
Abstract
Objectives:
The study objectives were to evaluate the efficacy of integrating hatha yoga therapy with therapeutic exercises for osteoarthritis (OA) of the knee joints.
Design:
This was a prospective, randomized, active controlled trial. Two hundred and fifty (250) participants who had OA knees and who were between 35 and 80 years (yoga 59.56±9.54) and (control 59.42±10.66) from the outpatient department of Ebnezar Orthopedic Center, Bengaluru, were randomly assigned to receive hatha yoga therapy or therapeutic exercises after transcutaneous electrical stimulation and ultrasound treatment (20 minutes per day). Both of the groups practiced supervised interventions (40 minutes per day) for 3 months. One hundred and eighteen (118) (yoga) and 117 (control) subjects were available for the final analysis.
Results:
There were significant differences within (Wilcoxon's, p<0.001) and between the groups (Mann–Whitney U, p<0.001) on all the variables, with better improvements in the yoga than the control groups. Walking pain in the yoga (37.3%, 64.9%) and control (24.9%, 42%), knee disability in the yoga (59.7%, 83%) and control (32.7%, 53.6%), range of knee flexion in yoga (12.7%, 26.5% right, 13.5%, 28% left) and control (6.9%, 13.3% right, 5.6%, 11.5% left), joint tenderness in yoga (52.3%, 86.1%) and control (28%, 57.1%), swelling in yoga (55.4%, 85.9%) and control (32.1%, 60%), crepitus in yoga (44.0%, 79.9%) and control (27.0%, 47.8%) and walking time in yoga (26.6%, 52.8%) and control (9.3%, 21.6%), all improved more in the yoga than the control groups on the 15th and 90th day, respectively.
Conclusions:
An integrated approach of hatha yoga therapy is better than therapeutic exercises as an adjunct to transcutaneous electrical stimulation and ultrasound treatment in improving walking pain, range of knee flexion, walking time, tenderness, swelling, crepitus, and knee disability in patients with OA knees.
Introduction
The need for safer treatment of OA has led to research into many alternative and complementary therapies. 9 There are several randomized placebo-controlled trials (RCTs) that have used nonpharmacological interventions for OA knees. In a meta-analysis of 36 RCTs on 1391 patients, manual acupuncture, static magnets, and ultrasound therapies did not offer statistically significant short-term pain relief over placebo, while pulsed electromagnetic fields offered a small reduction in pain. Transcutaneous electrical nerve stimulation (including interferential currents), electro-acupuncture and low-level laser therapy offered clinically relevant pain relieving effects that seemed to persist for at least 4 weeks. This review by Bjordal et al. concluded that physiotherapy modalities at the most offer only short-term relief of pain and hence add-on therapies such as exercises, acupuncture, and so on may be beneficial. 10
The beneficial effects of yoga on OA hands have been reviewed by Garfinkel. 11 This author studied the effects of 10 weeks of supervised yoga in an RCT on 25 subjects and showed significant reduction in pain, tenderness, and improved range of motion of fingers. 12 In another pilot study on 11 patients with OA knees, Kolasinski et al. showed reduction in pain and disability. 13
Ranjita and Nagarathna (unpublished observations) showed 28%–45% improvement in pain and mobility after 1 week of intensive residential integrated yoga therapy for OA knees.
There are studies on add-on exercise to physiotherapy, 14 and acupuncture to physiotherapy as adjuvant therapies, 15 but there are no studies on add-on yoga to physiotherapy. Also, there are no RCTs that have looked at the effect of yoga on OA knees with active intervention for the control group. Hence, the present study was planned to study the effects of yoga as an adjunct to physiotherapy in the treatment of OA knees.
Materials and Methods
Two hundred and fifty (250) patients with OA knees from the outpatient department of Ebnezar Orthopedic Center, Bengaluru were recruited for the study. Table 1 shows the baseline characteristics that were similar between groups on all variables (p>0.05, Mann–Whitney test for prevalues). A sample size of 250 was obtained on G power software by fixing the α at 0.05 powered at 0.8 and an effect size of 0.379, considering the mean and SD of an earlier study. 16
SD, standard deviation.
Two hundred and fifty (250) patients of both genders in the age group of 35–80 years (59.56±8.18) in the yoga group and (59.42±10.66) in the control group with OA knees (one or both joints) satisfying the American College of Rheumatism (ACR) guidelines 17 for diagnosis were included. The inclusion criterions were (1) persistent pain for 3 months prior to recruitment; (2) moderate to severe pain on walking; (3) Kellgren and Lawrence 18 radiologic grading of II–IV in x-ray films taken within 6 months prior to entry; and (4) those fully ambulant, literate, and willing to participate in the study. Those with (1) grade I changes in the x-ray films; (2) acute knee pain; (3) secondary OA due to rheumatoid arthritis, gout, septic arthritis, tuberculosis, tumor, trauma, or hemophilia; and (4) those with major medical or psychiatric disorders were excluded.
The study was approved by the Institutional Review Board and ethical committee of SVAYSA University. Signed informed consent was obtained from all the participants.
Design
This was a prospective, randomized, parallel active controlled study on patients with OA knees in the age range of 35–80 years. Patients attending the outpatient department of Ebnezar Orthopedic Center who satisfied the inclusion criteria were recruited for the study. After the initial screening for selection criteria, they were assigned to either the yoga or the control group. A computer-generated random-number table (
Both of the groups had supervised practices at the center (40 minutes per day) after physiotherapy (20 minutes per day) for 2 weeks. The yoga classes were conducted in the basement of the center where one hall was exclusively dedicated for yoga therapy. The study group was taught integrated yoga and the control group the nonyogic therapeutic exercises by certified therapists Dr. Yogitha Bali, Mrs. Pragati, and Mr. Rangaji—all trained at Yoga University, SVYASA, Bangalore. After this they were asked to practice daily at home for the next 12 weeks. The patients were asked to mark the practices daily in the diary provided for this purpose after their home practice. Compliance was supervised by telephone calls once in 3 days, and a weekly review was conducted once a week for 12 weeks. The daily review cards were checked for the regularity and doubts, if any, were clarified. This along with their clinical progress was checked and documented at every visit. All the assessments were carried out on the first, 15th, and 90th day by the therapists.
Blinding and masking
As this was an interventional study, double blinding was not possible. The answer sheets of the questionnaires were coded and analyzed after the study was completed. The statistician who did the randomization and data analysis, and the researcher who carried out the assessments were blinded to the treatment status of the subjects.
Intervention for yoga group
The daily routine practiced at the center in the yoga group included 40 minutes of integrated yoga therapy practice after 20 minutes of physiotherapy with transcutaneous electrical stimulation and ultrasound for 2 weeks. The integrated yoga therapy practice included shithilikarana vyayamas (loosening practices), sakti vikasaka (strengthening practices), followed by yogasanas and relaxation techniques with devotional songs. Later patients were advised to continue the integrated yoga therapy practice for 40 minutes at home for the next 10 weeks (Table 2).
TENS, transcutaneous electrical nerve stimulation.
The concepts used to develop a specific module of an integrated approach of yoga therapy for knee pain were taken from the traditional yoga scriptures (patanjali yoga sutras, yoga vasishtha, and upanishads) that highlight a holistic lifestyle for positive health at physical, mental, emotional, and intellectual levels.
19
Yoga is defined as the mastery over the modifications of mind (chitta vritti nirodhah: definition of yoga by patanjali). It helps to remove the unnecessary surges of neuromuscular activation resulting from heightened stress responses that may contribute to aging.
20
The daily routine included a 40 minutes practice as follows: • Yogic sukshma vyayamas (loosening and strengthening practices): These are safe, rhythmic, repetitive stretching movements synchronized with breathing. These practices mobilize the joints and strengthen the peri-articular muscles. • Relaxation techniques: Three (3) types of guided relaxation techniques were interspersed between the physical practices of sukshmavyayamas and asanas. • Asanas (physical postures): Asanas are characterized by effortless maintenance in the final posture by internal awareness. Asanas were selected in standing, supine, and prone positions that would relax and strengthen the knee joints. • Pranayama: The practice of voluntary regulated breathing while the mind is directed to the flow of breath is called pranayama. These practices promote autonomic balance through mastery over the mind.
21
• Meditation: Patanjali defines meditation (dhyana) as effortless flow of a single thought in the mind without distractions (pratyaya ekataanata dhyanam). This has been shown to offer physiologic benefits through alertful rest to the mind–body complex.
22
• Lectures and counseling: Yogic concepts of health and disease, yama, niyama, bhakti yoga, jnana yoga, and karma yoga were presented in the theory classes. These sessions were aimed at understanding the need for lifestyle change, weight management, and preventing early aging by yogic self-management of psychosocial stresses.
Intervention for control group
The daily routine practiced at the center in the control group included 40 minutes of therapeutic exercises after 20 minutes of physiotherapy with transcutaneous electrical stimulation and ultrasound for 2 weeks. These therapeutic exercises included loosening and strengthening practices for all the joints of the upper and lower limbs, a brief period of rest, specific knee practices, and supine rest followed by light music. Later the patient was advised to continue the therapeutic exercise practice of 40 minutes at home for the next 12 weeks (Table 3).
Outcome variables
Pain while walking
Patients were asked to mark the severity of their pain experienced while walking in the past few days on the walking numerical rating scale (WNRS). For this purpose, a 10-cm line drawn in the center of a white sheet with “0” as “no pain” and “10” as “worst possible pain” was used. 23 Separate sheets were used during each assessment.
Knee disability score
This was assessed by WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index Score for Knee Joint) that consists of 24 questions under three domains as follows: Pain (5 questions), Physical functions (17 questions), and Stiffness (2 questions). Each item was scored by the patient on a 5-point scale (0–4). Total WOMAC score is the sum of the scores on all items. The higher the score, the more severe the disability is. This multidimensional questionnaire has well-defined reliability, test–retest reliability, content and construct validity, at Cronbach's α of 0.88–0.95 and concordance correlation coefficient of 0.85–0.94. 24
Active range of movements
The degree of knee flexion was measured by using a dial-type goniometer (Anand Agencies, Pune, India). This instrument has a dial with calibration from 0 to 360°. The patient rested in the supine position on the couch. The center of the goniometer was placed on the outer side of the knee joint with the two arms firmly held along the thigh and leg. The range of flexion was noted on the dial as the knee was bent slowly to its maximum.
Tenderness
Knee tenderness was graded by the clinician using the following key: Grade 1–tenderness on deep palpation, Grade 2–patient winces on pressure, Grade 3–patient winces and withdraws, and Grade 4–patient does not allow the examiner to touch. 25
Swelling of the knee
Swelling was graded on a 4 (0–3)-point scale by the clinician.
Crepitus
This was also assessed by the clinician on a 5-point severity scale (0–4).
Walking time
The time taken to walk 50 m was recorded using a stopwatch.
Statistical methods
The data were analyzed using SPSS Version 16. The baseline values of the two groups were checked for normal distribution by the Shapiro Wilk test. Baseline matching was checked by the Mann–Whitney test. Wilcoxon signed-rank test and Mann–Whitney U test were used for assessing “within” and “between” group differences, respectively.
Results
The study profile is shown in Figure 1. There were 7 dropouts in the study group and 8 in the control group. Table 4 shows the results within the yoga group on the 15th and 90th day. Table 5 shows the results within the control group on the 15th and 90th day. Table 6 shows the results between the yoga and control groups.
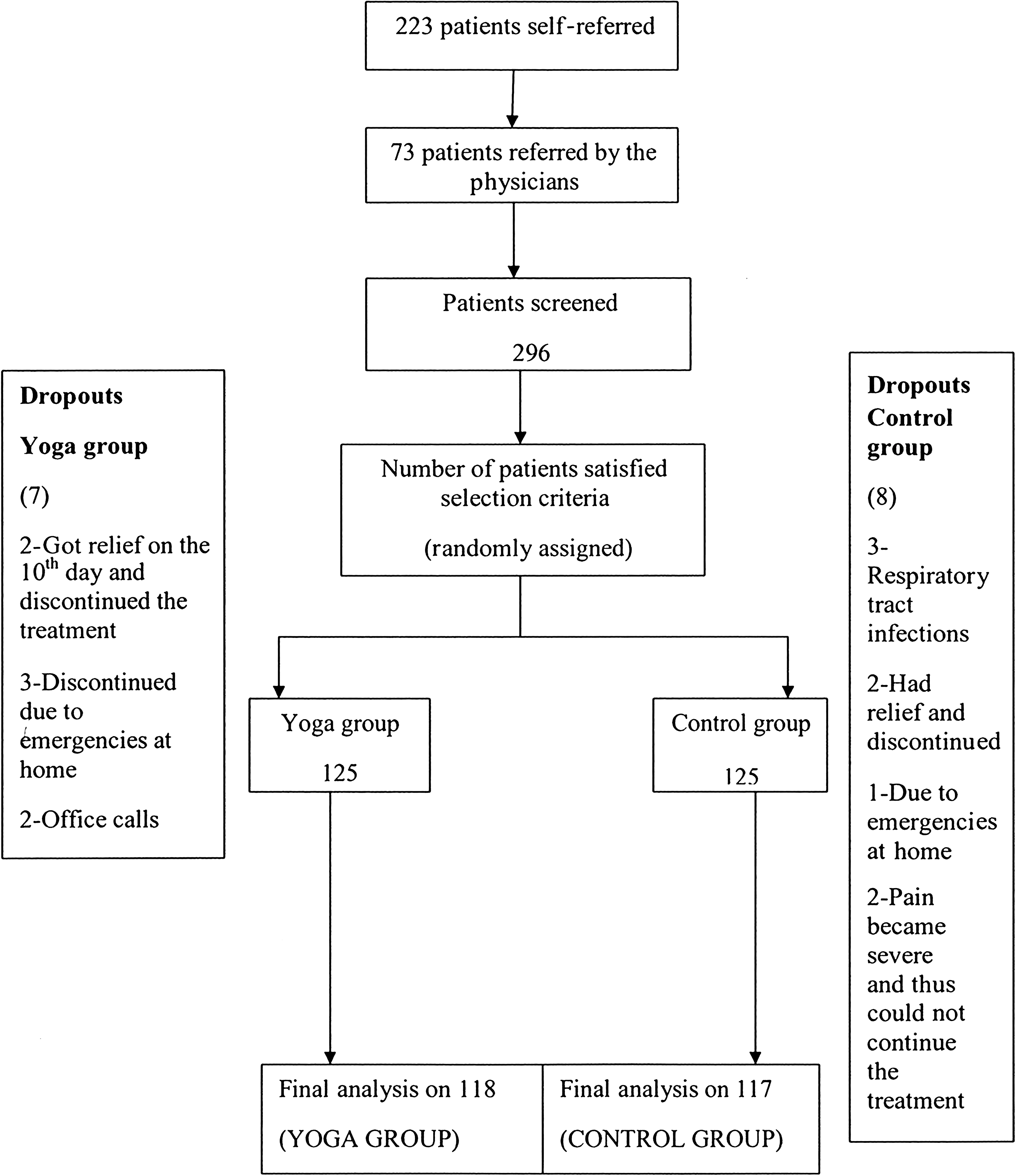
Study profile.
VB, variables; SD, standard deviation; CI, confidence interval; ES, effect size; % change; percentage change.WP, walking pain; KDS, knee disability score; RNF, right knee flexion; LNF, left knee flexion; TN, tenderness; SW, swelling; CR, crepitus; WT, walking time; Po 1, post (15th day); Po 2, post (90th day); LB, lower bound; UB, upper bound.
VB, variables; SD, standard deviation; CI, confidence interval; ES, effect size; % change, percentage change; LB, lower bound; UB, upper bound; WP, walking pain; KDS, knee disability score; RNF, right knee flexion; LNF, left knee flexion; TN, tenderness; SW, swelling; CR, crepitus; WT, walking time; Po 1, post (15th day); Po 2, post (90th day).
ES, effect size; WP, walking pain; KDS, knee disability score; RNF, right knee flexion; LNF, left knee flexion; TN, tenderness; SW, swelling; CR, crepitus; WT, walking time; Po 1, post (15th day); Po 2, post (90th day).
Walking pain
The baselines were matched for both groups and data were not normally distributed. There was a significant difference in walking pain (WNRS) within (Wilcoxon, p<0.001) and between the groups (Mann–Whitney U test, p<0.001) after the intervention with higher effect size in the yoga than in the control group.
Knee disability score (WOMAC)
There was a significant difference in knee disability within (Wilcoxon, p<0.001) and between the groups (Mann–Whitney U test, p<0.001) after the intervention with higher effect size in the yoga than in the control group.
Goniometry for knee movements
There was a significant difference within (Wilcoxon, p<0.001) and between the groups (Mann–Whitney U test, p<0.001) in the flexion of right and left knee joints after the intervention with higher effect size in the yoga than in the control group.
Tenderness, swelling, and crepitus also showed a significant difference within (Wilcoxon, p<0.001) and between the groups (Mann–Whitney U test, p<0.001) after the intervention with higher effect size in the yoga than in the control group.
Walking time
There was a significant difference in walking time within (Wilcoxon, p<0.001) and between the groups (Mann–Whitney U test, p<0.001) after the intervention with higher effect size in the yoga than in the control group.
Discussion
This randomized two-armed parallel controlled trial on 250 participants included patients of both genders in the age group of 35–80 years with OA of the knee joints. Results showed significantly better improvement in the yoga than in the control group on all variables (p<0.001, Mann–Whitney) (i.e., walking pain, knee flexion, walking time, tenderness, swelling, crepitus, and knee disability.
Pain reduction
The reduction in walking pain observed in this study points to the beneficial effect of yoga as an add-on therapy to conventional physiotherapy practices.
In a pilot study on OA knees, Kolasinski et al. 13 used a specific sequence of asanas based on the teachings of Iyengar for 8 weeks. They measured the pain by WOMAC with a significant reduction (p< 0.04) in pain by 46.7%. In another pilot study on yoga for OA knees, Ranjita and Nagarathna (unpublished observations) used a set of integrated yoga therapy program similar to the current study in a nonresidential camp set up for 1 week without any physiotherapy intervention. They showed a 40% reduction (from 6.59±2.24 to 3.97±2.44) in resting pain after yoga. In the current study, yoga was added after the standard physiotherapy, which showed a reduction in walking pain scores by 37.3% and 65% after 15 and 90 days, respectively.
The baseline pain scores were much higher in the current study (9.54±0.61) than in Ranjita's study (6.59±2.24). This difference is because Ranjita recorded the resting pain and the current study documented the pain while walking. However, the degree of changes appears to be similar in all the three yoga studies (37%–47%). This may point to the efficacy of yoga when used with or without a session of physiotherapy before the practice of yoga.
Similar effects of pain reduction have been observed by Garfinkel et al. 26 in an RCT on yoga for carpal tunnel syndrome, wherein the mean numerical rating scale (NRS) scores for pain decreased significantly (p=0.02) from 5.0 to 2.9 mm. Tekur et al. 27 studied the efficacy of an integrated approach of yoga therapy (IAYT) in patients with chronic low back pain which included several cases of spondylosis of the spine and documented 48.8 % reduction in NRS scores in the yoga group within 1 week of A residential program without offering any physiotherapy intervention. Garfinkel et al. 12 looked at the effect of Iyengar yoga in OA hands. Pre–post difference in mean scores of “pain during activity” in their study was similar (4.29) to the current study (3.56 at the second week and 6.19 at 3 months). However, they did not observe a significant difference between groups in tenderness, swelling, or hand functions, whereas these variables were significantly better in yoga than controls in the current study.
Knee disability score
In Kolasinski's study on OA knees 13 there was a reduction in WOMAC knee disability score by 44% (p<0.04). In the present study, the disability reduced by 60% to 83% on the 15th and 90th day in the yoga group. In the Ranjita and Nagarathna (unpublished observations) study of 1 week of intensive yoga without physiotherapy, there was improvement in performance-oriented mobility (45%) and also in the “Timed up and Go” test (28% in “number of steps” and 30% in “time taken”). Haslock et al., 28 in their controlled study on IAYT for patients who had a severe degree of rheumatoid arthritis and who had secondary OA, also showed a significant reduction in pain and functional disability, with 63% (left) and 66% (right) increase in hand grip strength in the yoga group as compared to an increase of 5% and 8% in their control group.
Walking time
The study by Kolasinski et al. 13 on Iyengar yoga for OA knees did not show any improvement in the walking time, whereas the current study observed significant reduction in walking time by 27% after 15 days and 53% after 90 days of IAYT. Fisher et al. 29 measured the effects of a quantitative progressive exercise muscle rehabilitation program that was added to a physical therapy program and observed significant decreases in walking time and pain experienced during activities.
Mechanisms
Activation of pain fibers (unmyelinated and small myelinated) found in the joint capsules, ligaments, synovium, bone, and the outer edges of the menisci, increased intramedullary tension, subchondral microfractures, osteophyte formation, and flexion contractures due to OA changes are the major factors that cause pain. 30 Decreased muscular stamina and muscle spasm are additional factors that can aggravate pain and disability. The actual experience of pain is a psychologic phenomenon that has several additional central processes that include affective, behavioral, and cognitive factors. 31 The multifactorial approach of yoga comprises practices that involve not only physical practices (asanas) that may provide benefits locally at the joint level but also includes breathing (pranayama), meditation (dharana and dhyana), introspective intellectual (jnana yoga) and emotion management (bhakti yoga) practices that promote healthy behavioral and lifestyle changes.
Muscle strengthening is the key component of exercises for OA since muscle weakness is one of the major causes of pain and disability. Studies have demonstrated the efficacy of exercise programs in improving muscle strength, flexibility, mobility, and coordination in patients with OA of knee and hip joints. 32 –34 There are several studies that have demonstrated better muscular stamina and strength 35 as well as steadiness and flexibility 36 after yoga in normal volunteers. This has been observed in patients with rheumatoid arthritis also. 28 The correct way of positioning the body in space at rest and during motion achieved through introspective body awareness differentiates yoga from physical exercises. The stress-reducing effect of yoga seems to be the other major mechanism of its efficacy in pain management in these patients. 37
Strengths of the study
Good sample size, randomized controlled design, active supervised intervention for the control group for the same duration as the experimental group, and follow-up for 3 months with good compliance (6% dropouts) are the strengths of this study. The results of this study have shown marked differences on all the variables between the groups and thus offer strong evidence for incorporating this yoga module for the management of OA knees by clinicians.
Limitations of the study
The study was on a select group who presented to a specialty orthopedic center and hence is not generalizable.
Suggestions for future work
A longer follow-up of ≥12 months is necessary to check for long-term efficacy and long-term acceptability. Studies using magnetic resonance imaging and biochemical variables may throw a better light on the mechanisms.
Conclusions
An adjunctive program with an integrated approach of hatha yoga therapy for OA knees reduces walking pain, tenderness, swelling, crepitus, disability, and walking time, and increases the range of flexion better than the therapeutic exercises. It thus offers a good value addition as a nonpharmacological intervention in the management of OA knees.
Footnotes
Acknowledgments
We are thankful to Dr. Ravi Kulkarni, statistician; Dr. Yogitha, Mrs. Pragati, and Mr. Rangaji, yoga therapists; and Mr. Zafar and Mr. Vishwanath, physiotherapists, who helped us in conducting this study. We gratefully acknowledge the help of all the staff members of SVYASA and Ebnezar orthopedic center for their cooperation in conducting and funding this study.
Disclosure Statement
No competing financial interests exist.