
Abstract
Background:
Appendicitis is an acute condition of the abdomen that is treated with surgical intervention. Conservative treatment of appendicitis currently involves intravenous antibiotics. While conservative care is a useful tool in apprehensive patients, in conditions such as appendicitis, delays in proper treatment can be life threatening. In spite of this, some patients will still refuse surgical and pharmacologic intervention, which can significantly limit the physician's therapeutic options.
Subject:
Sonographic evidence is presented of appendicitis in a patient who strongly desired to avoid pharmacologic or surgical intervention.
Results:
The patient underwent a medically supervised water-only fast followed by a plant-based, low-fat, low-sodium diet and achieved a significant reduction and eventual elimination of symptoms.
Conclusions:
This case demonstrates the need for further research on the effects of medically supervised water-only fasting and careful refeeding in cases of uncomplicated appendicitis.
Introduction
In 1956, Coldrey 4 first reported conservative treatment of appendicitis in a series of three case studies. Two (2) patients, ages 7 and 15, were treated with antibiotics and recovered within 17 and 16 days, respectively. The third patient, aged 9, recovered within 12 days but was readmitted 4 months later for an interval appendectomy. No details were provided as to whether the patients' guardians refused surgery or requested conservative therapy. Malik and Bari 5 reported on 80 patients randomized to either surgery or intravenous antibiotics for 2 days followed by oral antibiotics for 7 days. Two (2) patients in the conservative group required surgery within 24 hours and 4 others were readmitted within 1 year due to recurrent appendicitis. Eriksson and Granstrom 6 reported a prospective controlled study of 40 patients that concluded conservative management of appendicitis with antibiotics only was as effective as surgery in reducing pain and need for analgesia. The rate of eventual surgical intervention (8 of 40) was high, however.
So far, antibiotics have been the only nonsurgical treatment of uncomplicated appendicitis reported in the literature. The potential disadvantages of antibiotic treatment, besides potential allergic reaction to the drugs, are the higher risk of recurrence and increased risk of patient susceptibility to strains of antibiotic-resistant bacteria.
Medically supervised, water-only fasting may present another possibility due to its anti-inflammatory and immune-enhancing effects, especially for patients who request conservative therapy. Lithell 7 studied patients with chronic inflammatory conditions and found fasting to have potent anti-inflammatory effects. Wing et al. 8 found that macrophage activity was enhanced during fasting. In another study, Wing et al. 9 found that blood monocyte bactericidal activity and natural killer cell cytolytic activity in humans were improved by fasting. Palmblad et al. 10 found that fasting significantly reduced serum levels of acute phase reactants C3, haptoglobin, and orosomucoid.
Case Report
A 46-year-old man with right lower quadrant pain presented to an integrated medical facility that included medically supervised water-only fasting among its treatment options. The patient reported full, peri-umbilical abdominal pain that had moved to the bladder area within the past 3 days, was worse with urination, improved with pillow pressure, and was unrelated to meals. The patient denied dysuria, hematuria, nausea, vomiting, constipation, diarrhea, or fever. Upon physical examination, he was noted to be afebrile and there was a tender, nonprotruding 1-cm mass in the right lower quadrant.
An inguinal hernia was suspected, so a surgical consultation was obtained. However, it was concluded that there was no hernia, that the pain might be musculoskeletal, and that it appeared to be improving. The patient was advised by the surgeon to use nonsteroidal anti-inflammatory medication and to return if it worsened or if a bulge developed.
The patient returned to the integrated medical facility approximately 1 month later and reported that the pain had worsened. It prevented him from exercising and it was aggravated by walking, moving, driving over bumpy roads, urinating, and turning in bed. The patient again denied dysuria, hematuria, nausea, vomiting, constipation, diarrhea, and fever. A physical examination revealed mild right lower quadrant tenderness without mass or rebound tenderness. Laboratory tests revealed a normal white blood cell count of 5800/μL, normal differential, and slightly elevated erythrocyte sedimentation rate of 18 mm/h.
A retroperitoneal sonogram revealed an enlarged appendix accompanied by noncompressibility and increased blood flow along the periphery, findings that were suggestive of appendicitis (Fig. 1). The patient was advised of standard treatment of removal but wanted to try medically supervised water-only fasting to avoid surgery.
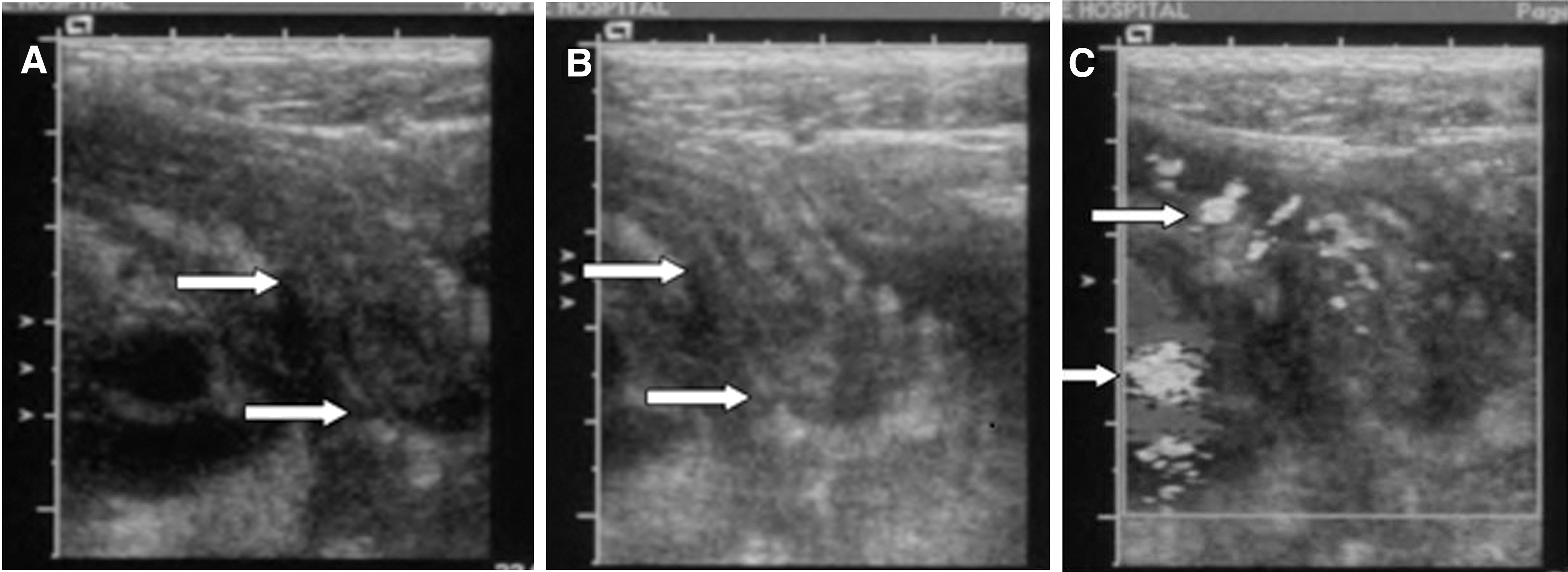
The enlarged appendix can be visualized on images
The patient agreed to surgery only if a brief trial of medically supervised water-only fasting yielded no improvement. Consequently, he was interviewed and examined on physical, mental, and emotional levels, and was found to be a safe candidate for fasting. He was prepared and underwent a fast for 7 days following the specific protocol for fasting previously outlined by the International Association of Hygienic Physicians 11 and subsequently adapted by Goldhamer et al. 12
The patient was monitored daily by on-site physicians in a residential facility. Twice-daily interviews and examinations were performed throughout the fast. Vital signs were taken once in the morning for the duration of the patient's stay as well as a urinalysis performed every 5 days. The 7-day fast was followed by a 4-day gradual reintroduction of food consisting of juice, fruits, and raw and steamed vegetables. After the careful refeeding period, the abdominal pain was much improved. A physical examination revealed a nontender abdomen, although subjectively the patient reported mild sensitivity to the palpation. Follow-up laboratory tests revealed a normal white blood cell count. He remained afebrile.
The patient was advised of healthy diet and lifestyle choices such as a plant-based diet low in sodium and fat along with adequate sleep. He continued with regular follow-ups over the next 3 months. At 3-month follow-up, the patient reported compliance to recommendations and no further abdominal pain. The patient reported that he had been able to resume his normal exercise regimen of running 4 hours per week. Physical examination revealed subjective mild sensitivity to palpation in the right lower quadrant.
At 1-year follow-up, the patient reported no return of the abdominal pain over the year. He had resumed full exercise and had even completed a triathlon. Physical examination revealed a nontender abdomen.
At 2-year follow-up, the patient reported compliance to the lifestyle recommendations, continued to be free of right lower quadrant pain, and still had no recurrence of symptoms since the original presentation.
Discussion
Fasting was first reported in the medical literature in 1880. 13 Since then, the physiology, 14 pathophysiology, 15 and metabolic effects 16 have been examined. Articles have appeared in medical journals on the use of therapeutic fasting for inflammatory conditions such as acute glomerulonephritis, 17 acute pancreatitis, 18 rheumatoid arthritis, 8,19 –21 systemic lupus erythematosus, 21 and irritable bowel syndrome. 22 To date, however, medically supervised water-only fasting has not been reported for appendicitis. The anti-inflammatory and immune-enhancing effects of fasting may have been responsible for this particular outcome, although the exact mechanisms remain unclear.
In this particular case, several factors may have contributed to the apparent success of this intervention. First, the patient appeared to have subacute appendicitis in that he was afebrile, had a normal white blood cell count, no rebound tenderness or rigidity, and only sonographic evidence of an inflamed appendix. This allowed for the entertainment of a “wait-and-see” approach. Second, the patient strongly desired to avoid surgery and try nonpharmacologic conservative therapy, and thus was very motivated to comply with the strict protocols of medically supervised water-only fasting. Third, the entire conservative therapy was medically supervised. Vital signs, urinalysis, symptoms, blood chemistries, and water intake were all monitored during the patient's stay with the understanding that any progression of symptoms would warrant emergency care, including surgical evaluation.
Conclusions
This case demonstrates the need for further research on the effects of medically supervised water-only fasting and careful refeeding in cases of uncomplicated appendicitis. In our case, the patient refused invasive medical treatment but ultimately benefited from medically supervised conservative treatment. If future research can demonstrate that this case study was not anomalous, can identify optimal candidates for this treatment regimen, and can delineate algorithms for surgical intervention, those patients who choose to refuse surgery and antibiotics may be able to expand their treatment options for a traditionally surgical diagnosis.
Footnotes
Disclosure Statement
No competing financial interests exist.