
Abstract
Objectives:
The study objectives were to evaluate outcomes in patients who have received dry needling treatments and to identify predictors of pain and disability.
Design:
The study was a prospective cohort follow-up design.
Setting:
The study was conducted at the Pain Clinic at Pingtung Christian Hospital, Taiwan.
Subjects:
Ninety-two (92) patients sick-listed for 3 months or longer for myofascial pain syndrome.
Interventions:
From February to October 2008, participants were treated at the pain clinic with dry needling of trigger points and muscle stretches of the involved muscles.
Outcome measures:
Data were collected by self-administered questionnaires to assess changes in pain intensity and pain interference. Data collection was performed at baseline and after 2, 4, and 8 weeks. Sociodemographic variables, symptom characteristics, and baseline outcome measures were analyzed using generalized estimating equation methodology.
Results:
The proposed dry-needling protocol reduced pain intensity and pain interference. Long duration of pain symptoms, high pain intensity, poor quality of sleep, and repetitive stress were associated with poor outcomes.
Conclusions:
Dry needling is an effective treatment for reducing pain and pain interference. However, long pain duration, high pain intensity, poor quality of sleep, and repetitive stress are associated with poor outcomes. Treatment outcome depends not only on the dry needling protocol, but also on disease characteristics and patient demographic profile.
Introduction
The many factors associated with the persistence of MTrP pain include occupational activity, postural abnormalities, mechanical disorders, metabolic abnormalities, and psychosocial factors. 3,8 Potential predictors of MPS revealed by studies of musculoskeletal pain include the severity and duration of the complaint and environmental factors such as working status. 9 –11 Most studies of MPS have focused on the prognostic value of clinical symptoms such as duration and intensity of pain. Despite convincing evidence of the prognostic value of lifestyle factors, 12,13 no studies have demonstrated that lifestyle factors are related to chronic pain in MPS.
Determining the prognostic value of clinical, psychosocial, occupational, and treatment factors in patients with MPS can improve accuracy in predicting their symptoms. The study aims were to follow up patients who had received dry needling treatment and to identify risk factors for persistent MPS symptoms in patients treated with dry needling of trigger points and passive stretching of affected muscles.
Materials and Methods
Design
This observational prospective cohort study was performed in the city of Pingtung, Taiwan. The subjects included all patients with MPS who had been referred for evaluation and treatment to the Pingtung Christian Hospital (PTCH) pain clinic from February to October 2008. Inclusion criteria were chronic musculoskeletal pain for 3 months or longer due to nonspecific muscle pain, physical examination revealing tender spot in a palpable taut band, ability of patient to distinguish between varying intensity of pain, referred pain pattern and local twitch response, 14 Chinese speaking, and age at least 18 years. Exclusion criteria were fibromyalgia syndrome; neurological pain; infection; drug or alcohol abuse; rheumatologic disease; pregnancy; and any other disease that might interfere with participation. The research protocol was reviewed and approved by the institutional review boards of PTCH. Signed, informed consent was obtained from all subjects.
Interventions
All needling protocols were performed by a single specialist. Taut bands with trigger points were isolated by palpation to ensure reproducibility of symptoms. Therapeutic needling was then performed with sterile 32G-diameter, 80-mm acupuncture needles. A needle plunger was first used to pierce the skin and muscle with the acupuncture needle. After the needle penetrated the skin, the plunger was removed, and the needle was inserted further into the taut band to elicit a twitch response. Appropriate placement of the needle was confirmed by reproduction of recognizable pain or by observation of local twitch response. The needle was then partially withdrawn and repeatedly inserted into the muscle until no further twitches were observed. After inactivating trigger points and reducing referred pain, the specialist then passively stretched the involved muscle toward its normal length. The patients then performed the muscle-stretch exercise technique developed by Travell and Simons. 3,15 All subjects received eight needling protocols administered over an 8-week period.
Outcome assessment
Pain questionnaire
After the dry needling protocol, each subject completed a questionnaire regarding demographic information (including education and marital status), history of pain and previous pain interventions, history of systemic disease, individual lifestyle, and occupational background.
The questions about individual lifestyle assessed factors such as smoking, drinking, sleep deprivation, and nutritional inadequacies. The questionnaire assessed whether the subjects had smoked 100 or more cigarettes in their lifetimes, whether they currently smoked cigarettes every day or some days, whether they consumed 10–45 g of alcohol per day, whether they subjectively needed sleep 1 hour more than actual sleep time, 16 and whether they had ever been diagnosed with a vitamin or iron deficiency.
The participants were also asked about occupational background. To assess repetitive work history, the questionnaire asked if they currently spent 10–44 minutes per hour performing repetitive movements in a typical work hour. The subjects were asked if they had ever worked in a cold working environment, which was defined as a workplace temperature below 20°C. Prolonged postures were defined as sitting for at least 30 minutes per hour, standing for at least 30 minutes per hour, or squatting for at least 5 minutes per hour.
The Taiwan version of the Brief Pain Inventory (BPI-T) was used. 17 The BPI has been widely used in the United States and has been validated in several languages. The BPI-T developed from the original BPI measures intensity of pain (sensory dimension) and interference of pain in daily life (reactive dimension) on a simple numeric scale from 0 to 10. Pain intensity was assessed by a four-item self-reported inventory requiring patients to rate their pain at the time of completing the questionnaire (present pain) and also when it was “worst,” “least,” and “average” within the previous week. Pain severity was measured on a scale from 0 (“no pain”) to 10 (“extreme pain”). A similar seven-item self-reported inventory was used to measure interference of pain with daily life, including general activity, mood, walking ability, normal work, relationships with others, sleep, and enjoyment of life. The anchor points for each of the interference scale items were “0” (“no interference”) and “10” (“extreme interference”). In addition to reporting present pain intensity, patients were instructed to indicate any changes in the type of pain and any use of nonpharmacologic pain treatment. The coefficient α regarding internal reliability was 0.81 for the severity scale and 0.89 for the interference scale.
All data collection was performed by 2 trained research assistants. Baseline data collection was as follows: Pain questionnaire and BPI-T (both at pain clinic); follow-up BPI-T by telephone interview 2 weeks, 4 weeks, and 8 weeks later.
Statistical analysis
Demographic and clinical characteristics were analyzed by using descriptive statistics. For two time interval comparisons, Effect Size (ES) was used to standardize the extent of change measured by the BPI-T. The ES is the difference between the mean scores for two time intervals divided by the standard deviation (SD) in the previous (or formal) time-interval score. An ES of 1.0 is equivalent to a change of 1 SD in the sample. ESs of 0.2, 0.5, and 0.8 are generally interpreted as small, medium, and large changes, respectively. 18
Multiple time points (in weeks) of follow-up was introduced into the generalized estimating equations (GEE) model with four domains of BPI-T (i.e., intensity of worst, average, and present pain and aggregated pain interference) used as the outcome variables to determine average score improvements.
Univariate models were then used to assess effective predictors of change in four domains of the BPI-T at different time points when using the baseline pretreatment measures. These effective predictive variables were included as covariates in the GEE approach because they were statistically significant in the multivariate models. 19 The SPSS 15.0 software for Windows and Stata Statistical Package, Version 9.0 (Stata Corp., College Station, TX) were used for all statistical analyses, and a p-value < 0.05 was considered statistically significant.
Results
Figure 1 shows that, after excluding patients with fibromyalgia (n=1), neurological pain (n=1), and hearing impairment (n=1), 105 subjects were eligible for the study. Of the 102 eligible subjects who gave written consent and were enrolled in the study at baseline, 8 were excluded because they could not be contacted, and 2 were excluded due to dissatisfaction with dry needling treatment. The remaining 92 subjects with MPS completed pretreatment and post-treatment assessments.
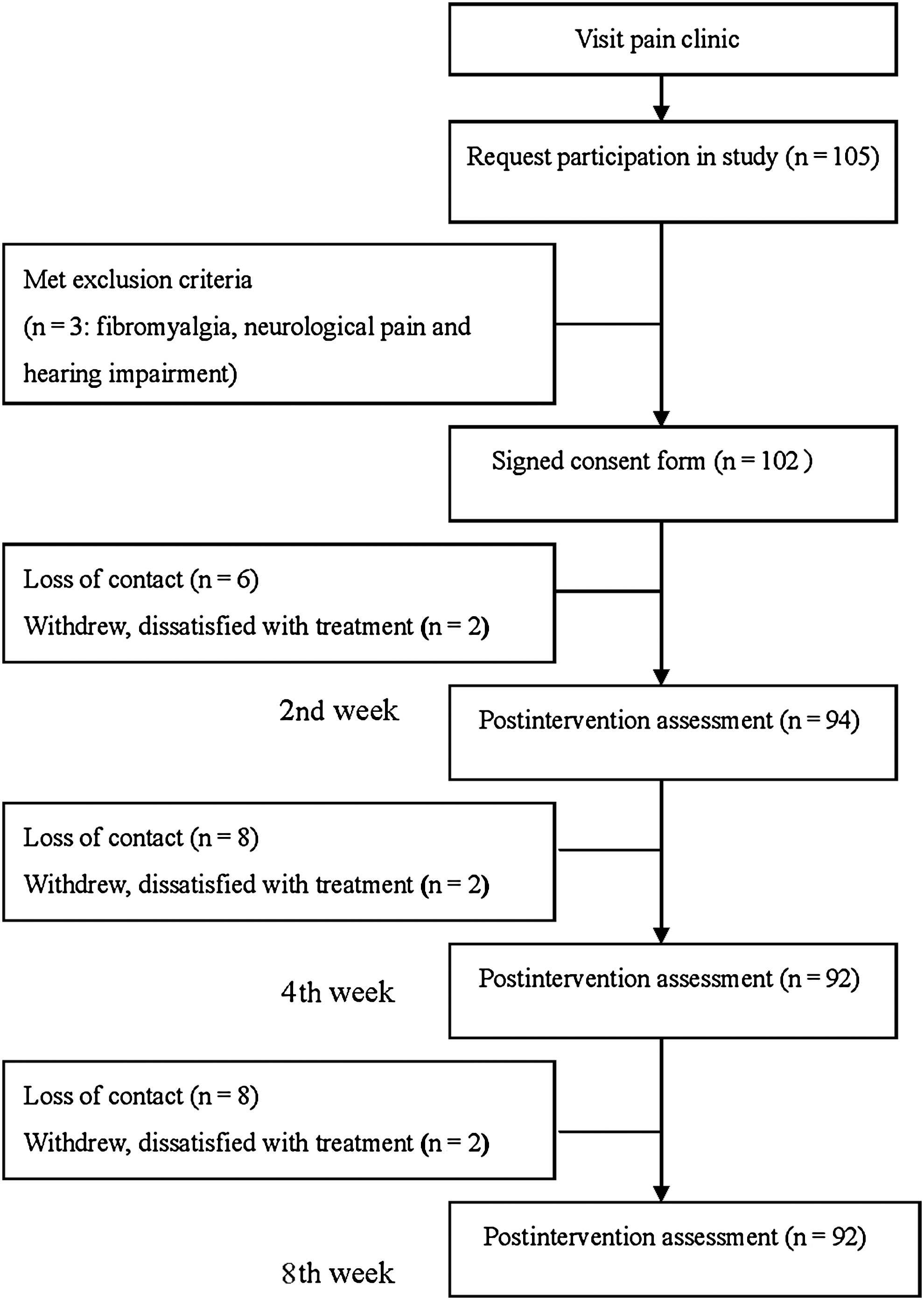
Progression of participants through the trial, including those who met exclusion criteria, those who withdrew, and those who were lost to follow-up.
Table 1 details the demographic data for the patients with MPS. The population had a mean age of 50.2 years (SD 13.9). Mean pain duration was 44.7 months (SD 59.6), and 70.7% of the patients were female. The anatomic site of the pain was diverse and classified into five clusters: head-neck, back-gluteus, upper limb, low limb, and shoulder-girdle. The 2 groups of included and excluded patients did not significantly differ in baseline patient characteristics (data not shown).
Low, middle, and high education refer to primary school education, high school, and university, respectively.
Table 2 also presents the baseline results for the GEE model of the BPI-T scores. Pain intensity and pain interference were assessed at baseline and then 2, 4, and 8 weeks later. A notable finding for BPI-T after dry needling and the intervention period was a significant negative change in pain intensity, including worst, average, and present pain at the 2-week time point (p<0.001). Worst pain and average pain had a larger ES (−0.67 and −0.68, respectively) at the 2-week time point. In the 8th week, the reduction slopes for aggregated pain interference significantly differed from those observed at the 2-week time point (p<0.001).
ES1 2nd week versus pretreatment; ES2 4th week versus 2nd week; ES3 8th week versus 4th week.
Aggregated pain interference was calculated as follows: [(pain interference of general activity+mood+walking ability+normal work+relationship+sleep+enjoyment of life)/7].
SD, standard deviation.
Table 3 shows results for the univariate models for demographic associations with pre- and post-treatment BPI-T. In the dry-needling protocol cohorts, pain duration, sleep deprivation and nutritional inadequacies, occupational history of repetitive work, pretreatment BPI-T, and pain location including head–neck and shoulder-girdle were significantly related (p<0.05) to post-treatment BPI–T.
Gender: female versus male; Lifestyle factors: present versus absent; Occupational condition: present versus absent. Pain locations per patient: present versus absent.
Aggregated pain interference score was computed as follows: [(pain interference of general activity+mood+walking ability+normal work+relationship+sleep+enjoyment of life)/7].
Table 4 summarizes the results of all of relevant GEE analyses. The first model, which compared trends in BPI-T over time, indicated that BPI-T scores gradually decreased. In the cohort, the regression coefficient for three time points was significantly and negatively related to the sensory dimension of BPI-T. The regression coefficient for the 4-week and 8-week time points was significantly and negatively related to aggregate pain interference.
Present versus absent.
Aggregated pain interference score was computed as follows: [(pain interference of general activity+mood+walking ability+normal work+relationship+sleep+enjoyment of life)/7].
The second model, which described the relationships between demographics and their associations with time and BPI-T, revealed that pain duration was significantly and positively related to worst pain and aggregated pain interference. However, sleep deprivation was significantly and positively related to worst pain and average pain. Repetitive work was significantly and positively related to present pain. All observed associations with baseline demographics varied over time.
The third model described the longitudinal relationship between baseline and post-treatment BPI-T after adjusting for time, baseline demographics, and their interactions with time. In the cohort, baseline BPI-T was significantly and positively related to post-treatment BPI-T. Again, all associations with baseline demographics and BPI-T varied over time.
Discussion
This study is the first to examine the effects of dry needling in patients with MPS and the first to apply GEE methodology to analyze how covariates are related to outcomes in this patient group. A longitudinal data model was constructed for the GEE. The correlation structure between dry-needling responses was analyzed at four different time points. The primary aim of this study was to evaluate a dry-needling protocol for MPS. Comparative studies indicate that dry needling is as effective as injected anesthetics such as lidocaine. 5 Their comparable effectiveness in relieving overall pain supports the theory that mechanically disrupted muscle fibers and increased blood flow are important factors in pain relief. 20 Techniques for passively stretching muscles to their normal lengths can inactivate trigger points, reduce referred pain, and improve range of motion (ROM). 21 The efficacy of this treatment was reflected in the reductions in pain intensity (worst pain, average pain, and present pain) and aggregated pain interference observed in the patients with MPS in this study. Therefore, despite the current lack of objective data to confirm that dry needling improves muscle length or ROM, the significant subjective improvement observed in this study is very convincing. Although the pain relief achieved by dry needling is often discredited as a placebo effect, local muscle mechanisms may still contribute to global reduction in pain perception. The effects of such mechanisms may have key roles in achieving clinical improvements.
Pain severity impacts health-related quality of life (HRQoL). 22 Worst pain is a common clinical indicator of treatment outcome and is highly correlated with pain interference. 23 Pain interference and worst pain, which is usually fluctuating and brief, are very difficult to treat. 24 The GEE model of BPI-T scores in this study showed that worst pain was significantly improved at 2 and 8 weeks. Worst pain and average pain may have assimilative effects on HRQoL that parallel those produced by pain interference. Thus, improvements in worst pain and average pain may also improve pain interference and HRQoL. Although aggregated pain interference in the patients with MPS in this study also decreased over time, aggregated pain interference significantly differed between baseline and the 8th week. Worst pain and average pain at 2 and 8 weeks were also significantly improved in comparison with baseline. The slow improvement observed in aggregate pain interference suggests a maturation effect. 25
The second aim of the present study was to identify prognostic indicators after dry-needling protocol. Prospective cohort follow-up studies are essential for identifying prognostic predictors. Studies of prognostic indicators of musculoskeletal pain have focused on specific sites of regional pain (e.g., low back, neck, shoulder, and knee). 26 –28 Patients treated for musculoskeletal pain in pain clinics, however, often report pain at multiple sites. In this study, the objective was to identify potential prognostic indicators across different regional pain sites.
The results of the authors' analyses also showed the importance of symptom duration and severity in predicting outcome. A systematic review of prognostic indicators of musculoskeletal pain in primary care found that predictors of poor outcome across more than one anatomical site include disease characteristics (high intensity of pain, long duration of pain, widespread pain, previous episode of pain, and disability caused by pain), psychologic factors, limited social support, and older age. 29 Longer pain duration is also associated with poor prognosis for low-back pain and shoulder pain. 27,30 Two (2) studies have reported a negative association between high-intensity pain and outcomes at 1 year. 9,31 In agreement with previous studies, the most consistent predictor of poor outcome in the current study was duration of symptoms at baseline. In the present study, symptoms were more likely to persist in patients who already had a long history of pain symptoms at the time of presentation, and baseline BPI-T was significantly and positively related to post-treatment BPI-T. Variables associated with manual work such as heavy lifting, repetitive motion, or squatting for extended periods have revealed significant associations with several musculoskeletal pain conditions, including neck and shoulder pain. 11 The current study showed that repetitive work was significantly and positively related to present pain following dry-needling treatment.
Sleep deprivation does produce hyperalgesic changes in healthy subjects, 32 which likely reflect alterations in supraspinal modulation of nociception such as impaired function of inhibitory modulation pathways. Sleep deprivation has a much larger effect on muscle nociception than on skin nociception. 33 Furthermore, sleep deprivation is known to produce additional effects such as increased fatigue and negative mood, which might cause a modulation of pain processing. Depression, which is strongly associated with poor mental HRQoL, is only moderately associated with poor physical HRQoL. However, sleep problems are apparently related to poor physical HRQoL. 34 In the present study, sleep deprivation was significantly and positively related to worst pain and average pain.
Pain management is a continuing challenge in MPS treatment. Table 5 compares the results of five intervention studies. Two (2) studies reported an association between long pain duration and poor prognosis. 27,35 Two (2) large-scale, long-term studies identified an association between high-intensity pain and poor prognosis. 27,28
Hsieh YL, Kao MJ, Kuan TS, et al. Dry needling to a key myofascial trigger point may reduce the irritability of satellite MTrPs. Am J Phys Med Rehabil 2007;86:397–403.
MTrPs, myofascial trigger points.
The following limitations to this study are acknowledged. First, sample size was inadequate for demonstrating improvement in all measurements taken. Second, this study cannot be considered a systemic comprehensive clinical trial since psychologic factors such as dysfunctional pain cognition and mistaken beliefs about pain were not considered.
Conclusions
Although this study found that dry-needling of trigger points combined with muscle-stretch techniques decrease pain intensity and aggregated pain interference, the study design does not permit a conclusion on causality. However, a reasonable interpretation is that this treatment has great potential for improving the quality of pain management in patients with MPS. Predictors of poor outcome in this study were long pain duration, high intensity of pain, poor quality of sleep, and repetitive work. Treatment outcome depends not only on the specific dry-needling protocol, but also on the disease characteristics and patient demographic profile.
Footnotes
Disclosure Statement
No competing financial interests exist.