
Abstract
Objectives:
Japanese style, superficial acupuncture (SA) has been clinically evaluated for its therapeutic benefit, yet the neurophysiologic responses associated with SA remain unclear. This study was performed to measure changes in regional cerebral blood flow (rCBF) following SA at LI-4 and LI-11 in healthy volunteers using single photon emission computed tomography (SPECT). Changes in SPECT activity following Japanese style SA were compared to previous reports of SPECT changes following electroacupuncture (EA) at the same acupoints.
Design and setting:
Ten (10) healthy volunteers were enrolled for this study. A few days after the baseline brain SPECT, SA was performed at LI-4 and LI-11 for 15 minutes and a second brain perfusion image was acquired for each subject. We used SPM2 to analyze the changes in rCBF after SA through a paired t test. In addition, the differences of rCBF changes between SA and EA were compared using a two-sample t test.
Results:
Cerebral blood perfusion significantly increased after SA in the left superior frontal gyrus, left middle cingulum, left insular, right medial orbital frontal gyrus, and right middle cingulum (paired t test, uncorrected p < 0.005), while no regions showed a significant decrease. The results comparing poststimulation images between SA and EA demonstrated that the perfusion in the right lingual, both thalamus, left middle temporal gyrus, left insula, and both cerebellum were significantly increased in SA compared with EA (false discovery rate [FDR] corrected p < 0.05).
Conclusions:
There were specific increase patterns of rCBF following SA at LI-4 and LI-11, which were similar to those following EA. However, there were significant differences in the decrease pattern of rCBF between SA and EA, which might be due to the difference of the strength of acupuncture stimulation between the two methods. These results may contribute to developing a better strategy to a select stimulation method in acupuncture therapy.
Introduction
Recently, a functional magnetic resonance imaging (fMRI) study indicated that there were no significant differences in the imaging patterns associated with SA and DA needling at LI-4. 8 It can be argued that the differences between the two depths of needling may be too subtle for detection in an fMRI due to the relatively short-term time span of a block design, or that the differences may only emerge over time. However, investigation of the long-term impacts of acupuncture using single photon emission computed tomography (SPECT) and positron emission tomography (PET) revealed that acupuncture treatment may alter brain activity. 9 –13 We previously reported specific patterns of regional cerebral blood flow (rCBF) and glucose metabolism after 15 minutes of electroacupuncture (EA) at LI-4 and LI-11 using SPECT and PET. 12 In traditional Korean medicine, these acupoints are frequently used for the rehabilitation of poststroke paresis, regardless of whether manual (superficial or deep) or electrical stimulation methods are used. 14 However, no previous study has investigated the cerebral blood perfusion changes after SA at LI-4 and LI-11 using SPECT, nor has any comparison been made between the perfusion changes after SA and those following EA.
The primary aim of this investigation was to use SPECT to measure the changes in rCBF after SA at LI-4 and LI-11 in healthy volunteers, and compare the differences between those changes and the changes that occurred after EA at the same acupoints.
Materials and Methods
Subjects
We enrolled 10 healthy volunteers (7 men and 3 women; age, 23–28 years) in this study. None of the enrolled subjects had a specific history of cerebral disease. Smoking was prohibited during the 48 hours preceding the study. The study protocol was approved by the local institutional review board. All subjects provided written informed consent in accordance with the ethical guidelines set forth in the 1975 Declaration of Helsinki.
Brain Perfusion Image Acquisition
Acquisition of baseline brain perfusion SPECT image
Prior to tracer administration, subjects were advised to close their eyes and relax in order to avoid visual activation, but not to sleep. They received 1110 megabecquerel (MBq) of 99mTc-ethyl cysteinate dimer (ECD) intravenously in the supine position with their eyes open in a low-stimulation environment. The subjects' heads were strapped down to restrain head movement. An individual brain SPECT was performed 5 minutes later using a triple-headed gamma camera (MS3, Siemens, USA) equipped with a fanbeam collimator. A 128 × 128-pixel acquisition matrix was used with a 6° angular increment for 20 minutes. Images were reconstructed by a filtered back-projection method using a Butterworth filter (cut-off frequency: 0.35 cycle/pixel).
Acupuncture and postacupuncture image acquisition
The interval between the baseline and the second brain perfusion SPECT was 7 days. Two (2) acupoints (LI-4 and LI-11) in the right upper extremity were chosen for stimulation. The acupuncture needling was performed by a skilled Oriental doctor under aseptic conditions using stainless steel acupuncture needles (DongBang Acupunture, Inc., Korea) measuring 0.25 mm in diameter and 40 mm in length. The insertion depth of the needle into both acupoints was superficial (about 4–5 mm). The needle stimulation was gentle such that subjects could only feel a tingling sensation, but not the de qi sensation, when the needles were inserted. After insertion, the needles were retained with no stimulation for 15 minutes. For acquisition of the second SPECT, 99mTc-ECD was administered intravenously 15 minutes after completion of the acupuncture.
Data Analysis
Brain SPECT images were spatially normalized to a standard template provided by statistical parametric mapping 2 (SPM2) (Institute of Neurology, University of London, London, UK) in MATLAB software version 6.5 (Mathworks Inc., Natick, MA). A local optimization of the 12 parameters of an affine transformation was applied to the spatial normalization. The images were then smoothed with a gaussian kernel (full width at half maximum, 16 mm) to minimize noise and improve between-subject spatial alignment. To identify the brain regions in which perfusion had changed after SA, baseline and follow-up images were compared voxel by voxel (two-tailed paired t-test). Then, to compare the changes of rCBF after SA at LI-4 and LI-11 with those after EA at the same acupoints, 12 a two-sample t-test comparing poststimulation images for SA and EA was performed. An uncorrected p-value of <0.005 or a false discovery rate [FDR] corrected p-value of <0.05 with an extended threshold (Ke) >100 was considered to be significant. Anatomical labeling of significant clusters was performed using the automated anatomical labeling SPM toolbox, which was based on the anatomy provided by the Montreal Neurological Institute.
Results
None of the subjects complained of any side-effects caused by acupuncture that could have affected brain activity during the study.
Cerebral blood perfusion significantly increased after SA at LI-4 and LI-11 in the left superior frontal gyrus, left middle cingulum, left insular, right medial orbitofrontal gyrus, and right middle cingulum (two-tailed paired t test, p uncorrected <0.005, n = 10; Table 1, Fig. 1). However, none of the regions showed a significant decrease in cerebral blood perfusion after SA.
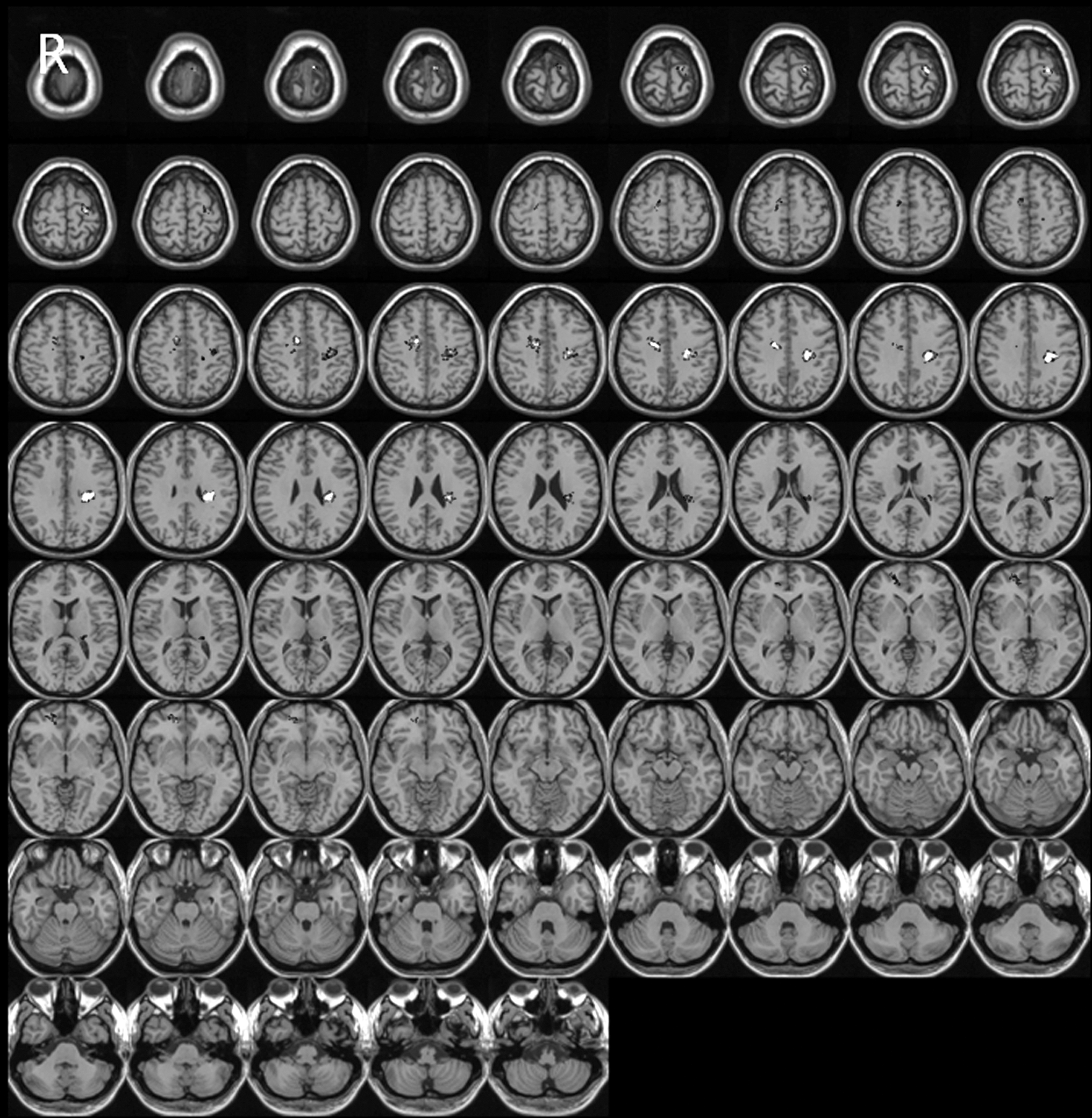
Brain areas showing significant changes in perfusion after superficial acupuncture at LI-4 and LI-11 (two-tailed paired t test, p uncorrected <0.005, n = 10). Regions of increased perfusion are indicated by white or gray spots on the transaxial images. R, right.
MNI, Montreal Neurological Institute, Montreal, Quebec, Canada.
A comparison of poststimulation images for SA and EA demonstrated that perfusion in the right lingual, both thalami, left middle temporal gyrus, left insula, and both hemispheres of the cerebellum had significantly increased after SA as compared with after EA (two-sample t test, p FDR-corrected <0.05; Table 2, Fig. 2), although a comparison of pre-acupuncture images between the SA and EA groups indicated that there were no significant differences (data not shown).
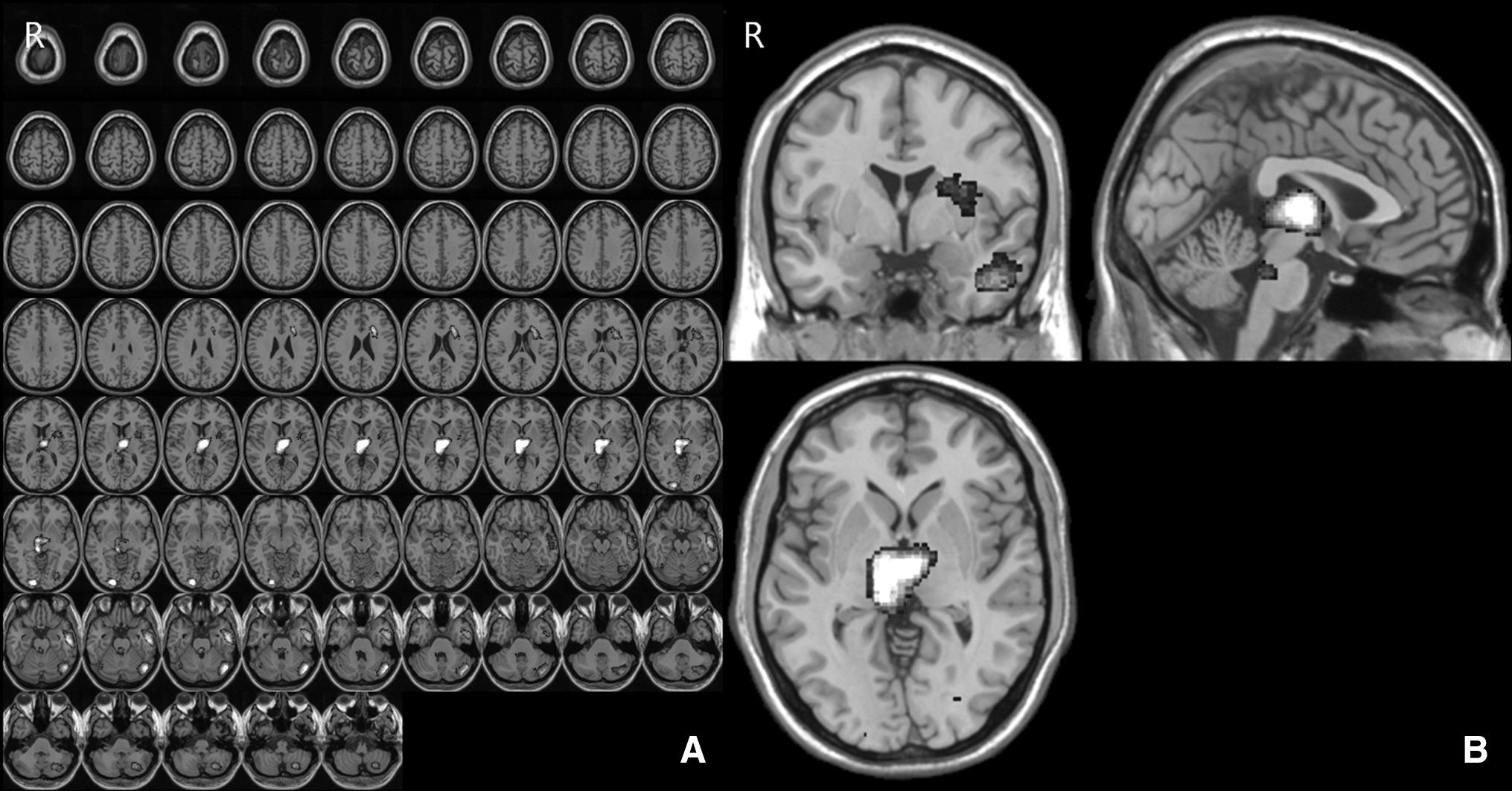
Brain areas showing significantly increased perfusion in superficial acupuncture at LI-4 and LI-11 compared with electroacupuncture at LI-4 and LI-11 (two-sample t test, PFDR-corrected <0.05). Regions of increased perfusion are indicated by white or gray spots on the transaxial images
MNI, Montreal Neurological Institute, Montreal, Quebec, Canada; FDR, false discovery rate.
Discussion
In this study, cerebral blood perfusion significantly increased in the left superior frontal gyrus, left middle cingulum, left insula, right medial orbitofrontal gyrus, and right middle cingulum after SA at LI-4 and LI-11. Our previous study demonstrated that EA administered at the same acupoints significantly increased rCBF in the left middle frontal, left superior parietal, right superior frontal, and right middle parietal gyri. 12 Although the acupuncture methods were different for both studies, the results indicated that LI-4 and LI-11 acupuncture induced a significant increase in rCBF in the frontal lobes regardless of whether SA or EA was used.
These results are much different from those of a previous control study, which reported that transcutaneous electrical nerve stimulation at right LI-4 and LI-11 increased rCBF only in the left somatosensory association cortex. 15 In addition, it was reported that EA administered at right GB-34 and GB-39, a pair of acupoints on the legs, increased rCBF in the right ventral posterior cingulate and left superior temporal, anterior transverse temporal, left parastriate, peristriate, right occipitotemporal, angular, left rostral postcentral, caudal postcentral, and preparietal gyri, 16 which differed from the results of SA and EA on LI-4 and LI-11. The current study and the abovementioned previous studies suggest that acupuncture-induced increases in rCBF may be acupoint-specific and dependent on stimulation methods, with or without penetration.
Previous studies have shown that ipsilateral cerebral regions may be affected by acupuncture. 10,12,17 In this study, both contralateral and ipsilateral cerebral regions showed significant hyperperfusion after SA, which is consistent with the results of the previous study that used EA. 12 These results suggest that both brain hemispheres were influenced by one-sided acupuncture stimulation, regardless of the type of acupuncture method used (SA or EA). It has been previously reported that activity in the ipsilateral hemisphere induced by acupuncture may be modulated through a crossed spino-thalamo-cortico-limbic pathway through the corpus callosum. 18,19 This mechanism may be supported by the hyperperfusion found in both cingula, beside the corpus callosum, after SA.
In the current study, none of the regions showed a significant decrease in rCBF after SA, while the previous study demonstrated that there were specific regions with decreased perfusion after EA. 12 The comparison of poststimulation images for both the SA and EA groups also showed that there were specific areas showing a significant increase in perfusion after SA as compared with EA. These results seem mainly to be attributed to the differences in decreased perfusion between SA and EA that were found in the paired t tests. Although the clinical meaning of decreased perfusion is uncertain, there has been an explanation referred to as “coordination and redistribution.” 20 According to this explanation, EA may redistribute CBF from areas with decreased perfusion to those with increased perfusion. In contrast, the absence of a decrease in perfusion after SA causes little or no redistribution of CBF, which may be interpreted as implying that SA provides relatively less strong stimulation than EA. This is in accord with the empirical perception that EA provides stronger stimulation than SA, which is partly supported by previous reports that EA produced more widespread fMRI signal increase than manual acupuncture did. 21,22 In the clinical respect, the difference in stimulation intensity between EA and SA may result in a discrepancy between therapeutic effects, as different acupuncture methods have been reported to cause different clinical outcomes. 6,7 Therefore, further study is warranted to clarify whether these results from healthy subjects produce different clinical outcomes for EA and SA.
Our study had a few limitations. Theoretically, it would seem appropriate to compare the effects of SA and EA in the same group. Practically, however, it is almost impossible to do this in SPECT studies because of an ethical issue, as testing would involve the repeated use of radiopharmaceuticals. Therefore, in the current study, we compared the effects of SA with those of EA as previously reported, on the basis of the following grounds: first, the ages of the volunteers in both groups were similar and the conditions of the SPECT image acquisition from both groups were identical (having been performed at the same place with the same SPECT machine, although the times of the subjects' enrollment were different); second, a comparison of pre-acupuncture images for the SA and EA groups indicated that there were no significant differences.
In conclusion, we observed that the specific increase patterns of rCBF after SA at LI-4 and LI-11 were similar to those after EA. However, there was a significant difference between the decrease patterns of rCBF after SA and EA, which may be due to the difference in the strength of acupuncture stimulation between the two methods. Further studies will aid in using these findings to select the appropriate stimulation method in acupuncture therapy.
Footnotes
Acknowledgments
This research was supported by the Program of Kyung Hee University for Young Researchers in Medical Science [KHU-20071476]
Disclosure Statement
No competing financial interests exist.