
Abstract
Objectives:
Users of Traditional Chinese Medicine (CM) and biomedicine (BM) are commonly assumed to belong to two different groups in most of the related literature. The purpose of this article is to compare the characteristics of those who use both CM and BM for the same illness (CBMS) with those who solely use BM (BMS).
Methods:
Starting with a systematic sampling of 200,000 patients from a database of the Taiwan National Health Insurance program for the year 1999, the data were organized so that those who visited hospitals and clinics more than twice for the same illness were selected. In total, there were 96,872 (60%) BM users and 30,099 (19%) CBM users. The χ2 test and mean test were applied to compare the differences in use between the above two subgroups. Logistic regression was used to calculate odds ratios of demographic variables and disease types.
Results:
Compared to the group using BM for the same illness (BMS), there were more females in the group using both CM and BM for the same illness (CBMS) (p < 0.0001). Most of the subjects in the CBMS group were aged 25–49 years (p < 0.0001). The mean number of total visits was higher for CBMS (16.33) than for BMS (13.71) (p < 0.0001). For both groups, the mean number of visits for females was higher than for males (p < 0.0001). Furthermore, the mean cost per visit was significantly lower for CBMS (519.58 New Taiwan Dollar [NTD]) than for BMS (582.37 NTD). Among the top eight major disease categories of patients in the two subgroups, disease of the respiratory system was the most common primary indication in both CBMS and BMS. However, diseases of the musculoskeletal system and injury showed the highest incidences in CBMS when compared with BMS.
Conclusions:
Alternative medicinal treatment has become increasingly popular in recent years. Providing integrated CM and BM service in one medical facility might greatly benefit patients.
Introduction
Medical plurality is not new. An early study examines a case in Nigeria where some people prefer a single medical treatment system for a specific disease, whereas others prefer more pluralistic medical treatment systems, that is, utilizing both traditional medicine and BM for the same illness. These choices may be affected by particular characteristics of patients and are significantly related to sex, religion, and residence. 11 A similar situation is more likely to exist among CM users who also seek BM for the same illness. The pattern of plural medical treatments was analyzed in this study, using population-based data from a national health insurance program in Taiwan.
Methods
Data
In 1995, the Taiwan National Health Insurance (NHI) program was established. NHI not only insures more than 99% of the 23 million citizens in Taiwan, but also covers modern BM and CM. NHI collects insured patients' information, which includes the number of visits, sex, birth, and medical history, in the National Health Insurance Research Database (NHIRD), forming the largest and most representative nationwide population-based dataset in the world. The research using NHIRD data to analyze the different ways in which patients access their medical care provides alternative views when compared to other studies that rely on questionnaires in terms of completeness.
The data in this study were obtained from a systematic sampling of the NHIRD with 200,000 patients in 1999. The available items are medical claims, numbers of visits, diagnostic codes, patient characteristics of date of birth and sex, health care facility classifications, and areas. However, information on income and residence is not available. There are four categories of health care facilities: academic medical center, metropolitan hospital, local community hospital, and physician clinic. For simplicity, health care facilities were reclassified into only two categories: hospitals and clinics. The former includes academic medical centers, metropolitan hospitals, and local community hospitals while the latter includes physician clinics, which are facilities with no beds. In line with the research focus in this study, the data on dentistry and home care, as well as that of patients lacking basic information such as sex or age and foreigners, were excluded. Ultimately, this article includes the data from 161,877 patients with 2,420,479 ambulatory visits.
Study sample
In order to examine the characteristics of patients seeking specific treatment method for the same illness, the total sample (all patients) first was divided into three subsamples: patients who use both CM and BM (Sample CBM), patients who only use BM (Sample BM), and patients who only use CM (Sample CM), as shown in Figure 1.
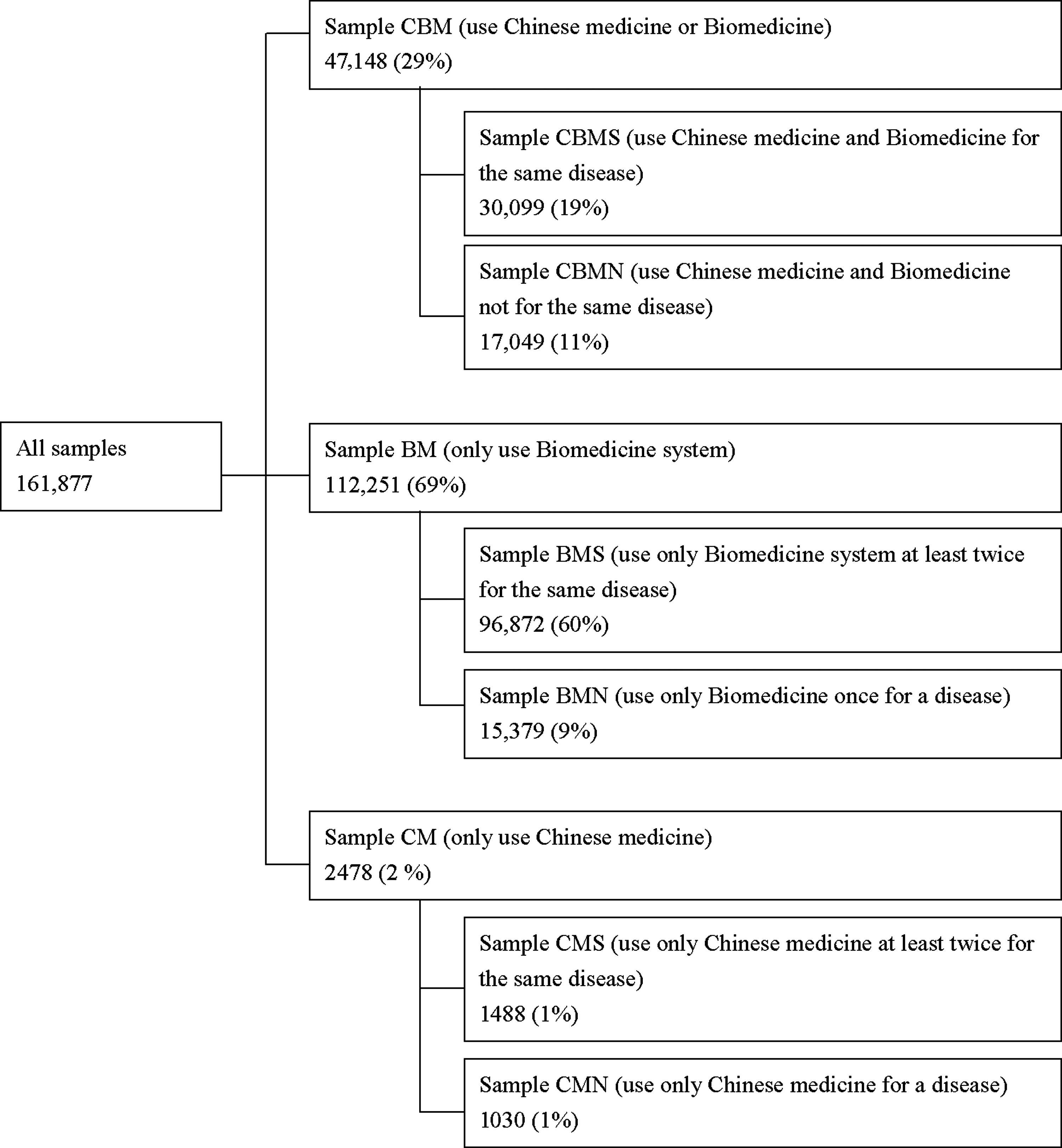
Data distribution of different medical systems in 1999.
Among the patients in our sample, an insignificant proportion (2478, 2%) use only CM; these samples were ignored thereafter. There were 112,251 (69%) who used only BM and 47,148 (29%) who used CBM. Since the focus of this study is to examine the characteristics of those who use plural medical systems, patients seeking medical care at least two times for the same illness in the sample period were selected. In other words, for the patients in Sample CBM, there are two different subgroups: one subgroup who always pursues different medical systems for the same illness (CBMS), and another group who does not combine the systems (CBMN), but instead selects BM and CM for different diseases. It is worth noting that to compare the patients' behavior of seeking medical care service between different groups in a consistent way, the data were also restricted to include patients visiting physicians at least two times in Sample BMS. In total, there are 96,872 (60%) BMS patients and 30,099 (19%) CBMS patients, respectively.
To account for “the same illness,” all diagnoses of ambulatory visits were determined by the index of the International Classification of Diseases (ICD-9-CM), which is used by medical facilities for both BM and CM. For simplicity, all diagnoses were combined into 18 types. The most frequent diagnostic categories among all samples are diseases of the respiratory system, followed by diseases of the nervous system, digestive system, the skin and subcutaneous tissue, the musculoskeletal system, and connective tissue, and so on.
Statistical analysis
To compare the differences in demographics of patients between CBMS and BMS, the χ2 test is applied. For comparisons of frequency of hospital and clinic visits, the mean test is used. In addition, logistic regression is utilized to estimate the marginal effect of demographic variables and disease types on the use of CBMS and BMS. The results are illustrated in terms of odds ratios. All of the procedures are performed using SAS software.
Results
Figure 2 illustrates the proportions of patients in samples of CBMS and BMS by sex. There is a higher proportion of females (59.2%) than males (40.8%) in the CBMS group. In the BMS group, the proportions are close to equal: 50.6% for females and 49.4% for males. Figure 3 indicates the differences in treatment methods between CBMS and BMS across five age groups. About 45% of CBMS and 35% of BMS patients are between 25 and 49 years of age. The majority of the CBMS subjects are aged 25–49, followed by those aged 13–24. Since not all of the health care facilities provide CM services, the places where patients seek CM are compared. There are two facility types: hospitals and clinics. Patients might choose a hospital for health care due to the specialty of physicians, as well as the availability of a wide range of equipment. On the other hand, they might choose clinics because of the less costly copayments and proximity to their residence. It is also common for patients to base this decision on the type or severity of disease from which they are suffering. It is worth noting that the copayments are different between hospitals and clinics under NHI. Figure 4 illustrates the proportions of patients using only hospitals or only clinics. We found that a greater proportion of patients in the CBMS group (55.1%) used both hospitals and clinics when compared with BMS group (44.6%).
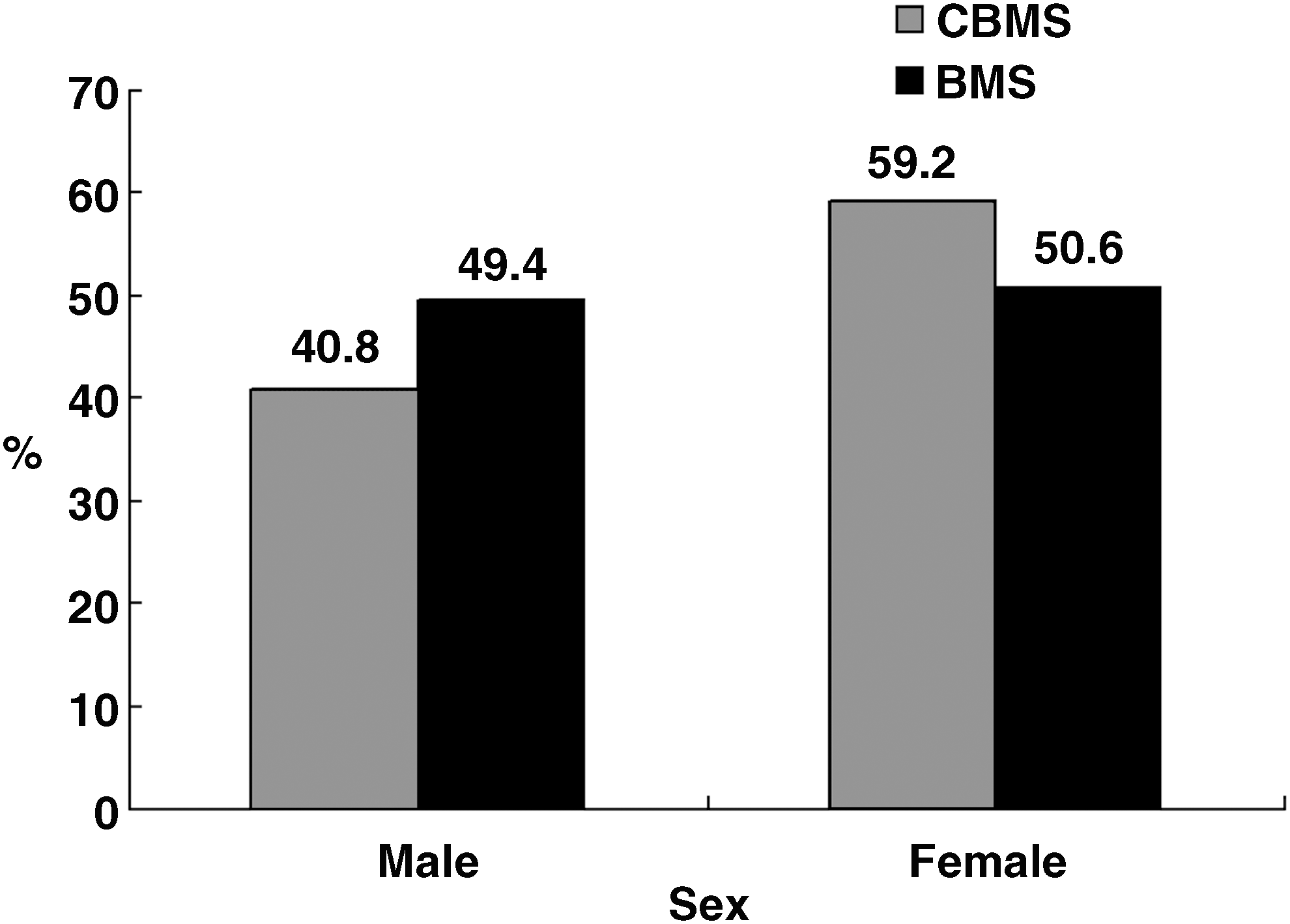
Proportion of patients by sex among subsamples. CBMS, Traditional Chinese Medicine and biomedicine for the same illness; BMS, biomedicine for the same illness.
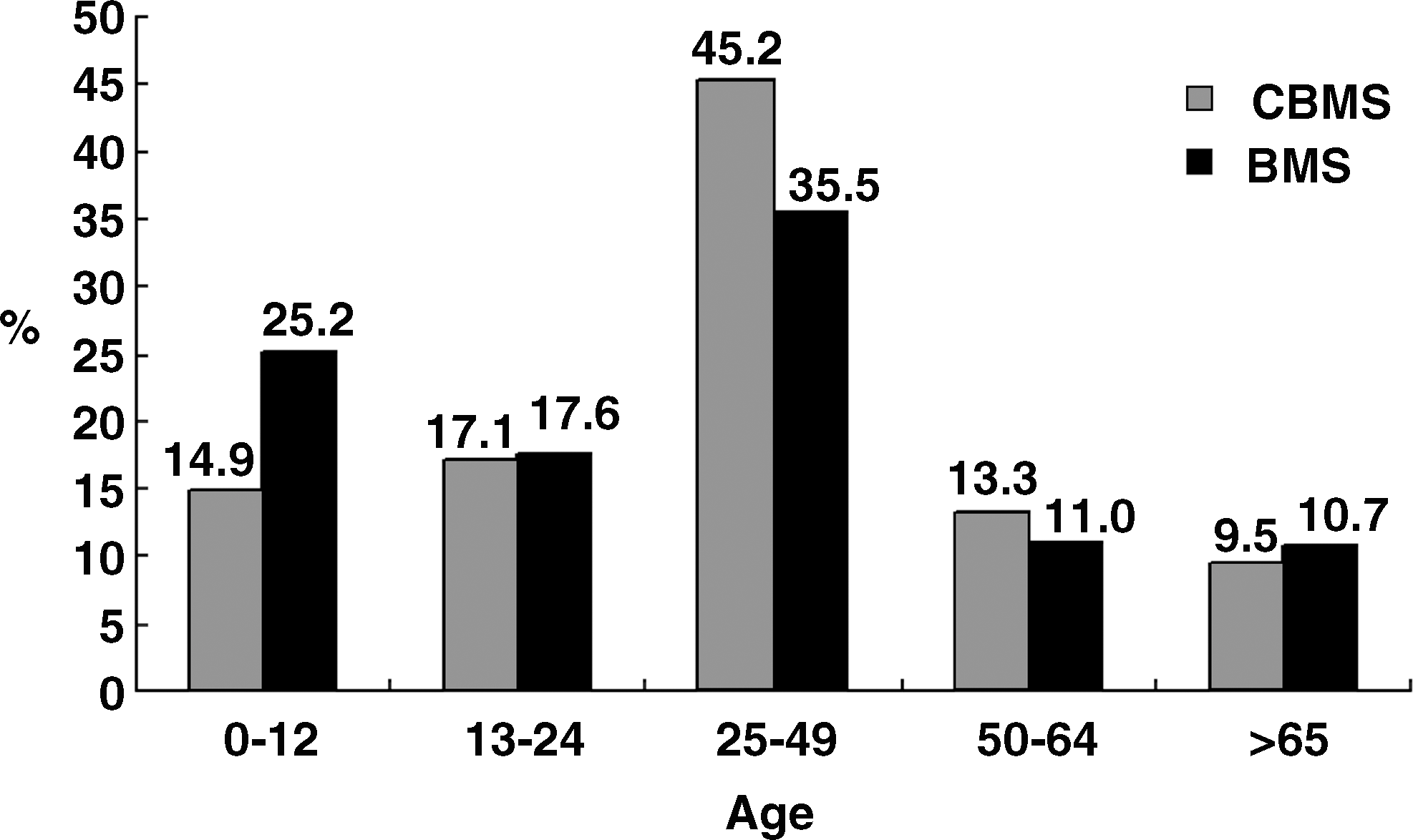
Proportion of patients by five age classes among subsamples. CBMS, Traditional Chinese Medicine and biomedicine for the same illness; BMS, biomedicine for the same illness.
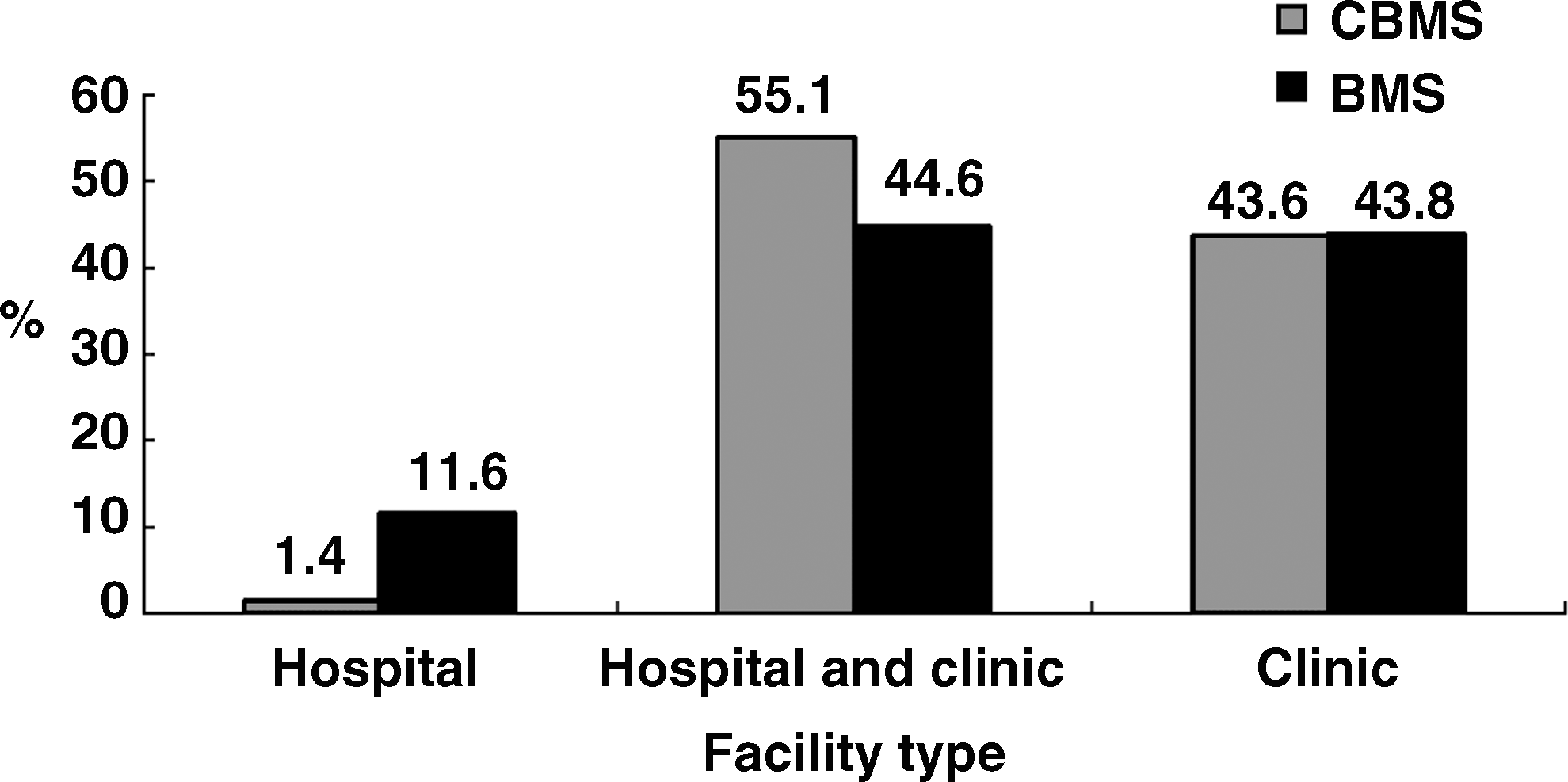
Proportions of patients by facility type among subsamples. CBMS, Traditional Chinese Medicine and biomedicine for the same illness; BMS, biomedicine for the same illness.
In Table 1, Panel A demonstrates the comparisons of cohort distributions of sex, age, and facility types. Compared to BMS, females (p < 0.0001), those aged 25 to 49 (p < 0.0001), and those who visited both hospital and clinical facilities (p < 0.0001) tend to prefer CBMS. In addition, there is a smaller proportion of children (aged 0–12) in the CBMS group (14.9%) than in the BMS group (25.2%). Panel B shows that the mean number of total visits is higher for the CBMS (24.25) than for the BMS group (14.79) (p < 0.0001). When considering all illnesses, the mean number of visits for females is higher than for males (p < 0.0001). The visits in Panel B were not limited to the same illness. Since people might seek CM for one disease, but BM for another, those visits for different diseases are excluded to further analyze the use difference between CBM and BM. Panel C indicates that the mean visits for CBMS and BMS for the same disease are 16.33 and 13.71, respectively. The mean values are significantly different (p < 0.0001). The huge drop in mean visits for CBMS from 24.25 (not necessarily for the same disease) to 16.33 (definitely for the same disease) reveals that patients in sample CBMS prefer using CM for various diseases.
SD, standard deviation.
In Panel D, we calculate the mean costs of each visit for the same disease, which were 519.58 New Taiwan Dollar (NTD) and 582.37 NTD for CBMS and BMS, respectively. The mean cost is significantly lower for CBMS than for BMS. In addition, the standard deviation is also smaller for CBMS (664.01 NTD versus 1,349.10 NTD).
Figure 5 shows the average number of visits by age and sex of patients. In general, the average number of visits for patients is U-shaped, suggesting that the average number of visits is higher for patients both below 7 and over 30 years of age. For each level of age, regardless of sex, the average number of visits of the CBMS group is higher that of the BMS group. For most age levels, females have a higher average numbers of visits than males.

Trends in mean visits by age among subsamples. CBMS, Traditional Chinese Medicine and biomedicine for the same illness; BMS, biomedicine for the same illness.
To further understand the composition of visits for CBMS, we list the ratios of CM and BM used by patients of CBMS in Table 2, in which BM accounts for 65% of the visits and CM for 35%. The share of costs for each visit is even higher for BM (70%) than for CM (30%).
Table 3 reveals the top eight major disease categories for patients using CBMS and BMS. In terms of the ranking by visits, diseases of the respiratory system is the prevalent category of disease for which patients seek treatment in CBMS and BMS groups; the ratios are 35.71% and 45.63%, respectively. The second most prevalent category for CBMS is diseases of the musculoskeletal system, which accounts for 15.41% of total patients. In stark contrast, however, this disease ranks seventh in Sample BMS, dropping to 5.69%. It is interesting to note that the diseases of nervous system and sense organs rank as second in Sample BMS, accounting for 8.07% of patients, but ranks seventh in CBMS, accounting for a mere 3.01% of patients. A similar situation of an opposing trend between CBMS and BMS also appears for injuries and diseases of the circulatory system. For injuries, a relatively higher ratio (8.99%) of patients seeks CBMS, while a small ratio (3.74%) seeks BMS. The diseases of the circulatory system reveal a reversed trend in that the ratios are 2.91% and 6.08% for CBMS and BMS, respectively. Other diseases such as those of the digestive system, the genitourinary system, and the skin and subcutaneous tissue have similar patterns between CBMS and BMS.
Top eight diagnoses included more than 80% of all visits among all samples.
CBMS, those who use both Traditional Chinese Medicine and biomedicine (BM) for the same illness; BMS, those who solely use BM; NP, number of patients.
Table 4 illustrates the adjusted odds ratios and 95% confidence intervals for the demographic characteristics and diseases associated with the patients of CBMS relative to patients of BMS. Females (1.29) have higher odds of using CBM than males (1.0). The odds of using CBMS are the highest for those aged 25–49 (1.01). Compared to patients who do not demonstrate a specific disease (1.00), for those who also choose CBMS based on their specific disease, the adjusted odds ratios for the specific diseases, in decreasing order are: symptoms, signs, and ill-defined conditions (3.31), musculoskeletal system and connective tissue (3.21), injury (2.68), digestive system (1.52), genitourinary system (1.44), congenital anomalies (1.23), skin and subcutaneous tissue (1.16), and poisoning (1.13). The odds ratios of other diseases such as certain conditions originating in the perinatal period, complications of pregnancy, and so on where patients prefer BM, are not greater than 0.71.
Adjusted odds ratio (95% confidence interval).
CBMS, Traditional Chinese Medicine and biomedicine for the same illness; BMS, biomedicine for the same illness.
It is worth noting that patients might not visit hospitals and clinics for only one disease. We plot the distribution of numbers of diseases for CBMS and BMS in Figure 6. The most frequent numbers of diseases are three and two for CBMS and BMS, respectively.
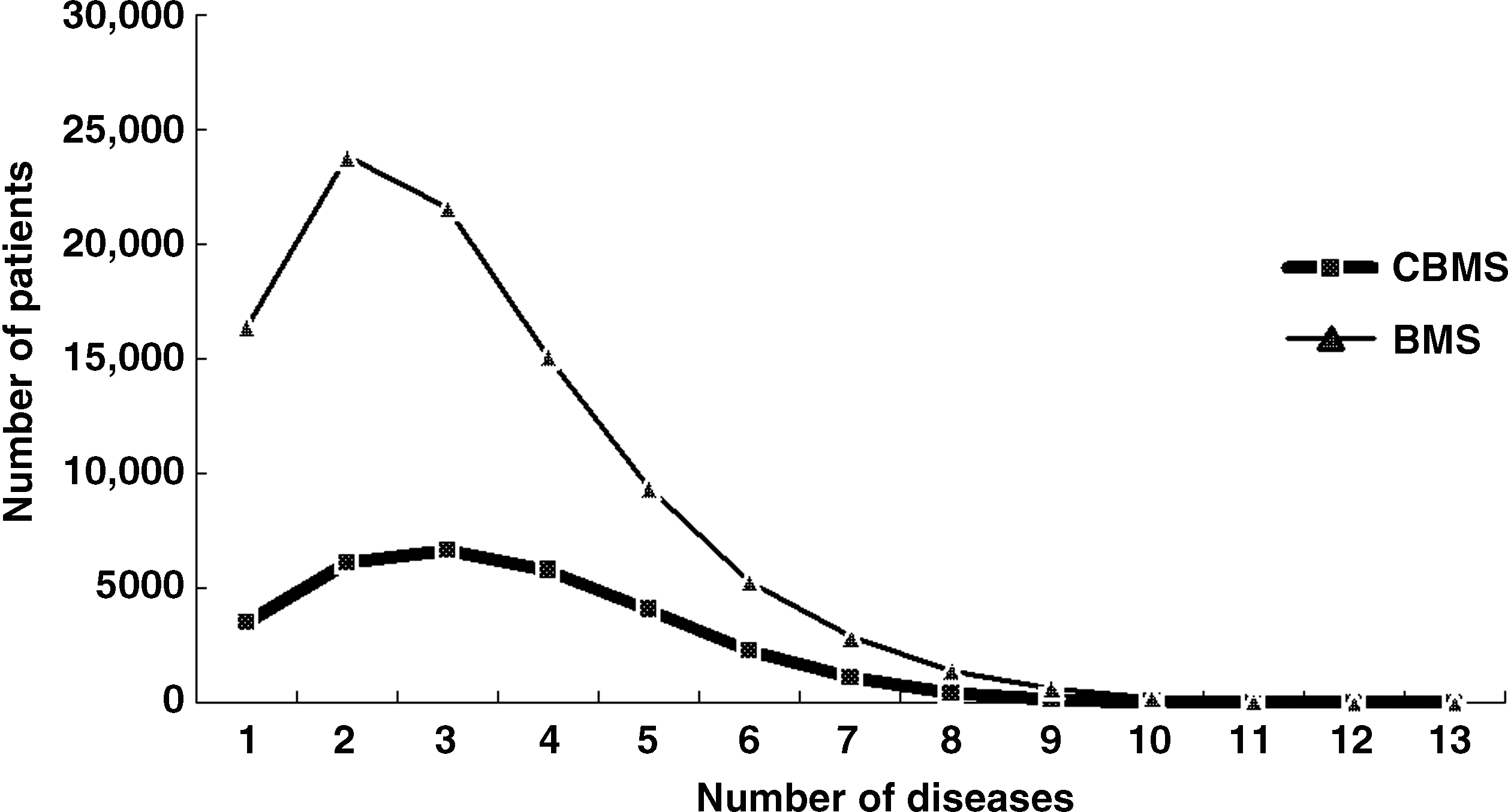
The distributions of number of diseases for Traditional Chinese Medicine and biomedicine for the same illness (CBMS) and biomedicine for the same illness (BMS).
Discussion
While most of the previous literature discusses the use of CM and BM separately, we provide an analysis of the use of CBM versus BM for the same illness. Regarding the role of sex, female patients have a relatively higher tendency to use CBMS, which is similar to previous studies on CM users. 9,10 In addition, middle-aged (ages 25–49) patients are more likely to use CBMS. These results are consistent with the findings of a recent systematic study that reviewed 110 articles that had the same observations on the use of CAM. 12
CM is considered to be cost-effective, compared with BM. 13 Theoretically, the cost of plural medicine, CBM that combines CM and BM, still has a lower cost than BM. The evidence in the above section supports this view in that the mean cost per visit of CBMS (519.58 NTD) is lower than that of BMS (582.37 NTD) (p < 0.0001). It is interesting to note that among those who use CBMS, the majority of the visits (65%) pertain to BM, whereas CM accounts for only 35%. Under this situation, the discrepancy between mean cost per visit is even larger: 604.39 NTD for BM and 465.59 NTD for CM, in Table 2. It seems that CM plays a complementary role in CBM where BM mostly dominates the health care field.
To understand on what occasion CBM will be used, Tables 3 and 4 provide seemingly opposite results and deserve further explanation. Disease of the respiratory system is the most common diagnosis for patients in both CBMS (35.71%) and BMS (46.63%) groups (Table 3). The proportions of patients who visit hospitals or clinics due to this disease are far higher than those of the second ranking disease for CBMS (15.41%) and BMS (8.07). Since odds ratios reveal the relative visiting probability between different health care systems (CBM versus BM), the odds of diseases of the respiratory system for CBMS is small (0.57, CI: 0.55–0.59, p < 0.001) despite the high ratio of use. The second most frequent diagnosis in sample CBMS is diseases of the musculoskeletal system and connective tissue, which has high odds of 3.21, indicating relatively higher use in CBMS than in BMS. In fact, when diseases cannot be very accurately classified, such as symptoms, signs, and ill-defined conditions category, the highest odds of patients preferring CBMS (3.31) is found. Previous studies confirm that CM is a popular treatment for chronic fatigue syndrome for a long time, which is closely related to muscle pain and symptoms. 14 The odds for musculoskeletal system and symptoms, signs, and ill-defined conditions reflect this.
CM is known for being natural, with few adverse effects and is more psychologically acceptable. 15 In our study, 19% of the patients seek CM and BM for the same illness while placing emphasis on BM. Providing an integrated service of CM and BM in one medical facility might greatly benefit patients of this sort. Based on the existing studies, both patients and doctors are willing to try such an integrated medical system. 16,17 Of course, some pilot exploration and experiments are needed before full integration. 18 Most importantly, establishing a solid educational curriculum and training programs to adopt the integrated system of medical care is a necessity.
Limitations
Findings from this database analysis should be interpreted cautiously due to several limitations. First, although CM and BM doctors all adopt the International Classification of Diseases Table (ICD-9) for NHI payment claims, this does not mean that CM and BM doctors have the same viewpoint of diseases. BM doctors have subspecialties but CM doctors do not. CM doctors are trained in major biomedical courses, but on the contrary, BM doctors are not trained in Chinese medical courses in medical school. Second, we do not know about the differences in effectiveness of these two kinds of treatment (CM and BM) and the reasons why patients choose CM and BM simultaneously. Such information is not available in the claims database from NHI. Third, several kinds of CAM, except CM, are not covered under NHI. Patients should pay out-of-pocket by themselves and thus these data are not included in the database analyzed here. Finally, the method used in this study is not face-to-face interviewing, nor questionnaire; thus, demographic features such as educational levels, incomes, health status, marital status, belief system, attitude toward CM and BM, and their medical seeking behaviors for detailed exploration cannot be obtained. Therefore, researchers may consider linking another database including important demographic features in the future studies.
Footnotes
Acknowledgments
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
Disclosure Statement
No competing financial interests exist.