
Abstract
Objectives:
The aim of this study was to use magnetic resonance imaging (MRI) together with proton magnetic resonance spectroscopy (1H-MRS) to study the influence of acupuncture therapy on abdominal fat and hepatic fat content in obese children.
Design:
The design was a longitudinal, clinical intervention study of acupuncture therapy.
Subjects:
Subjects were 10 healthy, obese children (age: 11.4 ± 1.65 years, body–mass index [BMI]: 29.03 ± 4.81 kg/m2).
Measurements:
Measurements included various anthropometric parameters, abdominal fat (assessed by MRI) and hepatic fat content (assessed by 1H-MRS) at baseline and after 1 month of acupuncture therapy.
Results:
One (1) month of acupuncture therapy significantly reduced the subjects' BMI by 3.5% (p = 0.005), abdominal visceral adipose tissue (VAT) volume by 16.04% (p < 0.0001), abdominal total adipose tissue volume by 10.45% (p = 0.001), and abdominal visceral to subcutaneous fat ratio by 10.59% (p = 0.007). Decreases in body weight (-2.13%), waist circumference (-1.44%), hip circumference (-0.33%), waist-to-hip ratio (WHR) (-0.99%), abdominal subcutaneous adipose tissue (SAT) volume (-5.63%), and intrahepatic triglyceride (IHTG) content (-9.03%) were also observed, although these were not significant (p > 0.05). There was a significant correlation between the level of abdominal fat (SAT, VAT) and anthropometric parameters (weight, BMI, waist circumferences, hip circumferences). There was no statistically significant correlation between IHTG and anthropometric parameters or abdominal fat content.
Conclusions:
The first direct experimental evidence is provided demonstrating that acupuncture therapy significantly reduces BMI and abdominal adipose tissue by reducing abdominal VAT content without significant changes in body weight, waist circumference, hip circumference, WHR, abdominal SAT, or IHTG content. Thus, the use of acupuncture therapy to selectively target a reduction in abdominal VAT content should become more important and more popular in the future.
Introduction
The prevalence of overweight children, defined by a body–mass index (BMI) greater than the 95th percentile for age and sex on the Centers for Disease Control growth charts, has tripled in the United States in the past 3 decades. 3 –5 Results of the most recent National Health and Nutrition Examination Survey estimate that 20.6% of children 2–5 years of age, 30.3% of children 6–11 years of age, and 30.4% of adolescents and young adults 12–19 years of age are overweight or are at risk of becoming overweight. 5 There also is growing evidence that obese children are at greater risk for several metabolic disturbances, including glucose intolerance, insulin resistance, hyperlipidemia, the metabolic syndrome, and diabetes mellitus, as well as for cardiovascular disease and nonalcoholic fatty liver disease. 6 –10
Therefore, the prevention and treatment of obesity have become major problems facing medical professionals. At present, there are numerous therapies for obesity, including pharmacotherapy, acupuncture therapy, dietary therapy, exercise therapy, and surgical therapy. Acupuncture is based on the theory that health is determined by a balanced flow of energy (qi), which is thought to be present in all living organisms. This life energy circulates throughout the body along a series of energy pathways (meridians). Each of these meridians is linked to specific internal organs and organ systems. Within this system of energy pathways, there are over 1000 acupoints that can be stimulated through the insertion of needles. This is thought to help correct and rebalance the flow of life energy, and restore health. Acupuncture has been practiced for over 5000 years and is known to have a positive effect on reducing obesity. 11,12 Acupuncture therapy, with its unique advantages of safety, efficacy, simplicity, inexpensiveness, and nontoxic side-effects, is becoming increasingly popular among patients.
However, the effects of acupuncture therapy on obese individuals have not been precisely defined. In China and Asia, the results of many studies investigating the use of acupuncture for weight control provide preliminary evidence of the potential effect of acupuncture on weight loss. 13 –17 Recent studies have indicated that acupuncture can reduce body weight in patients with simple obesity, as well as lower their BMI and waist-to-hip ratio (WHR). 18,19
Evidence is emerging that the metabolic risks associated with obesity are closely correlated with a central (abdominal), rather than a peripheral (gluteofemoral), fat pattern. 20 Abdominal visceral adipose tissue (VAT) is an important risk factor for obesity-related metabolic disorders. 9,10,20 –22 Thus, it is clinically important to be able to accurately measure abdominal fat tissue. Measurements of body circumferences, such as WHR, or calculation of BMI, although convenient and inexpensive, do not allow direct quantification of visceral fat. 23,24 Imaging techniques are certainly the most precise and reliable methods for a qualitative and quantitative subcutaneous adipose tissue (SAT) and VAT analysis. X-ray computerized tomography (CT) more accurately estimates the amount of visceral fat, but exposes subjects to ionizing radiation. 25 In addition, due to the radiation exposure required for the CT examination, the number of measurements that can be performed on one individual is limited, making this diagnostic method unsuitable for studies requiring repeated measurements on the same subject. 26 Magnetic resonance imaging (MRI) represents one of the safer and more accurate noninvasive techniques. It does not require water submersion or radiation exposure, provides images that are useful for clinical diagnosis, and has been used to characterize adipose tissue volumes. 27,28
Excessive storage of intrahepatic triglycerides (IHTG) is a common feature of obesity 29 and independently increases the risks of insulin resistance, 30 metabolic syndrome, 31 and cardiovascular disease. 32 Hepatic steatosis not attributable to excessive alcohol intake, or nonalcoholic fatty liver disease, may affect 30% of the adult population 33,34 and the majority of obese individuals. 29 Although liver biopsy is considered the “gold standard” for measuring IHTG, CT scanning and localized proton magnetic resonance spectroscopy ( 1 H-MRS) offer noninvasive alternatives. 1 H-MRS appears to provide a more sensitive measure of hepatic fat content than X-ray CT, 21,35,36 facilitating accurate measurements even in nonobese subjects with very low liver fat content. Values given by 1 H-MRS correlate with liver biopsy results 37,38 ; it is thus widely considered to be the optimal noninvasive method to assess IHTG and diagnose hepatic steatosis. 39
To date, no study has looked at the effects of acupuncture therapy on abdominal fat and hepatic fat content in obese children. Therefore, the goals of this study were to simultaneously measure total abdominal adipose tissue volume, VAT volume, SAT volume, and IHTG content in obese children, using noninvasive 1 H-MRS and MRI to assess the effects of acupuncture therapy on hepatic and abdominal lipids in 10 obese children.
Subjects and Methods
Subjects
Ten (10) 9–14-year-old obese children (7 boys and 3 girls with a mean age of 11.4 ± 1.65 years and a mean BMI of 29.03 ± 4.81 kg/m2) were recruited from Beijing Children's Hospital from July to September 2009. All patients gave informed consent, and the ethical committee approved this study. All obese participants had BMI > 95th percentile for age according to Centers for Disease Control and Prevention growth charts. 40 The subjects had not undergone any other weight-control measures within the 3 months prior to this study. The exclusion criteria included endocrinopathies, congenital metabolic diseases, genetic diseases, liver and kidney disease, or a history of using drugs that affect lipid metabolism.
Methods
Clinical measurements
Anthropometric parameters, including weight, height, BMI (weight in kilograms divided by height in meters squared), waist circumference, hip circumference, and WHR were measured and calculated. Anthropometric measurements were obtained on the same day MRI was performed.
Acupuncture therapy
In view of the clinical practice and according to its etiology and pathogenesis, obesity can be classified into the following type: “heat” in the stomach and intestine, a deficiency of qi in the spleen and stomach, and a deficiency of primary qi. 14 In this study, the patients were classified into two types by differentiation of clinical syndromes: coated tongue and pulse tracings. The acupoints were selected accordingly.
The type of excessive “heat” in the stomach (7 cases): The typical symptoms and signs were obesity, hyperorexia, polyorexia, dry mouth with a desire for drink, aversion to heat with lots of sweat, irritability, constipation, deep-yellow and scanty urine, red tongue with yellow and sticky coating, and rapid, taut, and slippery pulse.
Acupoints: Tianshu (ST25), Liangqiu (ST34), Zusanli (ST36), Gongsun (SP4), Quchi (LI11), Hegun (LI4), Zhigou (SJ6), Shangjuxu (ST37), and Neiting (ST44).
The type of excessive dampness due to spleen deficiency (3 cases): The typical symptoms and signs were obesity, lusterless complexion and lips, anorexia, abdominal distension after meals, lassitude, palpitation, shortness of breath, lethargy, loose stools, normal or scanty urine with edema, pale tongue with greasy coating, and deep and thready pulse. Acupoints: Tianshu (ST25), Liangqiu (ST34), Zusanli (ST36), Gongsun (SP4), Zhongwan (RN12), Yinlingquan (SP9), Fenglong (ST40), Qihai (RN6), and Shuifen (RN9).
Manipulation: The NK3010 needles (Jianweishi brand, Shanghai, China) were inserted through the skin to the acupoints. The needles were lifted, thrust, and twirled by using a mild reinforcing–reducing method. Needles remained in place for 15 minutes, and the treatment was given twice weekly over the course of 1 month. Simultaneously the acupoints were connected to the KWD-808II acupuncture stimulator (Yingdi brand, Changzhou, China). Intermittent wave was adopted.
Magnetic resonance data acquisition
All MRI and 1 H-MRS measurements were performed using a Philips Achileva 3.0-T MR scanner (Philips Healthcare, Best, the Netherlands) after a 10-hour overnight fast.
MRI for abdominal fat
T1-weighted transverse images were acquired using a turbo field echo sequence (repetition time [TR]/echo time [TE] = 10/2.3 ms, slice thickness = 5 mm, gap = 0 mm, flip angle = 15 degrees) with the patients supine. A total of 15 slices of T1-weighted transverse images (centered at the left renal hilum) were obtained from each subject with a sense torso coil or a cardiac coil. To minimize artifacts due to breathing, a respiratory triggering mode was employed. SAT and VAT content in the abdominal region was quantified from the transverse MRI images using imaging processing functions on a Philips workstation. At each MR image slice level, fat pixel intensity was segmented and used to determine the total volume of fat for the slice. Measurements were repeated at completion by an experienced doctor. Fat within bone marrow and paraspinal muscles was excluded from the measurement. SAT was defined as fat superficial to the abdominal and back muscles. VAT was defined as the intra-abdominal fat bound by parietal peritoneum or transversalis fascia. Total intra-abdominal fat represented the sum of both SAT and VAT. Figure 1 shows a typical example of the quantitative analysis of abdominal fat content extracted from an MR image using segmentation.

A typical example of a segmented abdominal T1-weighted magnetic resonance image. Subcutaneous fat and visceral fat were separated, and the content of each was quantified.
1 H-MRS for IHTG content
Hepatic fat content was measured by 1 H-MRS in all 10 subjects. Sagittal, coronal, and transverse images of the liver were obtained in all patients. Briefly, image-guided, localized 1 H-MRS scans were acquired using a sense torso coil with volumes of interest (22 mm × 22 mm × 22 mm) centered within the right lobe of the liver, avoiding major blood vessels, intrahepatic bile ducts, and the lateral margin of the liver (Fig. 2, left). To control respiratory motion, a respiratory triggering mode was employed. Hepatic spectra were acquired using the point-resolved spectroscopy technique (TR = 2000 ms, TE = 35 ms, flip angle = 90 degrees, 16 acquisitions, 1024 data points, spectral width = 2000 Hz). Fully automated high-order shimming was performed on the volume of interest to ensure maximum field homogeneity. Unsuppressed water spectra were acquired in vivo for use as the internal standard. Areas of resonance from the protons in water and the methylene groups in fatty acid chains of hepatic triglycerides (Fig. 2, right) were evaluated using MRS processing functions on a Philips workstation. MRI and 1 H-MRS processing were performed by an experimenter blinded to treatment allocation.
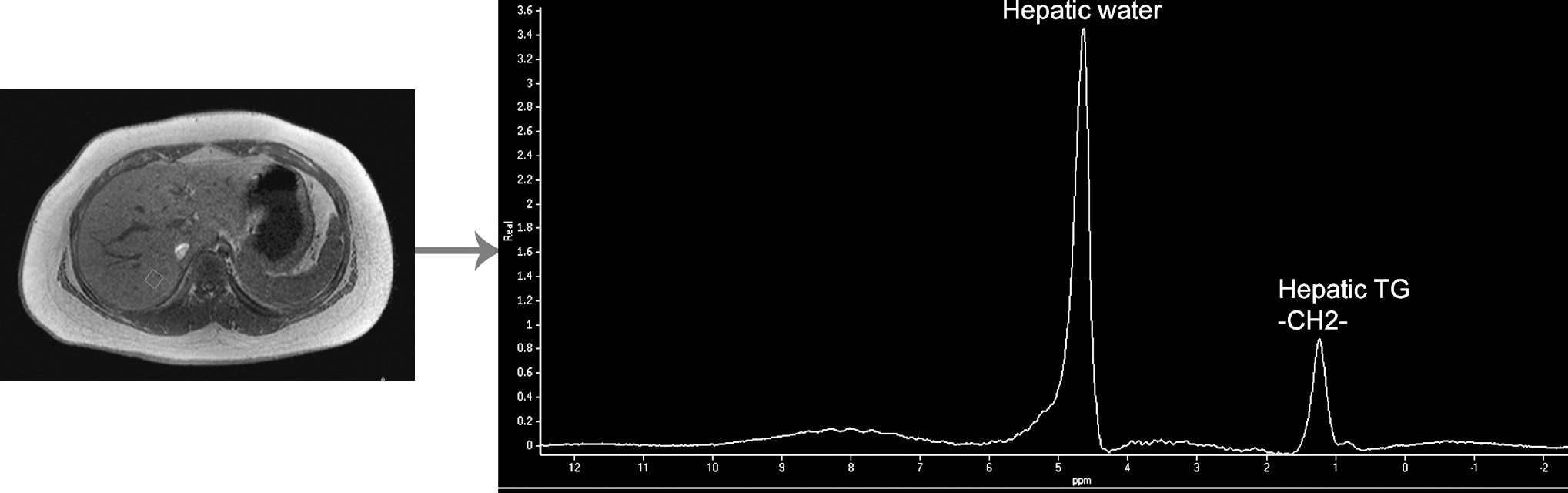
Experimental setup for measurements of intrahepatic triglycerides (TG) content by proton magnetic resonance (MR) spectroscopy.
Calculations
The volume of abdominal VAT or SAT in cubic centimeters was calculated by (sum of area of abdominal VAT or SAT in all slices in cm2) × 0.5 cm. Total intra-abdominal fat represented the sum of both VAT and SAT. The abdominal visceral to subcutaneous fat ratio (V/S) was calculated by dividing the baseline VAT in cubic centimeters by the baseline abdominal subcutaneous area, also in cubic centimeters. The percent change from baseline for selected variables was calculated as [(final – initial)/initial] × 100%.
Spectroscopic IHTG content was calculated as a ratio of the area under the methylene peak to that under the methylene and water peaks (×100 = %IHTG). 41
Statistics
SPSS11.5 for Windows was used for data analysis. The distribution of the data was tested for using the Shapiro-Wilk normality test. All values are expressed as means ± standard error. The effects of acupuncture therapy on variables were compared by paired t tests for repeated measurements in each individual before and after weight-loss intervention. Changes in all variables are expressed as a percentage. Relationships between variables were determined by Pearson's correlation coefficients. Statistical significance was accepted at p < 0.05.
Results
Anthropometry
In response to the acupuncture therapy, BMI decreased by 3.5% (p = 0.005). Decreases in body weight (-2.13%), waist circumference (-1.44%), hip circumference (-0.33%), and WHR (-0.99%) were also observed, although these were not significant (p > 0.05) (Table 1).
Values are means ± standard error.
N, number of subjects; BMI, body–mass index; WC, waist circumference; HC, hip circumference; WHR, waist circumference/hip circumference; % change, [(final – initial)/initial] × 100%.
Abdominal fat
The abdominal total adipose tissue decreased by 10.45% (p = 0.001), VAT decreased by 16.04% (p < 0.0001), and V/S decreased by 10.59% (p = 0.007). The biggest decrease was in the level of VAT. Decrease in SAT (-5.63%) was also observed, although it was not significant (p = 0.106) (Table 2).
Values are means ± standard error.
n, number of subjects; VAT, visceral adipose tissue; SAT, subcutaneous adipose tissue; TAT, total adipose tissue; V/S, VAT/SAT; IHTG, intrahepatic triglyceride; % change = [(final – initial)/initial] × 100%.
IHTG content
Decrease in IHTG (-9.03%) was also observed, although it was not significant (p = 0.071) (Table 2).
Relationship between variables
There was a significant correlation between the level of abdominal fat content and anthropometric parameters except WHR. There was a significant correlation between weight and SAT or VAT both before (r = 0.848, p = 0.002; r = 0.669, p = 0.004) and after (r = 0.877, p = 0.001; r = 0.833, p = 0.003) therapy. There was a significant correlation between BMI and SAT or VAT both before (r = 0.926, p < 0.0001; r = 0.388, p = 0.050) and after (r = 0.941, p < 0.0001; r = 0.701, p = 0.024) therapy. There was a significant correlation between waist circumference and SAT or VAT both before (r = 0.905, p < 0.0001; r = 0.695, p = 0.003) and after (r = 0.943, p < 0.0001; r = 0.850, p = 0.002) therapy. There was also a significant correlation between hip circumference and SAT or VAT both before (r = 0.922, p < 0.0001; r = 0.643, p = 0.005) and after (r = 0.889, p = 0.001; r = 0.808, p = 0.005) therapy. There was no significant correlation between WHR and SAT before (r = 0.075, p = 0.836) and after (r = 0.078, p = 0.831) therapy. There was a significant correlation between WHR and VAT before (r = 0.630, p = 0.006) but not after (r = 0.031, p = 0.932) therapy (Table 3). There was no significant correlation between IHTG and anthropometric parameters or abdominal fat content before and after therapy (p > 0.05) (Table 4).
r, Pearson's correlation coefficients; BMI, body–mass index; WC, waist circumference; HC, hip circumference; WHR, waist circumference/hip circumference.
IHTG, intrahepatic triglyceride; r, Pearson's correlation coefficients; BMI, body mass index; WC, waist circumference; HC, hip circumference; WHR, waist circumference/hip circumference; SAT, subcutaneous adipose tissue; VAT, visceral adipose tissue.
Discussion
Acupuncture has been used to treat obesity. A systematic review of four randomized controlled trials of acupuncture for weight loss concluded that there was no clear evidence of its effectiveness. 42 However, recent studies have shown that acupuncture can markedly reduce body weight, BMI, and WHR in patients with simple obesity. 13 –17 In agreement with previous studies, our findings also suggest that acupuncture is a useful method for reducing BMI in obese children. Decreases in both body weight and WHR were also observed, although these were not significant.
In this study, it was shown that acupuncture therapy can have beneficial effects on abdominal adipose tissue in obese children. There was a significant correlation between the level of abdominal fat (SAT, VAT) and anthropometric parameters (weight, BMI, waist circumferences, hip circumferences). To our knowledge, these are the first data on the effect of acupuncture therapy on abdominal adipose tissue in children. The study data suggest that acupuncture therapy results in decreased VAT but not SAT. The preferential reduction in VAT may be explained by previous observations, which suggest that VAT is more sensitive than SAT to lipolytic stimulation, 43 more metabolically active, 44 and less resistant to insulin suppression. 45 A reduction in VAT has important clinical implications. The excess accumulation of intra-abdominal adipose tissue seems to be associated with metabolic disorders in obesity. In particular, VAT has been implicated as a major risk factor for several diseases, including type 2 diabetes, coronary heart disease, hypertension, and stroke. 9,10,20 –22 VAT is directly associated with the negative health consequences of obesity. Therefore, therapies that selectively target VAT may be more effective at reducing the complications of obesity. One can make the argument that a reduction in VAT should be included as an important measure when assessing any intervention's ability to improve the metabolic consequences of obesity. 46 Therefore, a reduction in VAT has become a key therapeutic goal in the management of obesity. 47,48 According to recent studies, VAT is highly responsive to exercise and dietary interventions, 49 –51 and to a variety of pharmaceuticals. 52,53 It is thus increasingly desirable to find effective methods of monitoring changes in VAT in both clinical interventions and epidemiologic studies.
The mechanism behind the reduction in abdominal adipose tissue with acupuncture therapy remains unclear. For one thing, acupuncture can increase excitability of the satiety center of the ventromedial nucleus of the hypothalamus, so as to control the excessive appetite. 54,55 For another, under the influence of internal and external factors, the disorder of visceral functions leads to accumulation of dampness, phlegm, and lipid in the body and results in obesity. As to the treatment of obesity in traditional Chinese medicine, the therapeutic principle is to mainly regulate the spleen, stomach, and kidney. Treatment plans and acupuncture points are highly individualized, based on the location and the deficiency/excess of qi. Accordingly, a different set of points would be used, depending on which organ(s) needed to be “energized” or “inhibited.” 11 Thus, points along the Stomach Meridian of Foot-Yangming and the Spleen Meridian of Foot-Taiyin can be targeted during acupuncture to regulate the stomach and spleen. In this manner, acupuncture could regulate lipid metabolism and endocrine levels.
In this study, it was also observed that acupuncture therapy did not alter 1 H-MRS–measured IHTG (p > 0.05). There was no statistically significant correlation between IHTG and anthropometric parameters or abdominal fat content. The reasons for this are not immediately apparent, though several possibilities exist. First, recent studies have suggested that IHTG content may be altered by a single meal. It has been shown that there is rapid incorporation of dietary fatty acids into the hepatic triglyceride pool in both normal and diabetic subjects. 56 However, we scanned our subjects following a 10-hour overnight fast to minimize any potential effects. Second, IHTG reduction is believed to be hampered in individuals whose fatty infiltration has already begun to progress to fibrosis, compared to those who solely have steatosis. Third, consistent IHTG reduction resulting from weight loss may need a long-term intervention. In this study, acupuncture therapy was adopted for only 1 month, which is a short-term course. Finally, this study is a relatively small sample size. The findings are preliminary and should be confirmed in studies with larger cohorts.
Conclusions
In conclusion, this study provides the first direct experimental evidence demonstrating that acupuncture therapy significantly reduces BMI and abdominal adipose tissue. The greatest effect was seen in the reduction of abdominal VAT content, without significant changes in body weight, WHR, abdominal SAT, and IHTG content. Thus, the ability of acupuncture therapy to selectively target VAT reduction should become more important and more popular in the decades to come. Larger-scale studies are clearly required to elucidate this further. Also, future work to confirm the long-term efficacy of acupuncture therapy on abdominal fat and hepatic fat content in obese children is needed.
Footnotes
Acknowledgments
We are grateful to all of the children who participated in this study. This study was supported by grants from Beijing Municipal Natural Science Foundation (7092091).
Disclosure Statement
No competing financial interests exist.