receiving hemodialysis), unknown cause of gastrointestinal bleeding or acute infection, exposure to any other investigational drug (within 30 days prior to enrollment), history of allergy to the composition of the study medication, new onset or unstable psychiatric disorders, pregnancy or breastfeeding, history of alcohol or drug abuse, and any condition associated with poor compliance with medical treatment.
The study was performed in compliance with the principles of the Declaration of Helsinki and with “good clinical practice.” Informed written consent was obtained from all participants, and the study protocol was approved prior to being conducted by the research ethics committee of National Taiwan University Hospital. The study was registered (ClinicalTrial.gov Identifier: NCT00354575) and followed the recommendations of the International Committee of Medical Journal Editors.
Study medication
The choice of herbal formulation (CCH1) was based on the theory of TCM and the clinical experiences of TCM doctors. 15,16 It was modified from the famous formula of “Wen-Pi-Tang” in the Tang Dynasty, which was aimed at strengthening the function of the gastrointestinal system to improve stool passage for the elderly or chronically ill patients with constipation. 17
Built on the basic composition of Wen-Pi-Tang, the herbal preparation used in this study contained six herbs, which are listed in Table 1. All herbs were obtained from Pharmaceutical Co. Ltd., a qualified manufacturer of concentrated herbal extracts with Good Manufacturing Practices according to Taiwanese authorities. The herbs were authenticated at the Brion Research Institute in Taiwan on the basis of standards specified in the Taiwan Pharmacopoeia of Chinese Medicine (2004 edition). Contamination screening for heavy metals, pesticides, and aflatoxins was performed to ensure safety for human consumption. Decoction and extraction of mixed herbs was performed in a single batch to ensure consistency of quality. After extraction, herbal preparation was separated, concentrated, and spray-dried into the form of a powder and packed in sealed opaque aluminum foil bags. A placebo made of stirred fried starch colored like CCH1 was packed in an identical package. All packages were dispensed by an independent research staff in a separate office after the visit.
Study design
This double-blind, placebo-controlled, randomized study had two parallel groups with a total treatment phase of 8 weeks and an additional follow-up phase of 4 weeks. Because some participants in long-term care have poor cognitive function, currently available questionnaires for the severity of constipation are not suitable for them. To obtain baseline information and assess the degree of constipation, all patients had a run-in period of 1 week before randomization with MgO prescribed (250 mg three times a day) for ethical reasons. According to the enema and bowel frequency during the run-in period, the severity of constipation was classified into three categories: severe, moderate, and mild. Using the supplement MgO and using enemas more than once a week was regarded as “severe.” The residents who received an enema once a week or had less than three spontaneous bowel movements (SBMs) were classified as having “moderate” constipation. The frequency of SBMs 3–7 times a week was referred to as “mild.” Participants with an average of more than 1 SBM per day were excluded.
Residents who fulfilled the inclusion criteria and met none of the exclusion criteria were randomized to the study medication according to a computer-generated randomization schedule. Randomization was stratified based on Barthel's index (≤30, 35–60, >60) and the severity of constipation (mild, moderate, or severe). With the exception of the programmer and project statistician performing the interim analyses, all persons involved in the conduct and management of the study were blinded to individual patient treatment. The blinding was not broken for any patient during the study.
Patients were withdrawn from the study for any of the following reasons: hospitalization, discharge from long-term care, development of intolerable or worsening adverse events (AEs), and failure to comply with the protocol or withdrew consent.
Interventions
The patients with mild or moderate constipation were instructed to take one pack of 1.5 or 3.0 g of CCH1 powder (treatment group) or placebo (control group) once daily in the morning for up to 8 weeks. The patients with severe constipation received one pack of 3.0 g of powder in the morning and the other pack of 1.5 g at night. After 8 weeks of treatment, patients were followed up for 1 additional month without CCH1 or placebo. After randomization, a fixed initial low dose of MgO was given for both groups according to the severity of constipation. During the whole study period of 12 weeks, only one rescue oral laxative of MgO was allowed to be used. The blinded primary physician added MgO and titrated its dosage every week (increased by up to 750 mg/day once a week, maximum dose of 2.0 g/day) according to the daily stool diary of the previous week until the optimal bowel performance (3 SBMs/wk to 3 SBMs/day without any rectal treatment). If the patients had diarrhea, MgO was first withheld by the nurses in long-term care. If diarrhea persisted without MgO, the study medication was withheld or a reduced dosage was prescribed by the physician. In addition, a bowel routine protocol was set for the study sites: If there was no bowel movement (BM) by day 3, the nurse gave a suppository of bisacodyl or glycerin ball on day 3; if there was no BM after 8 hours of suppository insertion, an enema was given. Meanwhile, the caregiver could apply a digital maneuver to dig out the hard stool or stimulate the rectum when necessary.
Assessment
Patients were seen every week by the same primary physician with licenses for both conventional medicine and TCM during the entire study period of 12 weeks. At each visit, patients were interviewed by the doctor for symptoms, compliance, and occurrence of AEs and underwent physical examination. AEs were monitored with a comprehensive symptom questionnaire as well as clinical laboratory testing.
Daily stool diaries were kept by the attendant nurses from the beginning of the run-in period to the completion of the study. All caregivers involved in the study had been experienced in long-term care for at least 3 years and received training on keeping a stool diary prior to the start of the study. The caregiver recorded each bowel movement with additional notes on stool consistency, stool amount, and the use of rectal treatment (RT) including enema, suppository use, or digital maneuver. For clinical practicality, stool consistency was classified into four categories (1 = hard, 2 = moderate, 3 = loose, 4 = diarrhea). Stool amount was estimated by the caregiver and classified into three categories (S = small, <250 g; M = moderate, 250–500 g; L = large, >500 g) according to the national guidelines of the Registered Nurses Association. 18 SBM was defined as stool passage without digital maneuver and without the use of suppository or enema on the same day. Global assessment of efficacy was evaluated by the principal caregiver's subjective feeling of adequate relief of the patient's constipation by the study medication using a 5-point Likert scale (2 = markedly improved, 1 = slightly improved, 0 = unchanged, −1 = slightly worse, −2 = markedly worse).
Efficacy
There were three co-primary efficacy endpoints in the study: the mean numbers of SBM per week during weeks 1–4, 5–8, and 9–12; the mean numbers of RT per week during weeks 1–4, 5–8, and 9–12; and the mean numbers of rescue laxative tablets of MgO per week during weeks 1–4, 5–8, and 9–12.
Secondary endpoints included (1) mean proportion of stool consistency per week (hard, moderate, loose, diarrhea) during weeks 1–4, 5–8, and 9–12; (2) mean proportion of stool amount per week (small, moderate, or large) during weeks 1–4, 5–8, and 9–12; (3) global caregiver assessment of efficacy at week 8; and (4) cumulative incidence of AEs during the entire study period.
Safety
Safety evaluations included AEs and serious adverse events (SAEs) reporting, vital sign, physical examination findings, and laboratory results. Blood was collected at baseline and at the end of drug administration (week 8). Blood tests included complete blood count with differential count, plasma glucose, aspartate aminotransferase, alanine aminotransferase, total bilirubin, alkaline phosphatase, urea nitrogen, creatinine, albumin, thyroid-stimulating hormone, free thyroxine, sodium, potassium, calcium, phosphate, magnesium, uric acid, triglyceride, and total cholesterol.
Statistical analysis
An intent-to-treat analysis was conducted on all patients randomized to therapy who had a postbaseline assessment of at least one of the co-primary efficacy parameters. All patients who had taken at least one dose of study medication after randomization were included in the safety analysis. A last observation carried forward analysis was conducted for any missing data of primary or secondary outcomes except global assessment of efficacy and adverse events. Statistical analysis was performed using SPSS software version 13.
Numerical data were compared using Student's t-test. Categorical data were compared using the χ 2 test or Fisher's exact test where appropriate. These comparisons were made at a two-sided α level of 0.05. The Fisher's exact test was used to compare the proportion of patients reporting adverse effects in the two groups.
Sample size considerations
Based on a previous unpublished pilot study, the standard deviations of the mean weekly SBM and RT during weeks 1–4 were calculated to be 2.5 and 0.6, respectively. Assuming a mean difference of 2 SBMs/wk or 0.5 RTs/wk, a sample size of 34 or 30 patients would be required, respectively, in each study arm to achieve a power of 0.9 and a two-sided α-value of 0.05. In addition, according to the same pilot study, the standard deviation of the mean weekly tablets of MgO use during weeks 1–8 was calculated to be 15. Using the same assumptions, a sample size of 27 patients per group would be required to detect a mean difference of 14 tablets of MgO/wk. A dropout rate of 25% was anticipated, yielding a total sample size of 90 patients for each of the three clinical outcomes.
Results
Participants, study conduct, and completion
A total of 168 residents in long-term care who had constipation were screened; 90 met the inclusion criteria and were randomized. The reasons for exclusion are shown in Figure 1. Forty-five (45) patients were assigned to the CCH1 treatment group and 45 to the placebo group. The baseline characteristics of the patients were similar between the two treatment groups (Table 2). A total of 23 (25.5%) patients dropped out of the trial during the treatment phase (weeks 1–8): 12 (26.6%) in the CCH1 group and 11 (24.4%) in the placebo group (p = 0.809). Another 9 (10.0%) patients withdrew from the study during the follow-up phase of an additional 4 weeks (weeks 9–12): 6 (13.3%) in the CCH1 group and 3 (6.7%) in the placebo group (p = 0.485). Twenty-seven (27; 60.0%) patients in the CCH1 group and 31 (68.9%) patients in the placebo group completed the study (Fig. 1).
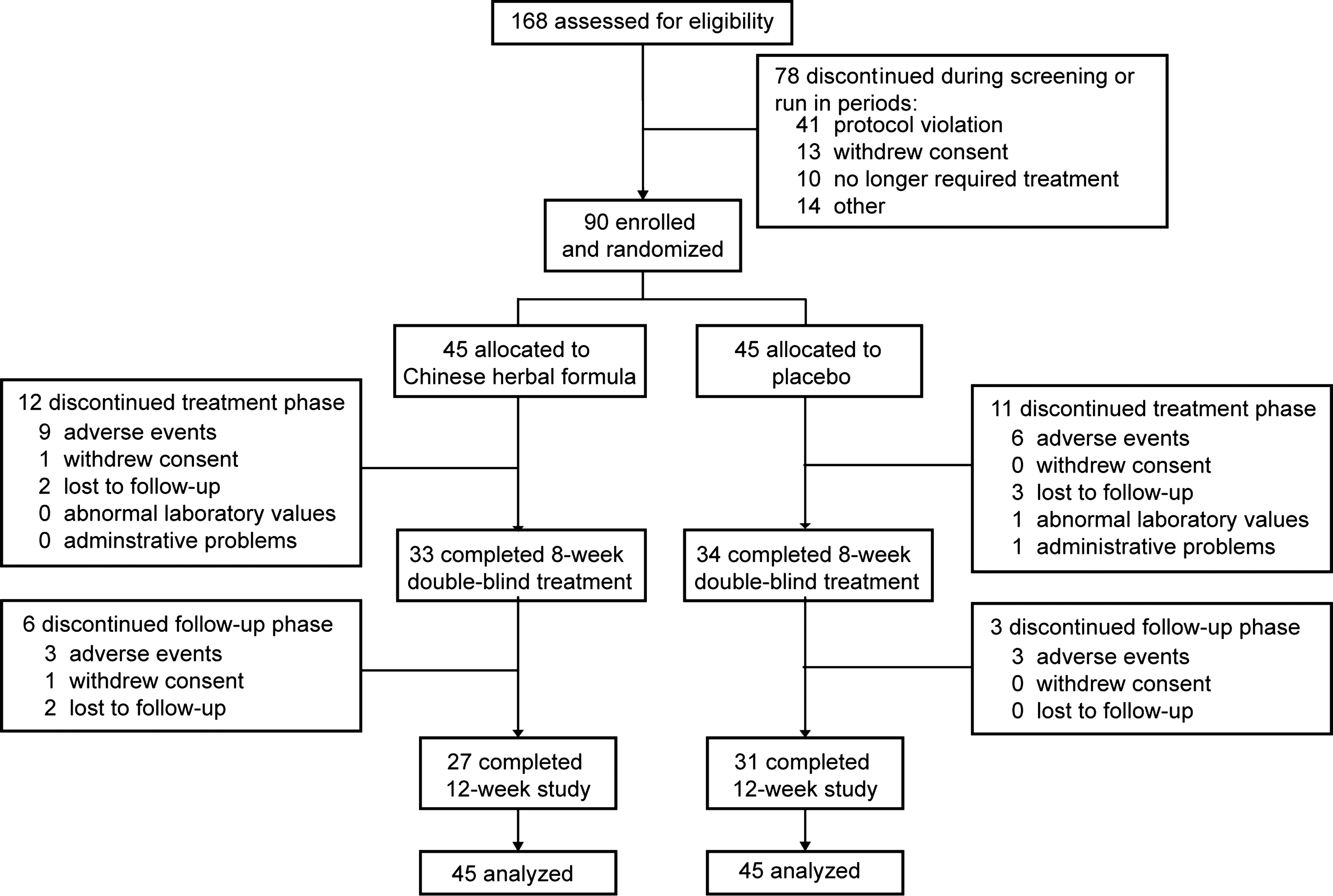
Study flowchart.
SD, standard deviation; SBM, spontaneous bowel movement; MgO, magnesium oxide.
Primary efficacy analysis
The mean numbers of SBMs/wk in the CCH1 group were greater than in the placebo group during weeks 1–4 (6.2 ± 2.2 versus 3.4 ± 2.1, p < 0.001) and weeks 5–8 (5.6 ± 2.0 versus 4.6 ± 2.5, p = 0.049; Fig. 2). Smaller mean numbers of RTs/wk were observed in the CCH1 group compared with the placebo group during weeks 1–4 (0.5 ± 0.5 versus 1.1 ± 1.1, p = 0.001) and weeks 5–8 (0.4 ± 0.5 versus 0.8 ± 1.1, p = 0.024) (Fig. 3). There were, however, no significant differences in the frequency of SBMs/wk (4.3 ± 2.7 versus 4.1 ± 2.4, p = 0.659) or RTs/wk (0.6 ± 0.6 versus 0.8 ± 1.1, p = 0.304) between the two groups during the additional follow-up phase of 1 month (weeks 9–12). With regard to the need for a rescue laxative (MgO), the mean numbers of tablets of MgO/wk were less for the patients who were given CCH1 than for the patients who received placebo during the entire treatment phase and the additional 4 weeks of follow-up (p < 0.01; Fig. 4); the greatest difference was during weeks 5–8 (14.4 ± 16.3 versus 33.4 ± 23.5, p < 0.001).

Frequency of spontaneous bowel movements (SBM) over time in randomized residents. SBM is defined as stool passage without digital maneuver and without the use of suppository or enema on the same day. SEM, standard error of the mean.
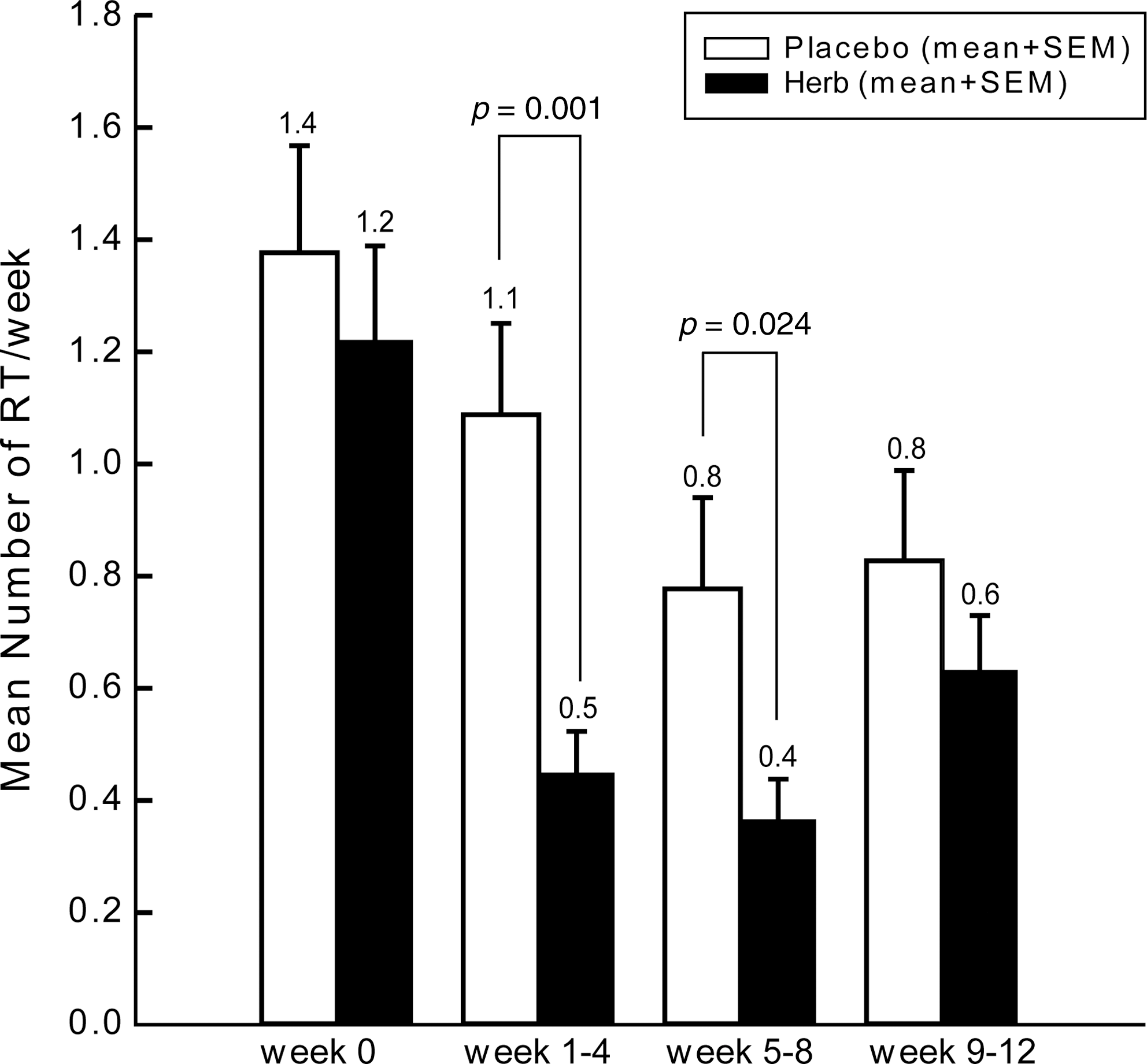
Frequency of rectal treatments (RT) over time in randomized residents. RT including enema, suppository use, or digital maneuver. SEM, standard error of the mean.
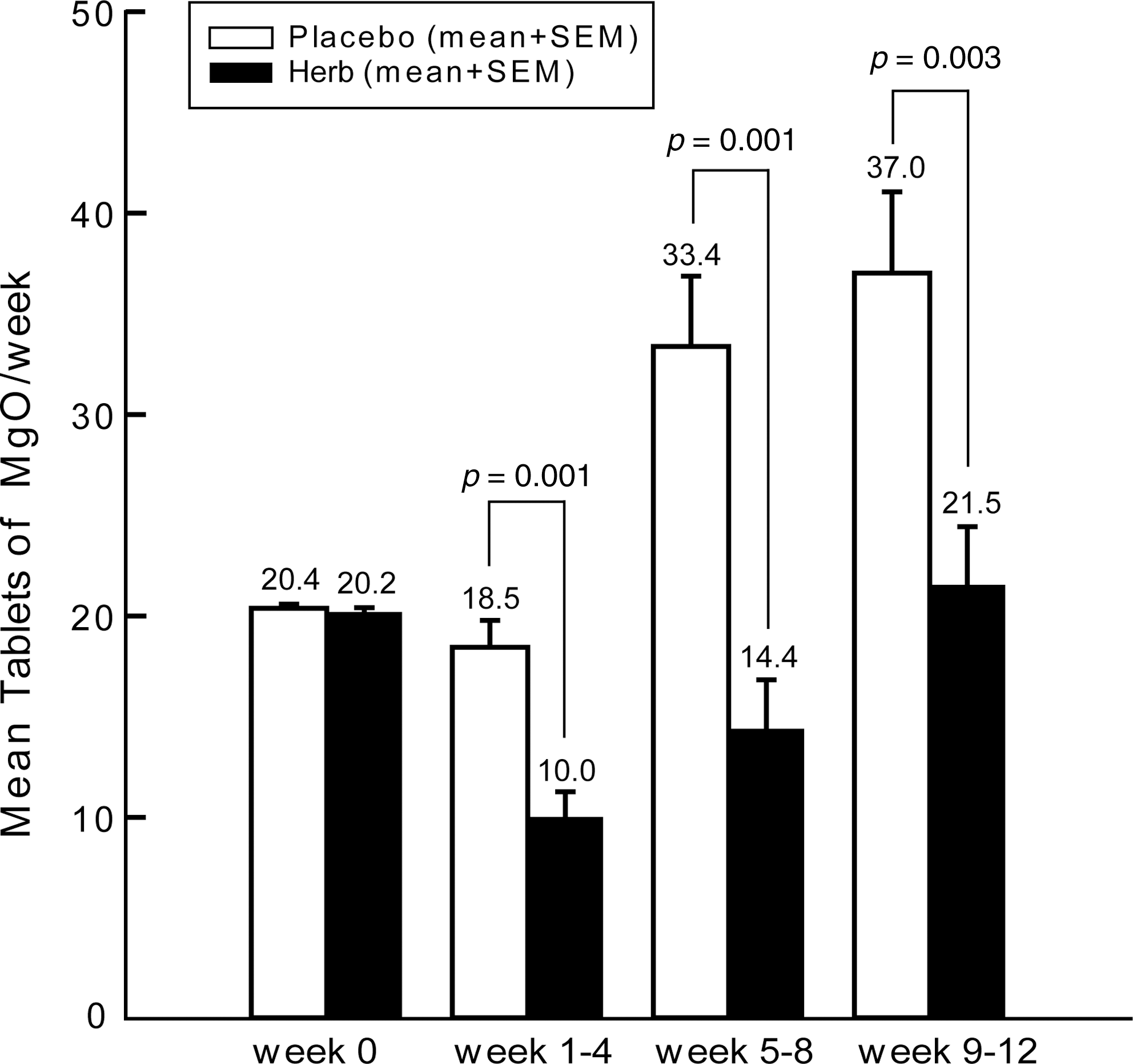
Mean number of rescue laxative tablets of magnesium oxide (MgO) over time in randomized residents. SEM, standard error of the mean.
Secondary endpoints
There were no significant differences in any category of stool consistency (hard, moderate, loose, diarrhea) and stool amount (small, moderate, large) between the two groups during the run-in period before randomization and the entire study period at all time points except for a lower proportion of hard stools/wk (3.0 ± 8.0% versus 8.5 ± 14.0%, p = 0.028) and a higher proportion of loose stools/wk (24.9 ± 25.0% versus 16.4 ± 17.3%, p = 0.070) in the CCH1 group than the placebo group during weeks 1–4. For the 67 (74.4%) patients who completed the treatment phase of weeks 1–8, 65 patients (2 had missing data) were evaluated by global assessment of efficacy by caregivers at week 8, but no significant differences between the two study groups were noted.
Safety and compliance
All patients had good compliance, with at least 90% compliance in both groups except for 1 patient with 86%. With a protocol including frequent weekly visits and detailed records, the cumulative incidences of at least one AE for the CCH1 and placebo groups (95.6% versus 93.3%, p = 1.000) were high during the entire 12-week study period. There were 12 and 9 patients (26.7% versus 20.0%, p = 0.455) in the CCH1 and placebo groups, respectively, who discontinued the study because of hospitalization for SAEs (Table 3). With regard to the most common AE, the CCH1 group had 5 more patients with dermatitis (31.1% versus 20.0%, p = 0.334) and 5 more patients with diarrhea (24.4% versus 13.3%, p = 0.283) than the placebo group. The patients with dermatitis or diarrhea had self-limited symptoms or responded to conservative management. There were no significant differences between the two groups in the incidence of any one of the common AEs or SAEs.
One (1) in herb group had upper gastrointestinal (GI) bleeding and chronic obstructive pulmonary disease (COPD) with acute exacerbation; the other in placebo group reported pneumonia and urinary tract infection.
Discussion
Despite the fact that there are few practical laxatives available for long-term care residents, it is a time-consuming and expensive process to rely on conventional drug development for additional treatment options. However, in June 2004, the U.S. Food and Drug Administration issued new guidelines that permit the approval of herbal mixtures if they can be shown to be safe and effective, even if the active constituents are not known. 19 In the current study, compared with placebo, the six-herb TCM formulation significantly increased SBMs during the treatment period of 8 weeks while concurrently reducing the need for rectal treatment and oral laxatives. This study is a good example of using currently available botanical products to target the health issue, in which there has been little progress and limited innovation over the past decades.
According to the systemic review of Tramonte et al., they concluded that laxatives and fiber increase BM frequency by an overall weighted average of 1.4 BMs/wk compared with placebo. 20 Bub et al. recently reported that a kind of herbal tea (containing senna leaf, ginger rhizome, licorice root, etc.), when added to the standard treatment regimen for nursing home residents with chronic constipation, increased BM by an overall average of 1.0 BM/wk during the 28-day study period compared to the addition of a placebo tea. 21 In the current study, compared with placebo, CCH1 increased the weekly numbers of SBM by an average of 2.8 (95% confidence interval [CI] 1.8–3.8) during weeks 1–4 and 1.9 (95% CI 1.0–2.7) during weeks 1–8 with concurrent reduction of weekly rescue laxative of MgO tablets by an average of 8.4 and 13.7, respectively.
Based on the theory of TCM, one with the balance of yin and yang is in a healthy status. Once the yin or yang is diminished, the balance is broken and one will manifest some symptoms and signs of diseases. Thus, to regain the balance of yin and yang is the central concept of Chinese medicine for treating diseases. 22 In older or chronically ill patients, most of their constipation is originated from decreased lower gastrointestinal function, and it is regarded as the presentation of yang Deficiency from the viewpoints of TCM. 15 Therefore, the majority of the target population in long-term care in this study was estimated to be the pattern of yang Deficiency. Without the pattern diagnoses based on TCM, this study design is easier to replicate or translate into routine care of constipation in conventional medicine without the need for or help of TCM practitioners.
For this pattern of constipation mentioned above, the purgative prescription, composed of drugs that are Warm in nature, would be made according to the theory of TCM. 16 This kind of prescription is mainly made up of drugs with the action of purging and warming the interior of the body. In this six-herb formula of CCH1, Da Huang has known laxative potency 23 due to emodin, which belongs to a family of anthraquinones. As one of the two principal drugs, Ren Shen is used to invigorate the Spleen (gastrointestinal system) and replenish Qi. Gan Jiang is the other principal drug for warming up the Spleen and dispelling Cold. Assisting Gan Jiang in warming up yang-Qi, Zhi Fu Zi and Gan Jiang have the action of warming the interior of the body. Bai Zhu has the effect of strengthening Spleen. Gan Cao can temper the actions of all the other ingredients and also invigorate Qi. Therefore, five of six herbs were formulated to strengthen the energy of yang together with Da Huang serving as purgative drug. 16,17 However, the contribution of each component of CCH1 for therapeutic effect remains to be investigated.
For considerations of ethical concerns and real situations in clinical practice, this study design allowed the primary physician to adjust the dosage of rescue laxative every week until optimal bowel performance was observed. Therefore, the laxative effect of CCH1 probably contributed to the combined effect of the herbal formula and MgO. Also, the therapeutic effects on SBM and RT were improved over time in the placebo group as the amount of MgO increased over time. As a result, the global efficacy assessed by caregivers at the end of the treatment phase had no significant differences between groups in the category of improvement shown to nearly all participants. In addition, because of more MgO prescribed in the placebo group in the beginning of the follow-up phase, there was not enough evidence to evaluate the maintenance effect of CCH1 by the study, and further trial with an appropriate design is needed.
For the residents with multiple co-morbidities in long-term care, frequent AEs or SAEs were predictable during the entire 12-week study period with weekly visits and detailed records. Despite an insignificant difference between the two groups, there were more patients with dermatitis and diarrhea noted in CCH1 group. Based on the theory of TCM, Da Huang has a remarkable effect on inducing defecation, so the prescription and dosage of Da Huang should be gauged to the individual's constitution or pattern diagnosis. 24 In addition, diarrhea and skin eruptions were rare but also reported in ginseng products. 25 Hence, the association of AEs or SAEs with CCH1 or constitution variation needs further large-scale studies.
Additionally, there were some limitations in this study. Objective data from medical records and stool diaries were used for outcome measurements rather than the subjective assessment of symptom score or quality of life, which are not suitable for the participants in this study with potentially impaired cognitive function or poor expression ability. In addition, although older people were the main population in this study, some adults aged 20–65 years were also involved. Therefore, the effect of CCH1 for young and middle-aged adults remains to be investigated.
Conclusions
The effect of CCH1 is promising and may provide a complementary therapy for constipation in long-term care. A properly designed large-scale or comparative study with other laxatives is essential, particularly with regard to concerns about quality of life and cost effectiveness. In addition, the efficacy and safety of CCH1 for the population in the community is needed to be confirmed by another study with subjective outcomes included.
Footnotes
Acknowledgments
This study was funded by National Taiwan University Hospital Yun-Lin Branch (NTUHYL95.S024). The study sponsor did not participate in the study design, data collection, analysis, and interpretation. Prof. Su is the inventor of CCH1 and provided scientific direction to the development of the clinical study. Prof. Lue and Prof. Chiu facilitated planning and operational aspects as well as direct scientific guidance to this study. Dr. Huang planned and conducted large parts of the study, and also wrote the article and interpreted the results. Dr. Lin contributed to writing assistance and manuscript preparation. Prof. Li was the principal statistician for the study. Prof. Lee contributed to the quality control and preparation of the herbal formula in the study.
Disclosure Statement
No competing financial interests exist.