
Abstract
Background:
The action of homeopathic medicines, in ultra-high dilution, is not directly observable. An attempt was made to explore autonomic response of selective homeopathic medicines, in healthy persons, using Medical Analyzer System (Electronics Division, Bhabha Atomic Research Centre, Mumbai, India).
Objective:
The objective of the study was to observe the action of homeopathic medicines on physiologic variability of heart rate and blood flow.
Material and methods:
Pre- and postinterventional variability spectra of heart rate and blood flow of 77 subjects were recorded with the Medical Analyzer System, administering homeopathic preparations of Aconitum napellus (6c, 10M), Arsenicum album (200c, 1M), Gelsemium sempervirens (200c, 1M), Phosphorus (200c, 1M), Pulsatilla nigricans (200c) and Sulphur (200c, 1M) versus placebo control. The amplitude of the peaks viz. low-frequency, medium-frequency, and high-frequency was measured for postintervention analysis. An increase in the amplitude of any valid peak by 100% or a decrease by 50% was considered as significant change.
Results:
Aconitum napellus produced a response in heart rate variability (HRV) with 30c potency and in blood flow variability with 1M potency. Sulphur 200c and 1M, Gelsemium 200c and Pulsatilla 200c, produced a 62.5% response in HRV against the placebo response of 16.6%. Gelsemium, Phosphorus, and Sulphur produced a response in blood flow variability with a 1M potency, similar to the response of Aconitum napellus 1M.
Conclusions:
These data suggest that it is possible to record the response of homeopathic medicines on physiologic parameters of the autonomic nervous system.
Introduction
A new technique, physiologic variability analysis, can study the functioning of the autonomic nervous system (ANS) through variations in a physiologic parameter in a subject resting in the supine position to estimate the input contribution of different body systems to ANS. 7 Several other studies have indicated that diseases of different organs of the body such as diabetes mellitus, myocardial infarction, hyperthyroidism, tuberculosis, and autoimmune deficiency syndrome cause specific alterations in physiologic parameters' variability. 8 –11 Jindal et al. measured central and peripheral blood flow using impedance plethysmography (IPG), before and after the administration of homeopathic medicines to patients. They recorded increase in blood flow with Sepia officinalis CM and Sulphur 1M. 12 As a natural extension of these observations, Jindal et al. had recorded heart rate variability (HRV) and blood flow variability (BFV) after administration of Sulphur 1M, Gelsemium 10M, and Phosphorus 30c and observed unique changes. 13
The Central Council for Research in Homoeopathy, India, took the initiative to extend these studies with a predefined protocol and meticulous methodology at the Regional Research Institute of Homoeopathy, Mumbai. The present article describes the effect of homeopathic potencies of Aconitum napellus, Arsenicum album, Gelsemium sempervirens, Phosphorus, Pulsatilla nigricans, and Sulphur on HRV and BFV.
Objective
The objective of this investigation was to observe the changes produced in the variability spectrum of HRV and BFV following administration of placebo and different potencies of certain homeopathic medicines.
Materials and Methods
The study group comprised 77 healthy volunteers ages 18–35 years. Laboratory investigations such as complete blood count, erythrocyte sedimentation rate, liver function tests, renal function tests, blood glucose level, serum lipid profile, electrocardiogram, and chest radiograph were done for all the subjects whose written consent was obtained after explaining the details of the study.
Medical Analyzer System (Electronics Division, Bhabha Atomic Research Centre, Mumbai, India) records the variability spectrum of heart rate and peripheral blood flow. This system is based on the principle of IPG and records blood volume changes in any part of the body noninvasively by measuring its electrical impedance, which is inversely proportional to blood volume changes. The rate of change of impedance thus gives the rate of change of blood volume. The pulsatile blood flow during ventricular systole is reflected as well-formed peaks in IPG, and the instantaneous heart rate is derived from the time elapsed between two consecutive peaks. The blood flow index (blood flow in milliliters per 1000 cm3 of body tissue per cardiac cycle) is obtained from the amplitude of the peak and gross electrical impedance of the body segment. 10 A 5-minute record of instantaneous heart rate and blood flow values thus obtained is interpolated to obtain periodic values of these parameters as a prerequisite before Fourier transformation. The subsequent Fourier transform depicts the contribution of various rhythms that cause variability in the physiologic parameters and represented by low-frequency (L), medium-frequency (M), and high-frequency (H) peaks (Fig. 1). “L” generally denotes sympathetic action, whereas “M” and “H” denote parasympathetic and/or vagal action. In view of the multiple readings required in this protocol, the system software was upgraded to incorporate the average variability spectrum, for HRV and BFV obtained from multiple readings in situ, pre- and postintervention, and display these on a PC monitor. 14

Heart rate variability (HRV) spectrum in a control subject. The lower graph shows HRV in the time domain and the upper one shows the same in the frequency domain. The complex time domain variations lead to definite peaks in the frequency domain. The peaks, their amplitudes, and power are given in the table at the bottom of the figure.
Medicines coming in the top grade on repertory search related to cardiorespiratory functions such as variations in pulse, respiration, breathing, and so on were considered for deciding on trial drugs. For rubric selection, “Complete Repertory” by Roger van Zandvoort 15 was consulted. In such a group, both polychrests as well as remedies having specific action on these parameters were included. As placebo, plain globules soaked with dispensing alcohol were used. Since it was an exploratory study, two different protocols were followed for the experiments.
Protocol 1 was designed for the Aconitum napellus group of 27 subjects. On the first day, pre- and postintervention data for placebo were obtained. Placebo was replaced by Aconite 6c, Aconite 30c, Aconite 200c, Aconite 1M, and Aconite 10M on the 2nd, 3rd, 4th, 5th, and 6th days, respectively. Data analysis was done for each of the days.
Protocol 2 was designed for a group of 50 subjects and comprised Arsenic 200c (n=5), Arsenic 1M (n=5), Gelsemium 200c (n=5), Gelsemium 1M (n=5), Phosphorus 200c (n=5), Phosphorus 1M (n=6), Pulsatilla 200c (n=4), Sulphur 200c (n=10), and Sulphur 1M (n=5). In this case, pre- and postintervention data were recorded with placebo on the 1st day and with any one of the selected medicines and potency on the 2nd day.
Since the study has been exploratory in nature, it was the intention of the authors to investigate all possibilities under this study. Protocol 1 was designed to meticulously investigate the effect of a particular medicine in different potencies. Protocol 2 was designed in such a manner that a large number of medicines could quickly be screened for their action on variability spectrum.
Data for both of the protocols were collected as follows. With the subject in the supine position, the IPG signal was recorded from the wrist of the subject for 5 minutes and three such consecutive observations were taken. The subject was then administered the desired substance (placebo or medicine) followed by recording of three similar readings again to obtain the postintervention data of HRV and BFV. The pre- and postintervention data were then analyzed using the software described above, which gave out average spectra of multiple readings.
In the postintervention analysis, a change was considered significant if the amplitude of any valid peak either increased by 100% (designated as “+”) or decreased by 50% (designated as “-”) as compared to the pre-intervention amplitude. These high thresholds were intentionally fixed in order to have reliable findings. Amplitude of the peak had been chosen for postintervention analysis in place of area under the same because the former had the advantage of noise elimination. A postintervention decrease in the first peak (L-) and increase in the third peak (H+) were discarded because these changes commonly occur due to prolonged rest.
Results
Typical pre- and postintervention average variability spectra are depicted in Figures 2 and 3. As can be seen from Figure 2, the placebo has not elicited any response in either spectra (HRV or BFV). The medicine has produced change in both HRV and BFV as illustrated in Figure 3.
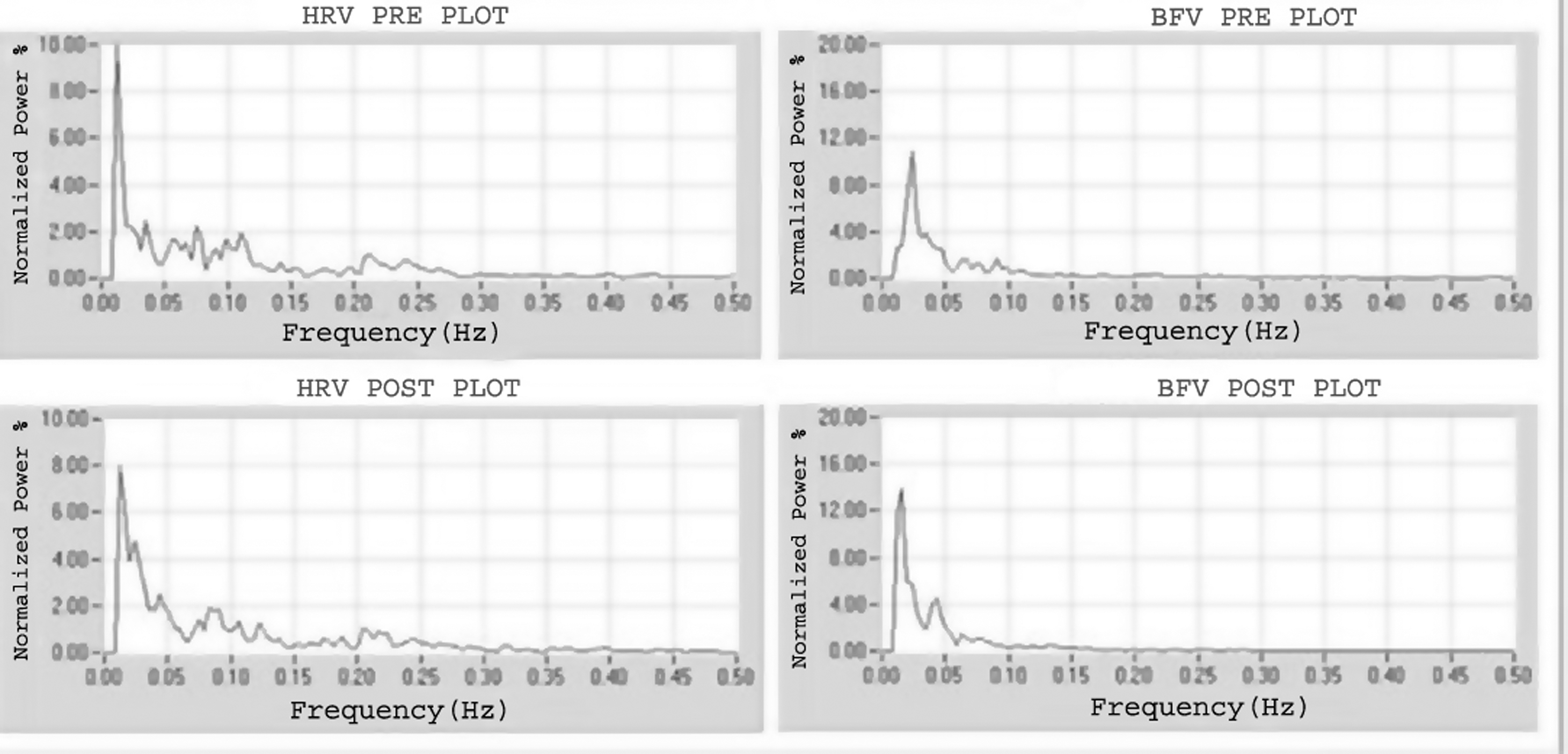
Pre- and postplacebo heart rate variability (HRV) and blood flow variability (BFV) average spectrum. The graphs on the top give HRV and BFV before and the ones in the bottom give HRV and BFV after placebo. There was a 20% decrease in the first peak in the HRV spectrum, which is not significant. Similarly, there is a 25% increase in the first peak in the BFV spectrum, which is also not significant as per the criteria.
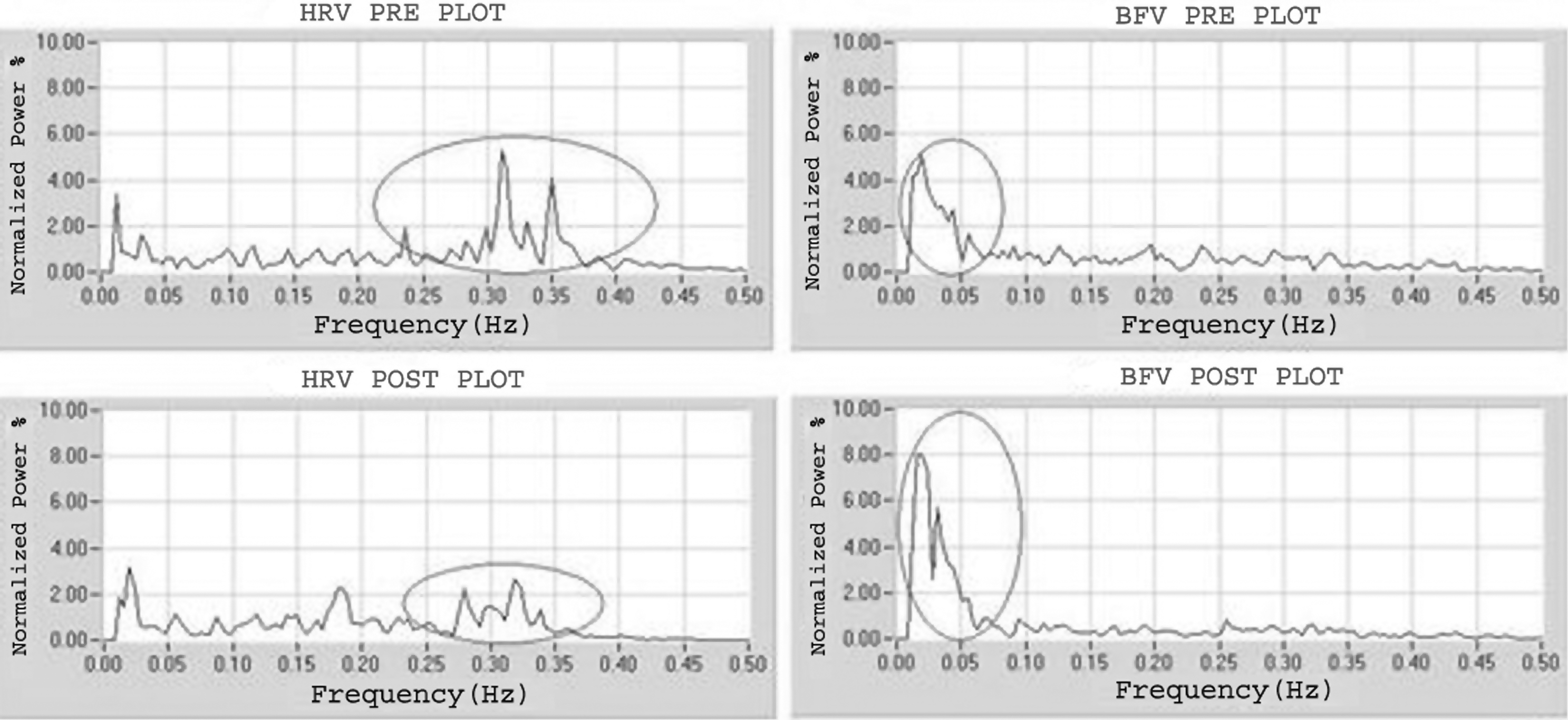
Pre- and postintervention average spectrum of heart rate variability (HRV) and blood flow variability (BFV) after Sulphur 1M. In HRV, the third peak is decreased in amplitude to almost half, whereas in BFV the first peak amplitude has nearly doubled.
Table 1 summarizes the results of intervention in HRV. Under Protocol 1, Aconite 30c has shown response in HRV. From Protocol 2, it is seen that the maximum response has been obtained in 200c potency, namely, Gelsemium 200c, Pulsatilla 200c, and Sulphur 200c accounting for 68.42%. The exception in this group is Sulphur 1M, which has shown some response in HRV and together, they account for 62.5% response in HRV as against 16.6% of placebo response.
Table 2 summarizes the response in BFV. From Protocol 1, Aconite 1M has shown response in BFV in 53.9% of the study sample as against placebo response of 25.92%. From Protocol 2, Gelsemium 1M, Phosphorus 1M, and Sulphur 1M have shown response in BFV, the exception here being Phosphorus 200c, which has shown a similar response. Response produced by medicines is 40% as against placebo response of 0%.
Other potencies of Aconite from Protocol 1 and both potencies of Arsenic in Protocol 2 have not shown any response either in HRV or in BFV.
Discussion
This exploratory study on HRV and BFV with homeopathic medicines on a defined protocol was the first of its kind using average spectra of multiple readings. The results show that certain medicines and potencies have action on either HRV or BFV (Tables 1 and 2).
Though the study was on an elaborate scale with defined protocol and multiple readings per setting, it was still exploratory in nature and, therefore, the study protocol and interpretation of results were not strictly in conformity with conventional pharmacologic trials of modern medicine. Some deviations were made in the analysis of variability data. Hitherto, the variability spectrum was analyzed on the basis of area under different peaks, which represents the contribution of a particular rhythm in autonomic control. Though this approach has the simplicity of machine-generated results, it completely overlooks the amplitude of a particular peak, which signifies the coordination of a particular rhythm in autonomic control. For instance, a narrow peak with high amplitude may have the same area as that of a very broad peak with very low amplitude; in reality, the narrow peak with high amplitude represents better coordination in the ANS. This has led to using the amplitude of the peak in variability spectrum to differentiate the response. Furthermore, the spectrum was analyzed between 0.02 Hz and 0.50 Hz as compared to the 0.00–0.50 Hz conventionally used. This was because the zero frequency component of variability sometimes suppresses the higher frequency components and can lead to incorrect inference. Since our interest was to study the various rhythms controlling ANS and not the zero frequency component, the deviation was justified.
In conducting the experiments, even though a separate placebo group has not been tested, placebo was administered on the first day of the experiment and medicinal intervention on following day(s) in all the subjects, irrespective of the group or medicine they belong to. This was done so that subjects act as their own control because physiologic response of every individual is different even in similar circumstances. To keep the variables at minimum, in all the subjects the experiments were conducted under similar conditions, and for each individual, the same timing was maintained throughout the experiment.
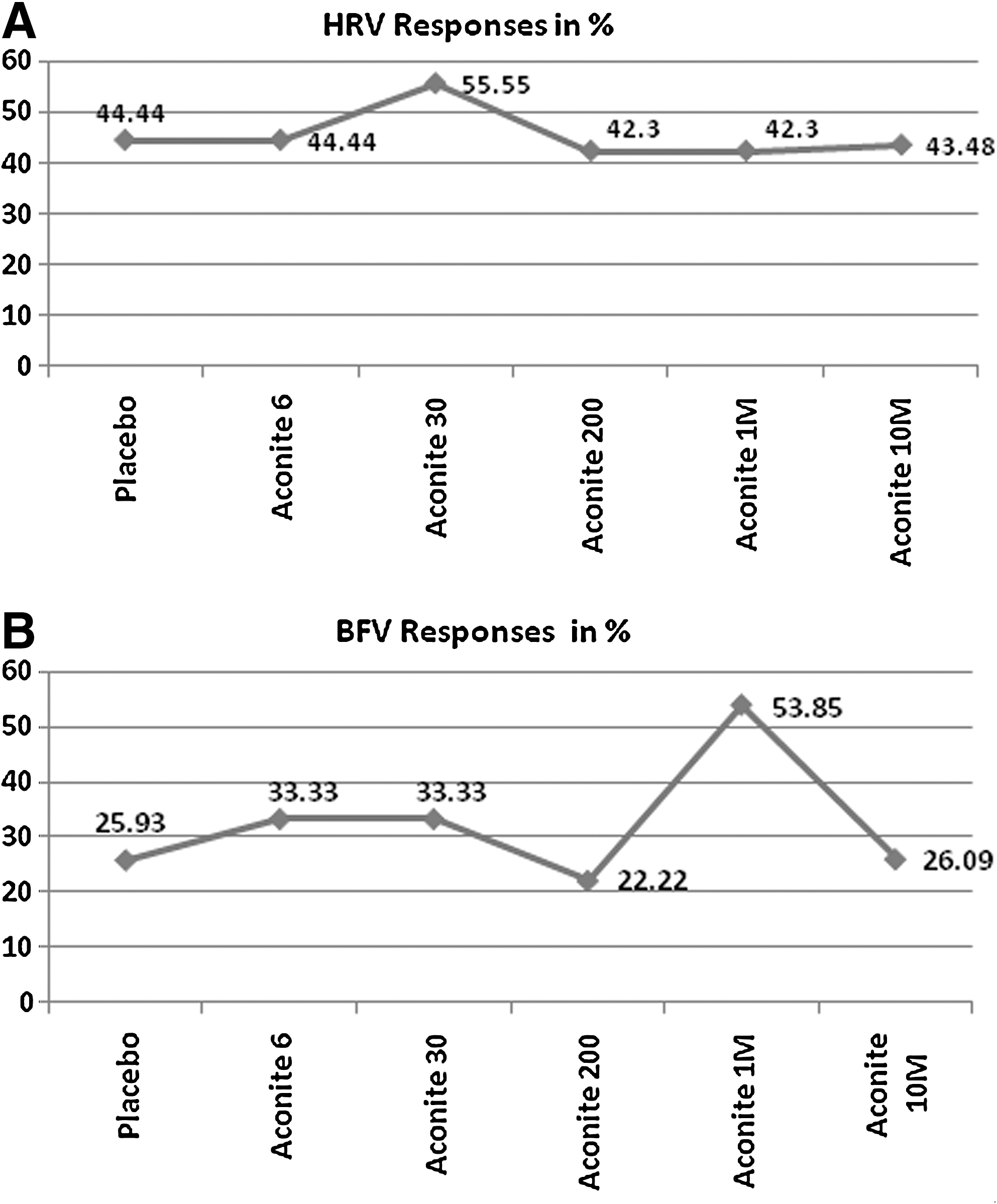
The experiment began with the Aconite group, as per Protocol 1, and various potencies were used in ascending order in each of the individuals. The observed outcome was potency specific. Aconite 30c produced a peak in HRV (Fig. 4A) and Aconite 1M produced a similar peak in BFV (Fig. 4B). It shows that Aconite acts at one level in 30c potency and another level in 1M potency. Other potencies did not show any remarkable changes either in HRV or BFV.
The results in the second group of subjects under Protocol 2 also revealed similar observations. Gelsemium 200c, Pulsatilla 200c, Sulphur 200c, and Sulphur 1M (1M potency is an exception here) produced response peaks in HRV (Table 1) and Gelsemium 1M, Phosphorus 1M, Sulphur 1M, and Phosphorus 200c (200c potency is an exception in this group), produced response peaks in BFV (Table 2). Arsenic did not produce any response in either of the potencies. The observations were consistent with those of Aconite: lower potency produced a response in HRV and higher potency produced a response in BFV, with the exception of Sulphur 1M in HRV and Phosphorus 200c in BFV.
A pattern seems to emerge from these experiments: medium potencies such as 30c and 200c have probable action on HRV and higher potency such as 1M has probable action on BFV. It is noteworthy that HRV and BFV are derived from the same data, yet the changes produced in both are by different potencies of the same medicine. To illustrate, the change in HRV at Aconite 30c is not reflected in BFV, and change in BFV at Aconite 1M is not reflected in HRV. This may be indicative of the selective action of different potencies of the same medicine. Plotting of the same shows a peak in HRV response, with Aconite 30c (Fig. 4A) and a peak in BFV response with Aconite 1M (Fig. 4B). These peaks separate the response of Aconite 30 and 1M from the rest of the interventions in this group.
The response has been counted positive, irrespective of its nature. For instance, significant increase or decrease in either of the L, M, or H peaks has been counted as response. In future such studies, the authors may explore the possibility of analyzing response with respect to a particular peak or parameter.
This was an exploratory study on variability in physiologic parameters, conducted for the first time on this subject hitherto unexplored in a systematic manner with homeopathic medicines. Eliciting an autonomic tone of healthy subjects with the help of homeopathic medicine is a process similar to that of a “homeopathic pathogenetic trial” in which, when a medicinal substance is given to a group of healthy provers, some symptoms of the medicine are elicited in a number of proving subjects, yet there are few symptoms that appear in 1 or 2 subjects only. Some subjects do not prove any of the symptoms of a medicine. This perhaps explains why some of the medicines/potencies did not show any response.
A few observations emerge from the experiments. First, the autonomic nervous system is not under voluntary control, and recording signals from the ANS immediately after intervention (within 5–15 minutes of intervention) helped eliminate subjective bias and objectively demonstrated the action of the homeopathic medicines.
Second, responses were observed in 30c, 200c, and 1M potencies, which are well beyond Avogadro's number. These are observations from exploratory experiments in emerging areas of physiologic variability and need validation by repeated experiments of this type. Detection of response was the primary objective of this study, which has been achieved. The number of subjects in each group was small; hence it was not possible to show the statistical significance of the results, an aspect that is intended to be covered in future studies.
Conclusions
Selective response has been detected with the administration of different potencies of various homeopathic medicines in HRV and BFV, and the exploratory study has provided directions for future trials. Reproducibility of these observations in a larger sample size will be necessary for validation of this study's results.
Footnotes
Acknowledgments
The authors are grateful to Dr. G.D. Jindal, Electronics Division, Bhabha Atomic Research Centre, Mumbai for providing the expertise needed for the study. They thank all of the students, interns, and faculty members of CMP Homoeopathic Medical College, Mumbai for enthusiastic participation in the study as volunteers. The authors acknowledge the contributions of Mrs. Uma A. Clerk and other staff of the Regional Research Institute for Homoeopathy, Mumbai.
Disclosure Statement
No competing financial interests exist.