
Abstract
Objectives:
The study objectives were to observe the clinical efficacy of primary massage of twining manipulation with one finger (PMTMOF) versus conventional tuina manipulation for treating muscular torticollis.
Methods:
A randomized, controlled, single-blind method was employed. Patients received either PMTMOF (experimental group, n = 265) or conventional tuina manipulation (control group, n = 235), once a day, 20 minutes each, for 15 days of treatment. After four treatment courses, sternocleidomastoid muscle morphology and size were detected using two-dimensional ultrasonography; sternocleidomastoid muscle blood flow was monitored by color Doppler ultrasonography; and head–neck deflection and range of motion were used to determine total curative effects.
Results:
In the treatment group, 55 patients were cured, 120 patients remarkably responded to the treatment, 75 patients effectively responded, and 15 patients were found to have no response. The total effective response rate to the treatment is 94.34%. In the control group, 15 patients were cured, along with very effective results in 60 patients, effective results in 125 patients, and ineffective results in 35 patients, and the total effective rate is 85.11%. A significant difference in total effective rate was found between experimental and control groups (p < 0.05).
Conclusions:
PMTMOF produced more obvious curative treatment effects in infantile muscular torticollis than conventional tuina manipulation and could effectively shorten treatment time and avoid sequelae due to delayed healing.
Introduction
For treating infantile muscular torticollis, nonsurgical treatments are recommended for infants <12 months of age, such as manipulation, because sternocleidomastoid muscle dragging can enhance the healing rate of nonsurgery treatments. Surgical treatment, an effective method, has been recommended for infants >12 months of age, 10,11 which is an effective method. However, postoperative collapsed sternocleidomastoid muscle on the affected side and neck asymmetry could lead to aesthetic compromises. 12 Based on conventional tuina manipulation for treating infantile muscular torticollis, the present study used a modified method—primary massage of twining manipulation with one finger (PMTMOF)—which involves a smaller contact area, provides faster frequency and stronger penetrating force, and produces better effects in promoting blood flow, removing blood stasis, promoting tissue regeneration, subduing swelling, and alleviating pain. It can also be used to locally treat the sternocleidomastoid muscle and promote development of adjacent muscle. 13 PMTMOF produced more obvious curative treatment effects on infantile muscular torticollis than conventional tuina manipulation and could effectively shorten treatment time and avoid sequelae due to delayed healing.
At present in China, infantile muscular torticollis is primarily treated with Traditional Chinese Medicine. Clinical massage efficacy has been confirmed by clinical practices and is widely accepted. Massage through twining, pressing, rubbing, lifting, and pinching the sternocleidomastoid muscle on the affected side promotes rhythmical contraction and dilatation of muscle blood capillaries, thereby reaching appropriate congestion, accelerating blood circulation, improving nutrient supply of local skin and muscle, promoting metabolism, accelerating back-streaming of blood and lymph fluid and absorption of edema and pathologic products in the focus region, finally relaxing tendons, activating blood circulation, relieving swelling, and disintegrating mass.
Stimulation of neck and back muscles and points through pressure and rubbing promotes muscular inflammation extinction, relaxes tonic muscles, expands peripheral vessels, reduces vessel resistance, dredges channels and collaterals, accelerates qi and blood circulation, disperses swelling mass, and promotes growth and development of neck and adjacent muscles. Neck rotation and lateral flexion drafting smoothes joints, releases ligament and muscle adhesion, and strengthens efficacy of joint motion. Dragging muscle fibers results in fully extended and relaxed sternocleidomastoid muscles, which further extends muscle fibers on the affected side, thereby improving and recovering length of contractural muscle fibers and increasing muscle work capacity and endurance. Releasing muscle hypertonicity, increasing sternocleidomastoid muscle extension, and reducing intramuscular viscosity relaxes tonic muscles and corrects muscular torticollis. Cheng et al. 14 –16 reported that manual stretching is a common method for treating hematomas and muscular torticollis of the sternocleidomastoid muscle. Manual stretching counterbalances the malformation-producing force, and restores physiologic muscle force balance. In addition, twining, pressing, rubbing, lifting, and pinching during manipulative therapy dredges channels and collaterals and opens blood pathways. Repeated stimulation decreases muscle contracture. During repeated manipulative therapy, nonorganized lumps become soft and are absorbed, and organized lumps are lengthened. With gradually strengthened adaptive capacity, the active motion amplitude increases, which accelerates development of sternocleidomastoid muscles, strengthens compensative capacity of other muscles, and finally improves head and neck motion functions.
Compared with surgical treatments and glucocorticoid injection, manipulative treatment exhibits unique advantages. The drawbacks of surgical treatment include collapsed sternocleidomastoid muscle on the affected side following surgery, which results in cosmetic compromises due to an asymmetrical neck. 17 Glucocorticoid exhibits many side-effects closely related to medication dose, time interval, and time of treatment. 18 Manipulative therapy is considered a “green” therapy that is safe and easily accepted by parents, because it does not induce pain or side-effects, and can be performed while the patient is sleeping. Therefore, manipulative therapy is a relatively ideal method for treating infantile muscular torticollis.
Materials and Methods
General data (Table 1)
A total of 500 infant outpatients, who received treatment at the Department of Massage, Linzi District People's Hospital, Zibo City, Shandong Province, China between February 2008 and February 2010, were diagnosed with infantile muscular torticollis using two-dimensional and color Doppler ultrasonography and were included in the present study. Two-dimensional ultrasonography was adapted to superior–inferior diameter, anteroposterior diameter, and left–right diameter of the sternocleidomastoid muscle. Color Doppler ultrasonography showed blood flow of sternocleidomastoid muscle. The patients, comprising 280 males and 220 females, averaged 69.8 days old (range 8–180 days). RandA1.0 (Randomization Adviser 1.0) software was adopted to randomly divide them into two groups: treatment (n = 265) and control (n = 235). In the treatment group, there were 150 males and 115 females, among which 125 were younger than 60 days, 100 patients were between 60 and 120 days, and 40 patients were between 120 and 180 days; 155 patients were spontaneously delivered and 110 patients were uterine-incision delivered; 230 patients were lump type, and 35 patients were atrophy type; 165 patients had the lesion site on the right side, 100 patients had lesion site on the left side; 55 patients had mild infantile muscular torticollis, 150 patients had moderate infantile muscular torticollis, and 60 patients had severe infantile muscular torticollis. In the control group, there were 130 males and 105 females, among which 120 were younger than 60 days, 85 patients were between 60 and 120 days, and 30 patients were between 120 and 180 days; 140 patients were spontaneously delivered and 95 patients were uterine-incision delivered; 200 patients were lump type, and 35 patients were atrophy type; 145 patients had the lesion site on the right side, 90 patients had lesion site on the left side; 50 patients had mild infantile muscular torticollis, 150 patients had moderate infantile muscular torticollis, and 35 patients had severe infantile muscular torticollis. Information collection, record, storage, and analysis were completed by professional personnel, according to single-blind protocol. All participants who were recruited had signed an agreement before joining in this study. Statistical analysis (X2 test) revealed no significant difference between treatment and control groups in terms of gender, age, delivery type, pattern of syndrome, lesion site, and degree of disease prior to therapy (p > 0.05), indicating that the groups were comparable.
Clinical diagnosis criteria
Clinical diagnostic standards were used for diagnosis of infantile muscular torticollis. Based on previously described symptom improvements, 19 the diagnostic criteria were as follows: (1) malposition, circular umbilical cord, oligohydramnios, forced left lateral position, dystocia, excessively long birth process; (2) head tilting toward affected side, maxillofacial region rotating toward the intact side; (3) able to touch orbicular-ovate or strip-shaped lumps with soft or hard texture in sternocleidomastoid muscle on the affected side; (4) affected side exhibited symptoms, including face hypoevolutism, a small contour, a tiny rima oculi, slightly lower auricle apex, head and neck tilting toward intact side, motion limitations, upper lifted shoulder joint, cervical vertebrae curved toward intact side, and upper thoracic vertebrae curved toward affected side; (5) two-dimensional and color Doppler ultrasonography were first-choice diagnosis methods; (6) and radiograph of cervical vertebrae was a secondary examination.
Classification criteria of syndrome patterns
Lump type: Able to feel lumps in the sternocleidomastoid muscle on the affected side; ultrasonography examination showed abnormal sternocleidomastoid muscle on the affected side, suggesting the presence of lumps.
Atrophy type: No lumps felt in the sternocleidomastoid muscle on the affected side; ultrasonography examination of the same segments, anteroposterior diameter of sternocleidomastoid muscle on the intact side: anteroposterior diameter of sternocleidomastoid muscle on the affected side ≥0.1 cm.
Classification criteria of disease severity
Mild: Superior–inferior diameter of lump ≤2.0 cm, as determined by ultrasonography examination, as well as atrophy type.
Moderate: Superior–inferior diameter of lump = 2.0–3.0 cm, as determined by ultrasonography examination.
Severe: Superior–inferior diameter of lump ≥2.0–3.0 cm.
Technology roadmap (Fig. 1)
Therapeutic methods
Treatment group
PMTMOF was used. (1) Manipulation of sternocleidomastoid muscle: The sternocleidomastoid muscle was divided into three segments for manipulation: papilla end (upper segment), clavicle end (inferior segment), and venter musculi (middle segment). The patients were placed in a bed in a supine position. The physician, who was seated on the affected side of the infant, slightly rotated the head and neck to the intact side to fully expose the sternocleidomastoid muscle on the affected side. The patient head was stabilized to facilitate persistent manipulation. An appropriate amount of diclofenac diethylamine emulgel (Novartis) was spread on the sternocleidomastoid muscle on the affected side to lubricate the skin and protect the muscle surface. Manipulation involving the thumb tip of the right hand was performed in the direction vertical to the muscle fiber of the sternocleidomastoid muscle. First, the upper segment of sternocleidomastoid muscle was massaged for 5 minutes using PMTMOF, then the middle segment was massaged for 10 minutes, and subsequently the inferior segment for 5 minutes. The entire manipulation lasted for 20 minutes with the patient in a recumbent position (atrophy type for 15 minutes). The pendular movement frequency was 220–250 times/min. (2) Manipulation of other muscles at neck: The infant patient was maintained in an upright position, with its back to the physician and the head stabilized. Several regions behind the neck were massaged, 1 minute at each region, including the trapezius muscle, levator scapulae muscle, lateral cervical muscle, musculus scalenus anterior, middle, and posterior. Several points including Fengchi (GB 20), Dazhui (DU 14), Fengmen (BL 12), and Jianjing (GB 21), as well as post aurem bone prominence, were massaged for 1 minute each. The infant faced the physician, and Tianchuang (SI 16) and Tianrong (SI 17) points on the affected side were massaged for 1 minute each. The sternocleidomastoid muscle on the affected side was lifted and massaged for 1 minute. The sternocleidomastoid muscle was lifted as much as possible to separate it from lower layer adhesion. Lifting, rubbing, and twisting the related muscles are necessary for treating atrophic muscular torticollis to accelerate local blood supply and promote muscle development. (3) Cervical part rotation and lateral flexion extension: The infant patient was maintained in an upright position facing the physician, with the shoulders stabilized. The physician held the mandibular region and posterior occipital region to rotate toward left and right along the vertical axis of the cervical vertebrae for a total of 15 times, which allowed for fully relaxed neck muscles. One (1) hand held the shoulder on the affected side and the other hand held the vertex of the head. Drafting toward the intact side was performed using gentle to heavy manipulation, and small to large amplitude. The sternocleidomastoid muscle tendon on the affected side was gradually elongated. During the drafting treatment, sudden flexion or clicking of the sternocleidomastoid muscle was observed. The rotation range was within 30°, and <1 month of age is a high-risk factor. Sudden flexion is often accompanied by contusion and increased range-of-motion of neck, which is likely to be due to muscle rupture. 20 For each of the abovementioned treatments, massage was performed once a day for 30 minutes each over a 15-day treatment course.
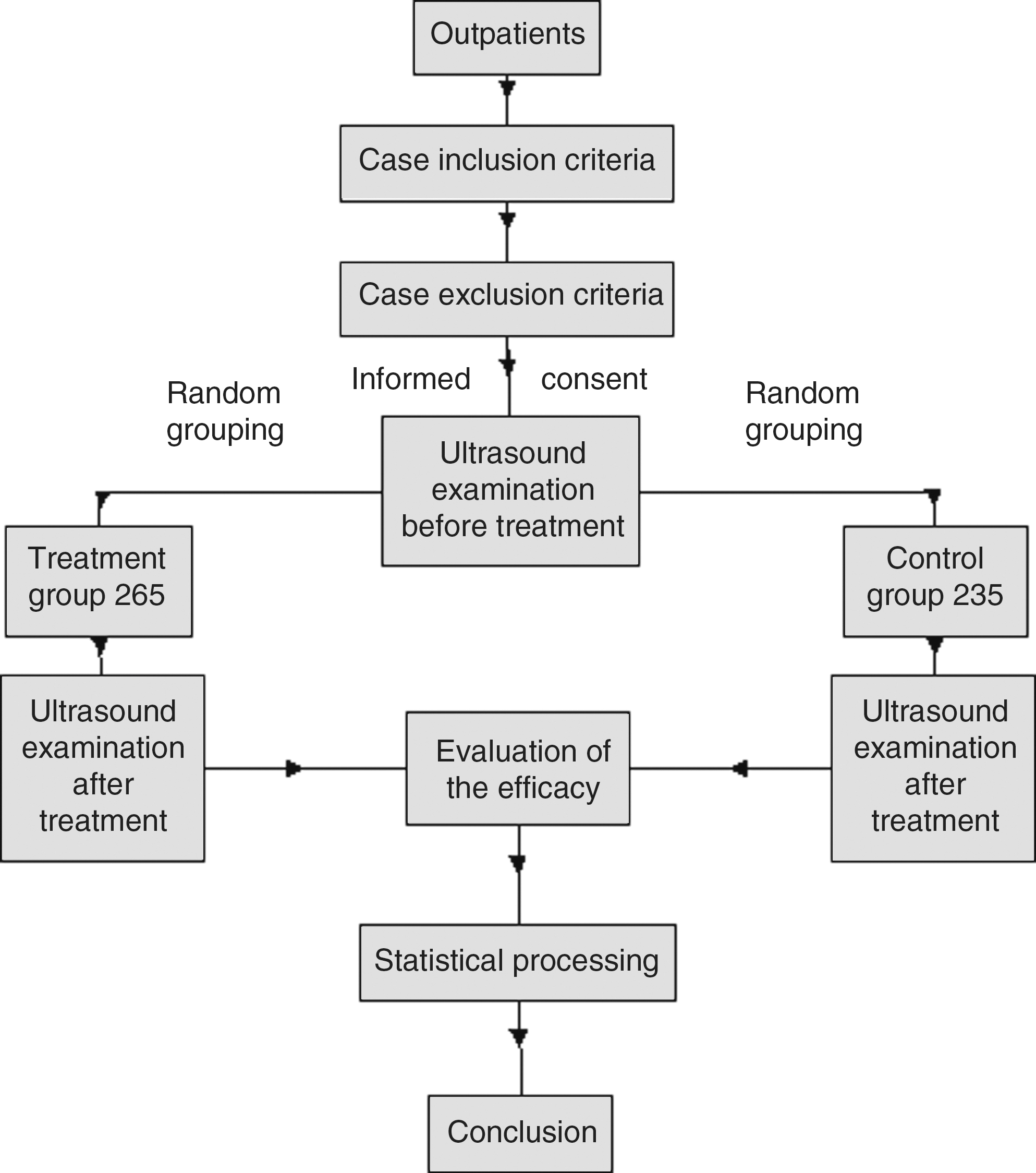
Technology roadmap.
Control group
Conventional tuina massage was primarily used. The infant was placed in a lateral position, with the affected side upward. An appropriate amount of diclofenac diethylamine emulgel (Novartis) was spread on the sternocleidomastoid muscle on the affected side to lubricate the skin and protect the muscle surface. The sternocleidomastoid muscle was massaged using the thumb surface for 6 minutes, and then it was lifted and pinched using the thumb and index finger for 5 minutes. The Fengchi (GB 20), Fengfu (Du16), Tianchuang (SI 16), and Tianrong (SI 17) points were massaged using the thumb for 1 minute each. Subsequently, bilateral Fengmen (BL 12), Feishu (BL13), and Jueyinshu (BL14) points were pushed using the thumbs of both hands for 1 minute at each point. Similarly, one hand held the shoulder of the affected side and the other hand held the vertex of the head. Extension toward the intact side was performed using gentle-to-heavy manipulation and small-to-large amplitude. The sternocleidomastoid muscle tendon of the affected side was gradually elongated. For each of the abovementioned actions, massage was performed once a day for 20 minutes each over a 15-day treatment course.
Clinical observational indices and detection time
A color Doppler ultrasonograph (Voluson 730, GE, USA), using a probe frequency of 2.5–7.5 MHz, was utilized. The superior–inferior diameter, anteroposterior diameter, and left–right diameter of the sternocleidomastoid muscle were measured using two-dimensional ultrasonography. Blood flow of the sternocleidomastoid muscle was monitored by color Doppler ultrasonography. Each index was detected prior to treatment, as well as after four treatment courses.
Curative effect assessment criteria
An obvious change in clinical practice is the softening and disappearing of the sternocleidomastoid muscle lump, and increase of blood flow, which were observed by means of two-dimensional ultrasonography and color Doppler ultrasonography. Ultrasound determination was completed by a professional operator, according to single-blind protocol. The following list criteria for curative effects.
Cured: Head and neck deflection disappeared, and head motion was flexible. Two-dimensional ultrasonography exhibited similar superior–inferior diameter, anteroposterior diameter, and left–right diameter of the sternocleidomastoid muscle between the affected and intact sides. Color Doppler ultrasonography showed abundant blood flow of the sternocleidomastoid muscle.
Very effective response: Head and neck deflection basically disappeared, and head motion was relatively flexible; two-dimensional ultrasonography exhibited a ≥50% reduction of the superior–inferior diameter and left–right diameter of the sternocleidomastoid muscle (lump type) or a ≥50% increase in anteroposterior diameter (atrophy type); color Doppler ultrasonography showed abundant blood flow of the sternocleidomastoid muscle.
Effective response: Head and neck deflection was alleviated, and head motion was poorly flexible; two-dimensional ultrasonography showed a ≥25% reduction in superior–inferior diameter and left–right diameter of the sternocleidomastoid muscle (lump type) or a ≥25% increase in anteroposterior diameter (atrophy type); color Doppler ultrasonography showed relatively abundant blood flow of sternocleidomastoid muscle.
Ineffective: Head and neck deflection were not improved; two-dimensional ultrasonography showed a <25% reduction in superior–inferior diameter and left–right diameter of the sternocleidomastoid muscle (lump type) or <25% increase in anteroposterior diameter (atrophy type); color Doppler ultrasonography showed relatively abundant blood flow of the sternocleidomastoid muscle.
Statistical analysis
The χ2 test was employed for enumeration data and Ridit analysis was used for clinical ranked data. All data were statistically processed using SAS software. A level of p < 0.05 was considered statistically significant.
Results
Comparison of clinical efficacy between treatment and control groups (Table 2)
After four treatment courses, curative results were observed in 55 patients (20.75%), very effective results in 120 (45.28%), effective results in 75 (28.30%), and ineffective results in 15 (5.66%), with a total effective rate of 94.33% in the treatment group. In the control groups, curative results were observed in 15 (6.38%), very effective results in 60 (25.53%), effective results in 125 (53.19%), and ineffective results in 35 (14.89%), with a total effective rate of 85.11%. There was a significant difference in total effective rate between experimental and control groups (U = 7.7434, p < 0.05). No patient was rejected or treatment-terminated, and no adverse reactions were observed.
Comparison of curative efficacy between different syndrome pattern patients (Table 3)
Factors that possibly influenced curative efficacy of infant patients with different syndrome patterns in the treatment group were analyzed. Of 230 lump-type patients, 35 patients (15.22%) were cured, very effective results were observed in 110 patients (47.83%), effective results in 70 patients (30.43%), and ineffective results in 15 patients (6.52%), with a total effective rate of 93.48%. Of 35 atrophy patients, 20 patients (57.14%) were cured, very effective results were observed in 10 patients (28.57%), and effective results in 5 patients (14.29%), with a total effective rate of 100.00%. Statistical analysis showed a significant difference in curative efficacy between different syndrome patterns in the experimental group (U = 3.6702, p < 0.05). Clinical efficacy was better in atrophy-type patients than in lump-type patients.
Comparison of curative efficacy in patients with different disease severities (Table 4)
Factors that possibly influenced curative efficacy of patients with different degrees of muscular torticollis in the treatment group were analyzed. Of 55 patients with mild muscular torticollis, 35 patients (63.64%) were cured and 20 patients (36.36%) had remarkable effects, with a total effective rate of 100.00%. Of 150 moderate infantile muscular torticollis patients, 18 patients (12.00%) were cured, very effective results were observed in 90 patients (60.00%), and effective results in 42 patients (28.00%), with a total effective rate of 100.00%. Of 60 patients with severe muscular torticollis, effective results were observed in 38 patients (63.33%) and ineffective results in 22 patients (36.67%), with a total effective rate of 63.33%. There was a significant difference in clinical efficacy among patients with different degrees of muscular torticollis (χ2 = 137.8950, p < 0.05). Better clinical efficacy was observed in patients with mild muscular torticollis.
Comparison of clinical efficacy in patients with varying ages (Table 5)
Factors that possibly influenced curative efficacy of patients with different ages were analyzed. Of 125 patients <2 months of age, 43 patients (34.40%) were cured and 82 patients (65.60%) had very effective results, with a total effective rate of 100.00%. Of 100 patients aged 2–4 months, 12 patients (12.00%) patients were cured, very effective results were observed in 33 patients (33.00%), and effective results in 55 patients (55.00%), with a total effective rate of 100.00%. Of 40 patients aged 4–6 months, very effective results were observed in 5 patients (12.50%), effective results in 20 patients (50.00%), and ineffective results in 15 patients (37.50%), with a total effective rate of 62.50%. There was a significant difference in clinical efficacy among patients with different ages (χ2 = 108.6387, p < 0.05). Better clinical efficacy was observed in younger patients.
Discussion
All 500 infant patients with muscular torticollis and their mothers were studied. During pregnancy, women with significantly longer periods in a left sleeping position resulted in more severe muscular torticollis in newborns. Obstetricians are strongly urged to inform pregnant women that the left sleeping position is better, but it should be emphasized that a persistent left recumbent position could increase the morbidity rate of muscular torticollis. Age in pregnant women could lead to more severe muscular torticollis in newborns. A fetal malposition that is not corrected in time could lead to more severe infantile muscular torticollis. Infants with a circular umbilical cord suffer more easily from muscular torticollis.
Conclusions
PMTMOF produced more evident curative treatment effects in infantile muscular torticollis than conventional tuina manipulation did, and effectively shortened treatment time and avoided sequelae caused by delayed healing.
Footnotes
Disclosure Statement
No competing financial interests exist.