
Abstract
Objectives:
This pilot study on the use of traditional Chinese acupuncture (TCA) to treat chronic stress explored the use of the diurnal salivary cortisol profile as a potential outcome measure.
Design and methods:
Adult volunteers (n=18) with high self-reported stress levels, ascertained by screening with the Perceived Stress Scale 14, were randomized into three groups. Group 1 received weekly sessions of TCA for 5 weeks; Group 2 received attention only weekly (practitioner present and subject supine) for 5 weeks, and group 3 acted as a waiting-list control. A diurnal cortisol profile was constructed for each individual at nine data points: two at baseline, five during the intervention, and two postintervention. A salivary cortisol sample was taken at four time points (on waking, 30 minutes, 3 hours, and 12 hours after waking).
Outcome measures:
Salivary cortisol concentrations were measured using a high-sensitivity salivary cortisol enzyme immunoassay.
Results:
The cortisol awakening response showed an average increase during the intervention for both TCA and attention groups, indicating that for these two groups the cortisol response had normalized and they were in a lower state of stress. These trends did not reach statistical significance due to individual variation and the small number of study participants. The control group showed an overall decrease in the average morning increase over the same period. No significant difference in the day decline in cortisol was found between groups at any point in the study.
Conclusions:
This pilot study suggests that TCA could reduce stress and increase the morning rise of the cortisol profile; however, this was not distinguishable from the effect of attention only. Further work with a larger sample is necessary to provide a definitive answer regarding whether this could be sustained with more TCA treatments. The morning cortisol increase could be a useful outcome measure for monitoring the effects of treatment on perceived stress.
Introduction
In recent years, cortisol concentration has been used as an objective biochemical parameter, and has been used in research in complementary medicine, including mindfulness-based stress reduction, transcendental meditation for stress, as well as cognitive behavioral therapy. 9 –11 Results have shown that these techniques relieved some of the negative psychologic consequences of stress and correspondingly lowered levels of the hormone cortisol. Research using a mixed cross-sectional and longitudinal repeated-measures design found that salivary cortisol secretion in a kinesthetic meditation group was lower in the afternoon on the day of the final kinesthetic meditation session compared to on a typical day in the same week. 12 Other research has indicated an instantaneous decrease in cortisol concentration after t'ai chi 13,14 and yoga, 15 –17 and have reported that the size of the cortisol response to a standard stressor can be attenuated by interventions such as cognitive behavioral therapy 16,18 and transcendental meditation. 17
Laboratory studies on the effect of acupuncture on cortisol concentration modeling stressful circumstances in animals have suggested that acupuncture can decrease cortisol concentrations. 19 –21 Few clinical research articles on acupuncture have used cortisol as a measurement. These studies investigated the difference in cortisol concentration before and after acupuncture. For example, research by Akimomo et al. showed an increase of salivary cortisol inhibited by acupuncture. 22 Uskok et al. 23 reported that cortisol is valid as a useful outcome measure. There is no research on acupuncture on diurnal salivary cortisol profile in stressed people.
The literature indicated that the diurnal profile of the salivary cortisol concentration could potentially be useful as an objective measure. 3,4 This study was the first time that the diurnal salivary cortisol profile had been used as a biochemical parameter to monitor any changes as a result of using traditional Chinese acupuncture (TCA) for chronic stress in adults and to determine whether TCA could normalize the diurnal salivary cortisol profile of chronically psychologically stressed adults. The protocol for collecting saliva samples (four points in time on each day of 9 separate days) was established after reviewing the literature for appropriate measurement points to demonstrate the diurnal profile of salivary cortisol concentration in this study. 4,24
Methods
This pilot study was approved by the Research Review Committee of Thames Valley University prior to initiating the study. Written consent to participate in the study was obtained from all participants.
Study participants
Study participants were volunteers from the university staff. Volunteers were screened for stress using the Perceived Stress Scale 14 (PSS-14), and invited to take part in the study if they scored 20 or more 25 ; were not currently receiving a complementary therapy or other treatment for stress and its related symptoms; had no serious or life-threatening medical conditions; and had not experienced a severe life event in last month. Volunteers scoring below 20 on the PSS were thanked for their time but were not invited to take part in the study. The PSS-14 was used to measure subjects' stress levels during the 8-week study. Subjects were randomized into three groups (TCA, attention only, and control groups) by using block randomization.
TCA group
The TCA group (n=6) received weekly sessions of TCA for a period of 5 consecutive weeks.Acupuncture treatment for each subject used a standard acupoints prescription and supplementation with other points according to the TCM diagnosis on the day of treatment. Acupuncture was provided by a Chinese-trained traditional acupuncturist.
The standard acupoints prescription for the treatment of stress consisted of DU20, DU24, EX-HN3, LI4, PC6, ST36, and LR3. In addition to these main points, the following supplementary acupoints were selected according to the individual's different TCM diagnostic patterns. Additional points were also added if there were any specific health issues reported during an individual's consultation: • Liver qi transforming into Fire: LR2, PC5 • Liver invading Spleen and Stomach: ST25, RN12 • Gallbladder qi Deficiency: GB34, ST40.
Attention group
The 6 subjects in the attention group were informed that they would receive weekly sessions of “relaxation” for a period of 5 consecutive weeks, but no acupuncture. Subjects attended the clinical site once a week. The researcher carried out a general consultation (in a Western style of asking about their general health and making notes, but did not include Chinese medicine consultation techniques such as tongue and pulse diagnosis). The subjects lay on the couch for a similar amount of time as the subjects in the TCA group. The researcher managed the subjects in the attention group and the subjects in the TCA group in the same manner (apart from the TCA, which also included a Chinese medicine consultation).
Control group
The 6 subjects in the control group acted as a waiting-list control and did not attend the clinical site but completed the same questionnaires and provided cortisol samples, following the same protocol as the other groups.
PSS-14
The PSS-14 is a 14-item questionnaire with a 5-point scale that has been shown to possess good reliability and validity. 25 In this study, the PSS-14 was used as one of the criteria for subject recruitment and in addition as a screening measurement to measure the self-reported stress levels during the study period.
The PSS-14 was completed by the three groups on the day of commencement of the study, which provided the baseline data for the study, and the day after the completion of the 5-week intervention and in the subsequent 2 weeks of follow-up.
Collection of salivary samples
Salivary samples were collected on 9 separate days over a total period of 8 weeks for all three groups. The collection days were as follows: the 2 consecutive days prior to commencement of the study, the day following each session of acupuncture or attention during the 5 weeks, and on the same day of the week for each of the 2 weeks after the intervention period. For the waiting-list control group, the samples were taken at the same time points. All collection dates were working days rather than weekends and off-days.
A salivary cortisol sample was taken four times on each sampling day for 9 separate days over a total period of 8 weeks. The four daily times were the following: immediately upon waking in the morning, 30 minutes after waking, 3 hours after waking, and 12 hours after waking. The exact time the sample was taken was recorded.
Salivary samples were collected by participants using the salivettes, which were dated, numbered, and marked with each individual's unique code number. Salivary collecting followed the Salimetrics recommended protocol. 26 Subjects were asked to collect their saliva samples no earlier than 30 minutes after eating or drinking, and before they brushed their teeth in the morning. Participants were asked to rest for 30 minutes prior to the collection of samples 3 and 4. Collection of saliva consisted of placing the inner cotton wool swap of the salivette under their tongue for 2 minutes, chewing it to make sure it had fully absorbed all the saliva, replacing it in the inner sleeve of the salivette, and then replacing the lid.
The samples were kept refrigerated by the subjects at 0–4°C overnight and then returned to the researchers the following day. They were then stored at −80°C until analysis. All samples were analyzed within 6 months of the end of the study.
Salivary samples analysis
An independent biochemist at Imperial College, London carried out the double-blind analysis of the salivary cortisol samples. The salivary cortisol concentration was analyzed by using a high-sensitivity salivary cortisol enzyme immunoassay by Salimetrics LLC (USA). The standard range in assay was 0.003 μg/dL – 3.000ug/dL (0.083nmol/L – 82.77nmol/L). 26
Statistical analysis
Demographic data for each group were compared using analysis of variance for the age of the participants and Fisher's exact tests for categorical data due to the small samples sizes (Table 1). The Kruskal-Wallis test was used to compare PSS scores between the study groups. Because cortisol data are typically positively skewed, a square-root transformation was carried out before analysis to normalize the data. One (1) set of saliva cortisol data was excluded from analysis because the laboratory found that the concentration in most, but not all, of that participant's samples exceeded the maximum range of the Salimetrics cortisol standard curve, indicating intermittent contamination. The mean CAR for each group was then calculated by subtraction of the mean cortisol concentration at 30 minutes from the awakening cortisol concentration (Δ Cort=Cort t30 – Cort t0). One-way ANOVA was used to test for differences within and between groups. The decline in cortisol concentration over the day (excluding the awakening rise) was calculated by subtracting the cortisol concentration of the last sample at+12 hours from the awakening concentration (Day Decline12h=Cort t0 – Cort t12). The same procedure was used to calculate the decline from 3 hours to 12 hours postawakening (Day Decline3–12h=Cort t3- Cort t12). An average cortisol concentration over the awakening to+12 hours period was also calculated using the mean data for awakening,+3 hours and+12 hours (Day Average=[Cort t0+Cort t3+Cort t12]/3). Spearman rank correlation was used to test for a relationship between the day average cortisol concentration and time of awakening.
TCA, traditional Chinese acupuncture; NS, not significant; SEM, standard error of the mean.
Results
A total of 18 participants (15 female, 3 male; mean age 42.3±2.7 years old [range 19–58 years]) were recruited and completed the study (see Table 1 for demographic characteristics). The mean age difference between each of the study groups did not reach statistical significance. In addition, there were no statistically significant differences in gender, occupation, and acupuncture experience between the three groups. Due to randomization, 2 subjects in the attention group were smokers and none were smokers in the other two groups. A total of 648 samples were collected and analyzed. Some, but not all, of the salivary samples for 1 participant in the TCA group were beyond the range of the cortisol standard curve, indicating intermittent contamination and could not be used, giving 5, 6, and 6 subjects for the TCA, attention, and control groups, respectively.
PSS-14
The PSS-14 mean scores for the three groups at the preintervention baseline and after the 5-week intervention (postintervention) were analyzed. 25 After the 5-week intervention period, the PSS-14 scores decreased for all three groups, with the mean decrease for both the TCA (13.9%) and attention (18.9%) groups decreasing more than the control group (3.8%). However, the difference between the pre- and postintervention period within the groups and between the groups did not reach significance in this small study. The mean PSS-14 score for the TCA group was, however, the lowest of the three groups both pre and post the 5-week intervention period. After the 5-week intervention, the PSS-14 scores dropped below 20 for 2 of the participants in the TCA group only; therefore, these 2 participants could be considered as no longer reporting above-average stress levels.
Diurnal profiles of mean salivary cortisol concentration
The data in Tables 2, 3, and 4 reflect the large variations in cortisol concentration that are known to occur in the normal human population. 24 The difference between the groups did not reach statistical significance due to individual variation within groups in this small sample.
Data are presented as mean (±standard error of the mean).
TCA, traditional Chinese acupuncture.
Data are presented as mean (±standard error of the mean).
Data are presented as mean (±standard error of the mean).
Cortisol awakening response
At baseline, the mean scores of CAR in the TCA group were much higher than for the other two groups. For the attention group, they were much lower than in the other two groups. Therefore, the baseline (2 days and 1 day preintervention) was excluded, and the analysis focuses on the differences among the trends of the morning rise of cortisol concentration in the three groups during the intervention period. The morning rise of salivary cortisol concentration for each group is presented graphically in Figures 1, 2, and 3.
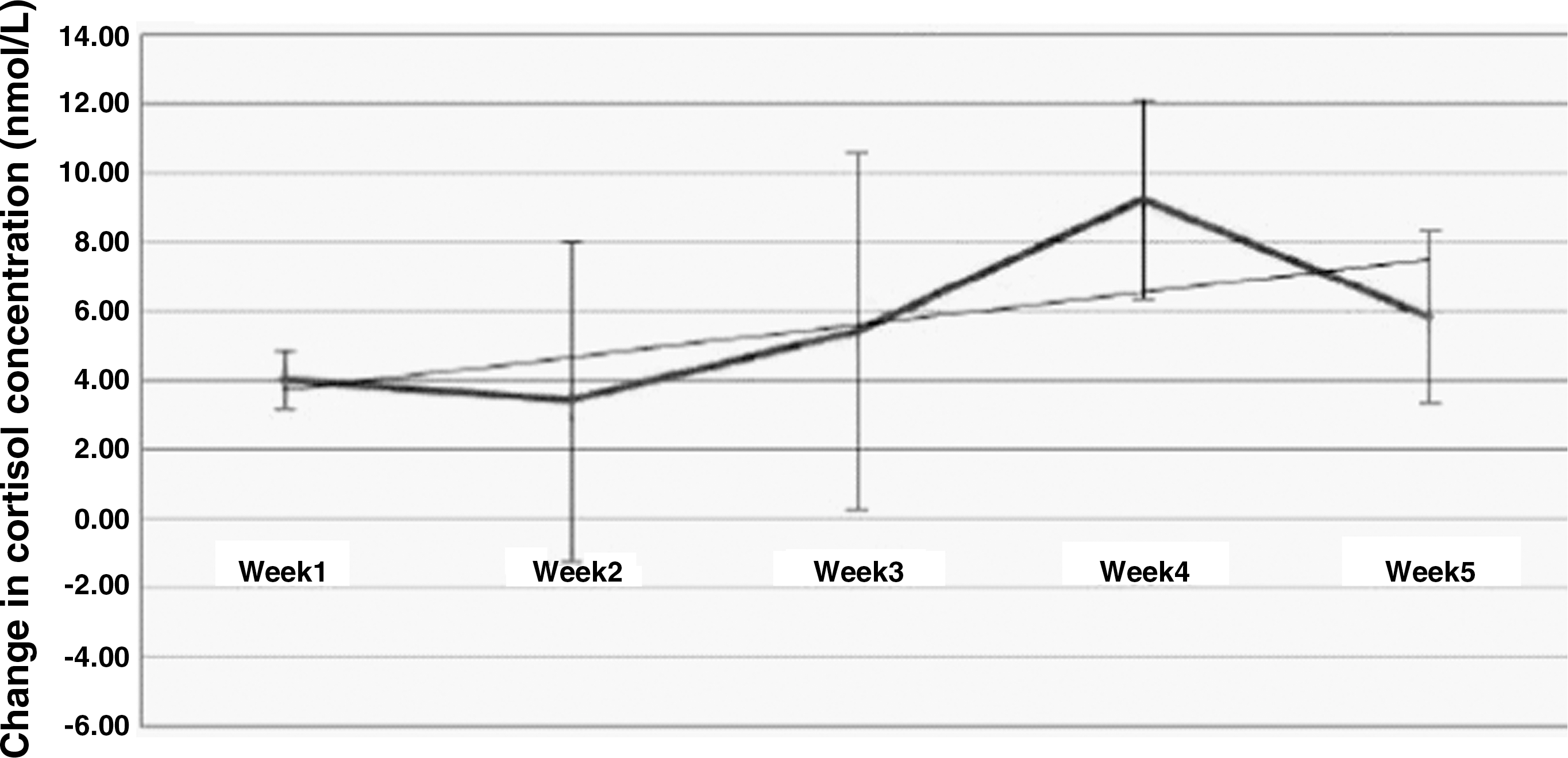
Mean morning rise of cortisol concentration during the 5-week intervention period for the traditional Chinese acupuncture group. Data are presented as mean±standard error of the mean.
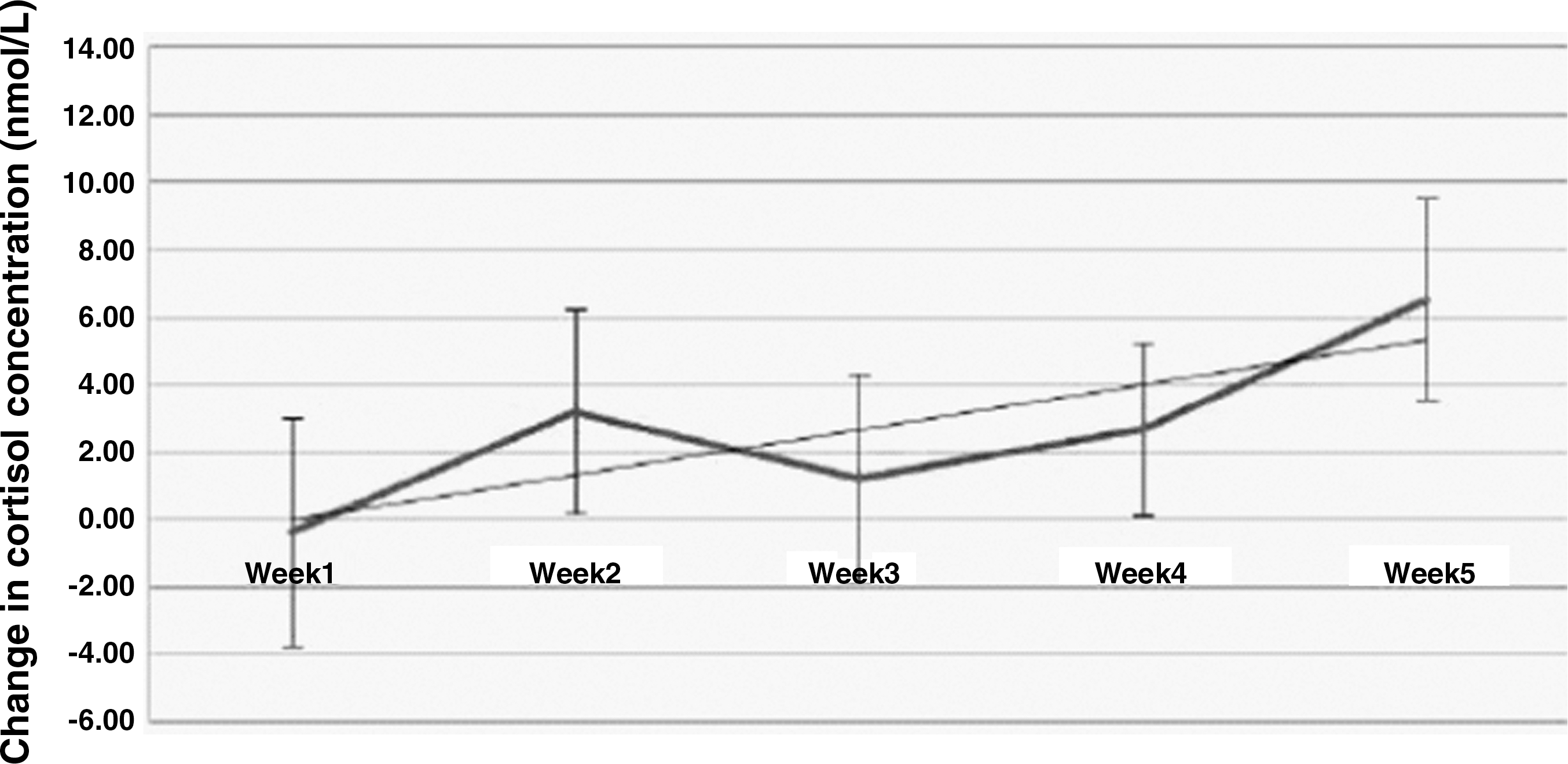
Mean morning rise of cortisol concentration during the 5-week intervention period for the attention group. Data are presented as mean±standard error of the mean.
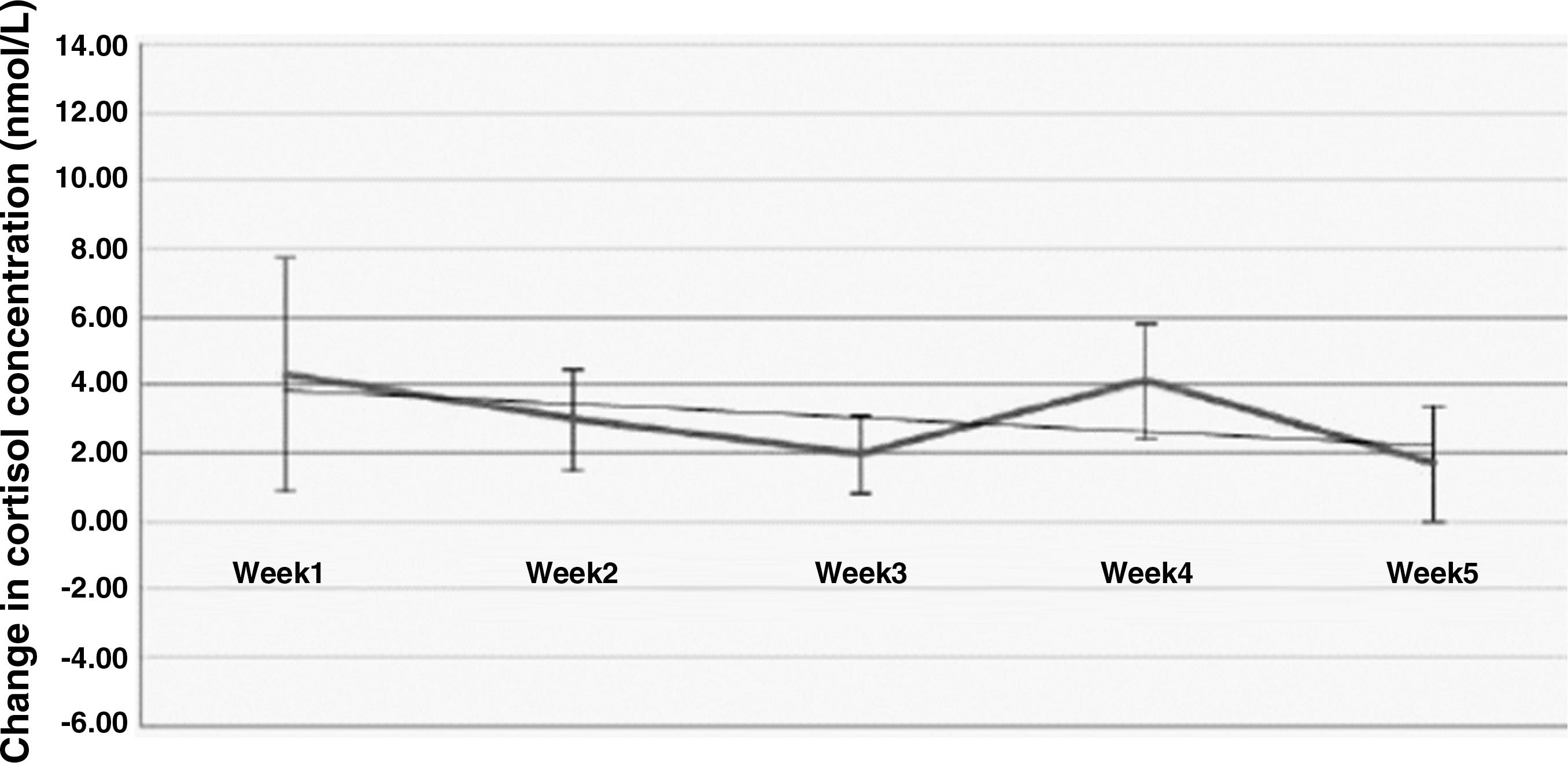
Mean morning rise of cortisol concentration during the 5-week intervention period for the control group. Data are presented as mean±standard error of the mean.
Figures 1, 2, and 3 illustrate that the TCA group had the greatest level of change in week 4 (9.28 nmol/L). Generally during the 5-week intervention period, the morning rise in the TCA group was greater than for the other two groups (except in week 5 when it was lower than for the attention group). The CAR showed an increase during the intervention in the TCA group and the attention group, with both groups showing upward trends. The control group showed an overall decrease in the mean morning rise during the same period.
In week 1 of the intervention period, the TCA group and the control group showed a similar mean morning increase, whereas the level for the attention group was much lower than the other two groups. Therefore, Figures 1, 2, and 3 indicate that the TCA group had a greater increase in the morning rise than the control group during the 5-week intervention period. The attention group also showed an increase in the mean morning rise over the period of the intervention. No statistically significant difference was found in the CAR between the TCA and attention-only groups due to the variability of the data within groups and the low power due to the small sample size.
Day decline in cortisol concentration
Tables 5, 6, and 7 present the mean day decline for 12 hours, day decline for 3–12 hours, and day average cortisol for the three study groups each week. No significant difference in the day decline in cortisol was found between groups at any point in the study.
Data are presented as mean (±standard error of the mean).
Data are presented as mean (±standard error of the mean).
Data are presented as mean (±standard error of the mean).
Day average cortisol concentration
A Spearman rank correlation was carried out on the data from the pretreatment samples between the day average cortisol concentration and the time of waking for all participants. A significant negative relationship was found between the day average cortisol concentration and the time of waking 2 days prior to the study (r s=–0.55, p=0.010) and 1 day prior to the study (r s=–0.541, p=0.012). One-way ANOVA revealed no significant difference in day average cortisol between groups at the end of the treatment period.
Discussion
The diurnal cortisol profiles reflected considerable individual variability. The combined data show a diurnal pattern as reported by other researchers overall. Because a stressed group of individuals were selected for study, the combined data reflect the typically reduced CAR. 4 However, for some individuals the diurnal salivary cortisol profile did not appear abnormal before the intervention, especially for the TCA group, and this was reflected in the mean data (Table 2). This indicated that either the stress the participants were experiencing was not at a level great enough to disturb the hypothalamic–pituitary–adrenocortical axis (HPA) or the HPA was not sensitive enough to reflect the subjects' self-reported stress. Granath et al. 27 demonstrated similar results using the PSS in a study comparing self-rated stress with two treatment groups (yoga and cognitive behavioral therapy). Both the TCA and attention groups in this study showed an overall increase in the morning rise, suggesting a normalization of diurnal profile, whereas the control group showed an overall decrease in the average morning rise, suggesting a more stressed diurnal profile. These preliminary observations suggest that a more simplified and less costly cortisol sampling schedule (the first two data points of the diurnal profile only) could be used as a research tool in subsequent studies. The changes observed in the average morning rise over the period of the study are worthy of further investigation.
The PSS has been found to correlate with “number of life events” and has a slightly greater correlation with “impact of life events.” 25 The PSS is more successful at predicting a variety of health issues and health care outcomes than are measures of specific life events that focus on the number rather than the appraisal of the stressful nature of events. In this study, the PSS-14 was useful for recruiting participants and measuring the participants' self-reported stress levels. A potential confounder in this study was the fact that a sudden announcement of compulsory redundancies was made as the study began. This would have had a likely impact given the age of some of the participants. Although the scores of the PSS-14 at the baseline were not completely reflected by the morning rise of salivary cortisol concentration in TCA and control groups, the trends of the scores between pre- and postintervention in three study groups were the same as the changes of the morning rise of salivary cortisol concentration in three groups during the study. Because this is a pilot study and the cost of salivary cortisol analysis is high, the sample size in this study was small and significant results were not identified. Other researchers have reported this difficulty. A recent small study (n=18) investigated that when acupuncture was given to dysphonic patients, the cortisol level immediately prior to and post-treatment showed a reduction in cortisol concentration during treatment but returned to pretreatment level within 10 minutes. 24 The authors could not distinguish between the groups, but combined data gave a significant result. The power calculation indicated that a sample size of 106 patients would be required in order to detect a significant difference between treatment groups. However, a limitation of the study by Kwong and Yiu 24 was that it did not include a waiting-list control. In the current study, which included the waiting-list control, the authors were able to demonstrate a trend indicating a reduction in stress for both groups in contact with the practitioner in comparison with the waiting-list control.
Aromatherapy provided to patients during a treatment regarded as stressful by patients showed that cortisol levels decreased significantly during aromatherapy treatment. 28 This research suggests that there is potential for use of such treatments in an acute situation; however, whether these effects may be sustained if regular treatment was provided is currently unknown. Similarly, salivary cortisol levels and self-reported stress were found to be reduced 40 minutes following visits to an art gallery. 29 This suggests that there are various potential interventions that can reduce acute stress. Research evidence suggests that psychologic variables including stress and other conditions such as novelty, unpredictability, and uncontrollability are associated with increases in HPA activity and cortisol release. 30 However, in many of these studies, a substantial percentage of subjects did not respond (i.e., do not show elevated cortisol levels) after exposure to a stressor, possibly owing to strong anticipatory effects. 31 The sensitivity of the HPA to a variety of different conditions and events may make it less useful as a specific indicator of stress, and the interpretive issues raised by nonresponders or even people who show inverted responses made the cortisol measures difficult to interpret.
Research by Bartels et al. on 12-year-old children showed that a significant genetic contribution was found in the variation of basal cortisol levels in the morning and afternoon samples. 32 Other research has suggested that childhood family environments represent vital links for understanding mental and physical health across the lifespan and disruptions in the stress-responsive biologic regulatory systems, including the sympathetic–adrenal–medullary system and HPA functions. 33 Therefore, genetic and environmental factors could affect stress levels and influence individual differences in the cortisol concentration. An individual with a stable environment will respond less to stress. Wichers et al. found that genetic liability to depression was in part expressed as the tendency to display negative affect in response to minor stressors in daily life. 34 Human study groups are not genetically identical in the way animal models are, so the genetic polymorphisms natural in any population make interpretation of data more problematic. 35,36 Other factors that affect the salivary cortisol response could include gender, 37 age, 38 exercise, smoking, 26 and awakening time. Although the groups in this study were matched, the sample population was largely female; therefore, menstrual cycle and oral contraceptive use could have also influenced cortisol secretion. 39 Despite the large variation in cortisol concentration between the subjects in this pilot study, changes in the CAR could still be seen during the treatment period. In this study, apart from TCA group, the attention group also shows an upward trend in the morning rise of salivary cortisol concentration, which suggests a decreased stress level. It is clear that a short period of relaxation during the working day and the attention of a skilled practitioner may also have a positive effect on perceived stress, and evidence from other relaxation-based interventions support this. 16 –18 The attention group was provided with a time-out period, which they may have used for reflection and relaxation, providing them with a coping strategy that was more effective than the equivalent period for the TCA group receiving the more invasive acupuncture treatment. There could also have been some concern about the use of needles in the TCA group. In addition, the fact that there were only small differences observed between the TCA and the attention groups may have been due to a suboptimal intervention; five sessions of TCA may be insufficient to deal with chronic stress. Other research into potential interventions for stress (yoga) using inflammatory and endocrine markers has suggested that only regular practice can provide substantial health benefits by reducing stress. 40 The authors' previous article on this study reported that the TCA participants reported improvements in their general health and a range of other symptoms which were treated pragmatically during their individual consultations. These provided an added benefit that would not have been captured using a cortisol measure. 25 A larger trial would be necessary to investigate these aspects further.
Recent research by Streeter and co-workers used a different technique to test changes in affect in relation to two different potential therapeutic treatments. 41 They measured brain γ–aminobutyric acid (GABA) levels by magnetic resonance spectroscopy, which demonstrated positive correlations between changes in mood and GABA levels. This technique could provide a future direction for research into patient outcomes, but is costly for a clinical application.
Conclusions
In conclusion, although in this study trends did not reach statistical significance due to individual variation in this small sample, the normalization of the CAR observed in the TCA group and the attention group compared to the control group during the intervention period suggested that these interventions could affect the morning rise of cortisol concentration. The CAR could therefore be a useful outcome measure to monitor the effects of treatment on perceived stress with important implications for the treatment of stress. It also suggests that the cortisol profile had been normalized by the effects of both the TCA and attention interventions. This could have led to longer-term improvements in stress and coping that were not measured during this study. The number of treatments may be an important factor, with the possibility that more TCA treatments could sustain the effect over a longer period.
The change in the morning rise of cortisol concentration is substantiated in this study. Future work could restrict measurements to the first two collecting time points (immediately upon waking in the morning and 30 minutes after waking). This would reduce study costs to the investigator and make collection easier for subjects. A larger study is required to confirm these observations. This study supports the acute use of acupuncture to reduce stress as shown in other complementary interventions, but further studies are necessary to explore how this can be maintained and the level of treatment required.
Footnotes
Acknowledgments
We thank study participants who gave up their time to be part of the study, and Kieran O'Donnell at Imperial College, London for expertise in measuring the cortisol measurements in this study.
Disclosure Statement
No financial conflicts exist. All authors have no conflicts of interest.