
Abstract
Objectives:
Acupuncture has been gaining popularity among practitioners of modern medicine as an alternative and complementary treatment. However, the mechanism of its therapeutic effect still remains uncertain. The present study chose the GV20 acupoint to evaluate acupoint effectiveness, hypothesizing that its stimulation induces cerebrovascular responses.
Design and setting:
The effects of GV20 acupuncture treatment on middle cerebral artery (MCA) and anterior cerebral artery (ACA) blood flow velocities, and CO2 reactivity during hypocapnia were evaluated in 10 healthy male subjects (mean age 25.6 ± 0.8 years). Measurements were done at rest and during hypocapnia, and were repeated four times each at different cerebral artery territories with an interval of 1 week. MCA and ACA blood flow velocities were measured with a transcranial Doppler flowmeter. Blood flow velocity was corrected to 40 mm Hg of end-tidal CO2 partial pressure (PETCO2), and was expressed as CV40. CO2 reactivity was measured as percent change in mean blood flow velocity/mm Hg PETCO2.
Results:
Mean MCA and ACA blood flow velocities at rest, CV40, and CO2 reactivity during hypocapnia increased significantly after GV20 acupuncture treatment, whereas mean arterial blood pressure and pulse rate at rest did not change significantly. The increases in MCA and ACA blood flow velocity were associated with improved CO2 reactivity after GV20 acupuncture treatment.
Conclusions:
The data suggest that GV20 acupuncture treatment increases cerebral blood flow. The results of this small-scale study provide preliminary evidence for acupuncture effectiveness.
Introduction
Recently, acupuncture has gained popularity among practitioners of modern medicine as an alternative and complementary treatment. According to the theory of Oriental medicine, each acupoint has a functional specificity; specific acupoints are carefully selected when acupuncture is used to treat disorders. 3,4 In particular, the Bai-Hui (GV20) acupoint is used to treat headache, dizziness, dysarthria, and stroke. 3,4 The present study chose the GV20 acupoint to evaluate acupoint effectiveness, hypothesizing that its stimulation induces cerebrovascular responses.
Studies conducted using TCD have provided evidence of the efficacy of acupuncture and herbal medicine treatments, 5 –7 but comparative data concerning acupuncture and herbal medicine treatment are scant.
In the present study, changes of hyperventilation-induced carbon dioxide reactivity and corrected blood flow velocities at 40 mm Hg of the middle cerebral artery (MCA) and anterior cerebral artery (ACA) were assessed in 10 healthy young male volunteers. The results of this small-scale study provide preliminary evidence for acupuncture effectiveness.
Materials and Methods
Ten (10) healthy male volunteers (age, mean ± standard deviation, 25.6 ± 0.8 years, range 25–27 years) participated in this study. The study protocol was approved by the institutional review board at the hospital of Oriental medicine, KyungHee Medical Center. Informed written consent was obtained from each subject. None of the subjects had a history of psychiatric problems, hypertension, diabetes mellitus, neurologic disorders, or head trauma. The subjects were forbidden to smoke or consume alcohol and coffee during the study.
One (1) experienced acupuncturist performed all acupuncture procedures using a stainless steel acupuncture needle with a diameter of 0.30 mm and a length of 40 mm (DongBang Acupuncture, Seoul, Korea). Each needle was inserted into the skin to a depth of approximately 5 mm at the GV20 acupoint (which is on the midsagittal line at the intersection of a line connecting the right and left ear apices 4 ) of each subject and left in position for 20 minutes (Fig. 1). During this time, stronger stimulation was generated by periodic physical rotations of the needle for a minute at 2 Hz, with 5 minutes between rotations.
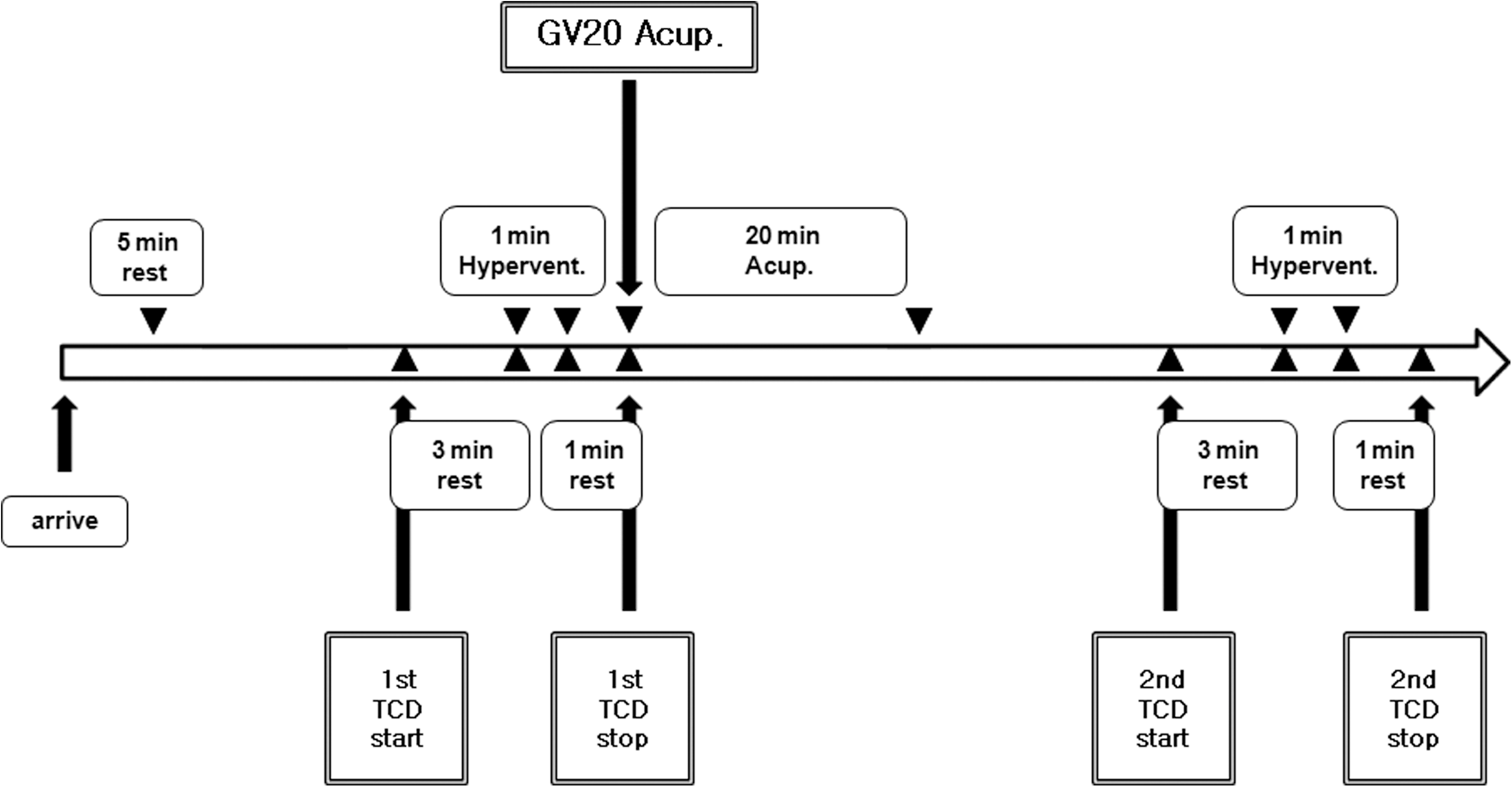
Study design on the effects of GV20 acupuncture. GV20, Bai-Hui acupoint; Acup., acupuncture; TCD, transcranial Doppler; Hypervent., hyperventilation.
Each subject took part in the study once a day at 3
Mean MCA and ACA blood velocities, and CO2 reactivity were measured by TCD using a Multi-Dop X4 system (Compumedics DWL, Singen, Germany) similar to previously described procedures 8 –10 at rest and during 1-minute hyperventilation-induced hypocapnia. Each subject was placed in the supine position with both eyes closed. The 2-MHz pulsed Doppler probe was positioned on the temporal region (ultrasonic window), and a removable bilateral probe holder (LAM-Rack; Compumedics DWL) was used to avoid shifting of the probe and permit continuous measurements. The highest signal was sought at depths ranging from 45 to 60 mm for MCA, and 65–80 mm for ACA. The sample and gain values were adjusted to the value and recorded when the waveform of CBF was well maintained. All investigations started after the subjects were stabilized for 5 minutes (Fig. 1). The mean flow velocity was calculated continuously as the time-averaged maximum velocity over the cardiac cycle computed from the envelope of the maximum frequencies. During continuous monitoring by a Cardiocap S/5 capnometer (Datex-Ohmeda, Helsinki, Finland), the subject was instructed to breathe normally until a steady state was reached. Mean MCA and ACA blood velocities at rest were obtained in the stable normocapnic condition, and the point of the temporal window was marked for the repeated study afterward. The lowest MCA and ACA mean flow velocities near the end of the hyperventilation period were examined thereafter. All TCD spectra were recorded for later review.
Since blood flow velocity is dependent on the Pa
where b is CO2 reactivity and V1 is velocity at P1CO2.
CO2 reactivity refers to the percent change in mean blood velocity per millimeter of mercury change in PETCO2, as calculated by the following formula
11
:
where Vrest is blood velocity at rest, obtained in the stable normocapnic condition, Vhypocapnia is the blood flow velocity of the latter half of the 1-minute period of hyperventilation period, and ΔPETCO2 is the change in PETCO2 from baseline to maximal hyperventilation (Fig. 1). CO2 reactivity was expressed as %/min.
The variables that may control CBF were controlled by various modules of the Cardiocap S/5 collector (Datex-Ohmeda). Blood pressure was obtained in a stable normocapnic condition before hyperventilation; this was done four times with a 2-minute interval between measurements to determine mean blood pressure. The pulse rate was continuously monitored by an oximetry apparatus positioned on the subject's finger. Also, PETCO2 was continuously monitored by a Cardiocap S/5 collector-connected nasal prong positioned on the subject's nostril, and each subject was asked to breathe only through the nose during the study. A snapshot function in the Cardiocap S/5 collector program was used to calculate the mean pulse rate and PETCO2 at certain assessment times. These three controlled variables were obtained and saved in the computer, which was connected to the Cardiocap S/5 collector program with various modules.
Using the above tools, before GV20 acupuncture treatment for each subject, the blood pressure was obtained four times with a 2-minute interval. Simultaneously, during an 8-minute interval, a continuous assessment of pulse rate was made. Subsequently, CO2 reactivity and mean blood flow velocity were obtained before and after TCD measurement. After the 20-minute GV20 acupuncture treatment, the procedure was repeated (Fig. 1).
Statistical analysis utilized Statistical Package for the Social Sciences version 12.0 for Windows (SPSS, Chicago, IL). Statistical comparisons between the values before and after GV20 acupuncture treatment were made with the Wilcoxon signed-rank test, and a p value <0.05 was considered significant. Data are expressed as mean ± standard deviation.
Results
Mean arterial blood pressure and pulse rate at rest did not change significantly after GV20 acupuncture treatment on the 10 subjects (Table 1). Corrected blood flow velocities (PETCO2 = 40 mm Hg) of right MCA, right ACA, left MCA, and left ACA during hypocapnia increased significantly after GV20 acupuncture treatment (p = 0.013 for right MCA and left MCA, p = 0.005 for right ACA and left ACA; Table 2). Also, CO2 reactivity of right MCA, right ACA, left MCA, and left ACA during hypocapnia increased significantly after GV20 acupuncture treatment (p = 0.005 for all; Table 3).
By Wilcoxon signed-rank test.
Values are mean ± standard deviation.
GV20, Bai-Hui acupoint; BP, mean blood pressure; PR, pulse rate; bpm, beats per minute.
By Wilcoxon signed-rank test.
Values are mean ± standard deviation.
CV40, corrected blood flow velocity at PETCO2 = 40 mm Hg; GV20, Bai-Hui acupoint; Rt MCA, right middle cerebral artery; Rt ACA, right anterior cerebral artery; Lt MCA, left middle cerebral artery; Lt ACA, left anterior cerebral artery.
By Wilcoxon signed-rank test.
Values are mean ± standard deviation.
GV20, Bai-Hui acupoint; CO2 reactivity, cerebrovascular reactivity to hyperventilation; Rt MCA, right middle cerebral artery; Rt ACA, right anterior cerebral artery; Lt MCA, left middle cerebral artery; Lt ACA, left anterior cerebral artery.
Discussion
The purpose of the present study was to determine whether GV20 acupuncture treatment would cause significant responses to CBF velocity and CO2 reactivity of the MCA and ACA during hypocapnia in normal subjects. Since previous related studies had some shortcomings, described later in our text, it was necessary to make some corrections to draw out a more accurate result and to make a guideline relevant for future research.
The results showed that mean corrected blood flow velocities (at PETCO2 = 40 mm Hg) of MCA and ACA, and CO2 reactivity increased significantly after GV20 acupuncture treatment. TCD was used to directly measure CBF velocity. TCD measures blood flow velocity but not CBF. However, changes in flow velocity may be proportional to those in CBF if the vessel diameter is constant. In humans, the diameter of a large cerebral artery with an internal diameter exceeding 2.5 mm does not change significantly despite alternations in Pa
Several aspects in previous studies need to be addressed. One (1) study, which used the same intervention and TCD introduced in our study, reported that mean, systolic, and diastolic velocities increased significantly, whereas pulsatility index decreased significantly at different depths of both MCAs in normal subjects. 6 However, the results of this study need to be confirmed because it lacked information about CO2 reactivity and corrected blood flow velocity (at PETCO2 = 40 mm Hg) mentioned in previous studies 5,11,28 –30 and the present studies. Furthermore, previous studies with medication intervention assumed that all territories of cerebral arteries were influenced, 5,7,31 whereas in studies with acupuncture using single-photon emission computed tomography, 32,33 only specific brain regions were affected by particular acupoints. Given the differing information, it was presently necessary to measure the mean blood flow velocities and CO2 reactivity on territories as much as possible. Hence, the present study measured not only both sides of MCA but also ACA, unlike the previous study, 6 whose conclusions were based only on measurements of the temporal region of MCAs. As a result, corrected blood flow velocities (at PETCO2 = 40 mm Hg) and CO2 reactivity of all groups increased significantly, which meant that GV20 acupuncture treatment may influence both sides of MCA and ACA territories due to GV20 acupoint's specific function and mechanism. 3
Several interesting studies have investigated significant CBF changes after acupuncture on different acupoints. An et al. 34 reported that there were specific increases in both regional CBF and glucose metabolism following electroacupuncture in both frontal regions. This common brain response in localized regions was induced from stimulation of specific acupoints (LI4 and LI11). Backer et al. 35 showed that different modes of manual acupuncture stimulation at LI4 differentially modulate CBF velocity, arterial blood pressure, and heart rate in human subjects. Also according to Litscher et al., 36 acupuncture at PC6, CV6, ST36, and SP6 significantly changed mean CBF velocity. These results are interesting in that they provide crucial evidence of acupuncture effectiveness on CBF. Compared with the present study, however, the acupuncture scheme, needle manipulation, methods of measurement, and selection of acupoints introduced in these studies were different; thus, data have to be compared with caution.
One limitation of this study was the absence of evaluation on the posterior cerebral arteries. The reason for this was due to large individual variation of the TCD incidence angle, blood flow velocity, and difficult continuous monitoring resulting from the location and structural nature of the artery. 2 Therefore, this study can only discuss the influence of the GV20 acupuncture on both sides of MCA and ACA. Further studies including an evaluation on the posterior cerebral artery will be needed to confirm the present findings. Another limitation of this study was the sample size, statistical power, and the number of related references. Not only studies with a larger sample size and attendant greater statistical power, but also more similar studies on hemodynamics of cerebral and carotid artery after acupoints stimulation as reported by Zhao et al. 37 are necessary to confirm the present findings. Also, a crucial nonacupoint control group should have been arranged, but due to an ongoing debate about the effectiveness and ethics of sham-acupuncture, we decided not to make our results controversial by adding a nonacupoint control group. Zaslawski et al. 38 reported that the experimental design of sham acupuncture may be applicable to many other acupuncture trials. However, Moffet 39 showed that most studies comparing acupuncture to sham acupuncture found no statistically significant differences in outcomes, and most of them found that sham acupuncture is efficacious, especially when superficial needling was applied at nonpoints. Moreover, as reported by Hammerschlag and Zwickey, 40 in the absence of well-documented mechanisms for most CAM therapies, with acupuncture, as representative cases, an appropriate sham control cannot be designed rationally. These findings highlight the difficulty of conducting controlled trials of acupuncture in the absence of theories about what, exactly, one is controlling for. Therefore, until the mechanisms of acupuncture are fully discovered, a sham acupuncture control group must be arranged in extreme precaution. More attention should be shifted to the question of clinical relevance, with research focused on comparing acupuncture to standard (biomedical) care, as reported by Hammerschlag 41 and Hammerschlag and Morris. 42
Conclusions
In conclusion, rheological improvement by GV20 acupuncture treatment results in increases in MCA and ACA blood flow velocities, which are associated with improvements in CO2 reactivity during hypocapnia in healthy subjects. These results may be of importance in various types of brain ischemia and stroke because rheological factors may likewise be of great importance as the determinants of CBF velocity in ischemic brain, where vasodilation is maximal and autoregulation is impaired.
Footnotes
Acknowledgments
The authors would like to sincerely thank all the professors in the department for their help throughout this study. There was no financial support throughout the present study.
Disclosure Statement
No competing financial interests exist.