
Abstract
Background:
Bipolar disorder (BD) is a debilitating syndrome that is often undiagnosed and undertreated. Population surveys show that persons with BD often self-medicate with complementary and alternative medicine (CAM) or integrative therapies in spite of limited research evidence supporting their use. To date, no review has focused specifically on nonconventional treatments of BD.
Objectives:
The study objectives were to present a review of nonconventional (complementary and integrative) interventions examined in clinical trials on BD, and to offer provisional guidelines for the judicious integrative use of CAM in the management of BD.
Methods:
PubMed, CINAHL,® Web of Science, and Cochrane Library databases were searched for human clinical trials in English during mid-2010 using
Results:
Several positive high-quality studies on nutrients in combination with conventional mood stabilizers and antipsychotic medications in BD depression were identified, while branched-chain amino acids and magnesium were effective (small studies) in attenuating mania in BD. In the treatment of bipolar depression, evidence was mixed regarding omega-3, while isolated studies provide provisional support for a multinutrient formula, n-acetylcysteine, and
Conclusions:
Current evidence supports the integrative treatment of BD using combinations of mood stabilizers and select nutrients. Other CAM or integrative modalities used to treat BD have not been adequately explored to date; however, some early findings are promising. Select CAM and integrative interventions add to established conventional treatment of BD and may be considered when formulating a treatment plan. It is hoped that the safety issues and clinical considerations addressed in this article may encourage the practice of safety-conscious and evidence-based integrative management of BD.
Introduction
Despite this, few studies have been done on nonconventional treatments of BD. Other than a review by Andreescu and colleagues, 9 there is a paucity of peer-reviewed publications reporting clinical trial outcomes and safety issues associated with nonconventional treatments of BD. While their article is significant for providing the first review in this area, its focus is primarily on unipolar depression, and it does not review nutritional interventions in detail, many of which are effective adjunctive interventions when combined with conventional pharmacotherapies. 10 The Andreescu et al. review is also limited by excluding studies published over 10 years ago. In the present article, evidence is critically reviewed for CAM and integrative treatments of bipolar depression, mania and hypomania, and recommendations are made for provisional clinical guidelines.
Methods
PubMed, CINAHL,® Web of Science, and Cochrane Library databases were searched during mid-2010 first for research in the overarching area of BD; then for human clinical trials using the terms
Bipolar Disorder
Etiology
BD is a mental illness that affects approximately 1%–2% of adults in their lifetime. When milder subclinical presentations are included, the prevalence rate increases to approximately 4%. 12 First-degree relatives of bipolar individuals are significantly more likely to develop the disorder than the population at large, and twins have a 70% risk of sharing the disorder. 13 Although not yet fully elucidated, BD symptoms are probably caused by dysregulation of serotonergic and dopaminergic pathways, and diminished activity in the hippocampus and prefrontal cortex. 14,15 It has been suggested that abnormal activity in hypothalamic circuits involved in maintaining normal circadian rhythms manifest as the affective and behavioral symptoms of BD. 15
Diagnosis
According to current conventional Western psychiatric nosology, BD diagnosis is divided into Bipolar Disorder Type I (BD I) and Bipolar Disorder Type II (BD II; Table 1), and can be differentiated from unipolar depression (major depressive disorder) by the presence of manic or hypomanic (lesser) episodes. 16 A manic episode is a complex symptom pattern that may encompass disparate affective, behavioral, and cognitive symptoms, including pressured speech, racing thoughts, euphoric or irritable mood, agitation, inflated self-esteem, distractibility, excessive or inappropriate involvement in pleasurable activities, increased goal-directed activity, diminished need for sleep, and in severe cases, psychosis. 16
A history of depressive episodes is not required for a formal diagnosis of BD I, according to the Diagnostic and Statistical Manual of Mental Disorders version IV (DSM-IV-TR). 16 In contrast, BD II can be diagnosed only in cases when at least one hypomanic episode and at least one depressive episode have been documented. In both disorders, moderate or severe depressive episodes typically alternate with manic symptoms; however, in “mixed mania,” symptoms of mania and depressed mood overlap. Another variant called rapid cycling is diagnosed when at least four complete cycles of depressed mood and mania occur during any 12-month period. A mild variant of BD, cyclothymic disorder, is diagnosed when several hypomanic and depressive episodes take place over a 2-year period in the absence of severe manic, mixed, or depressive episodes. 16 The emerging concept of a “mood spectrum” hypothesis suggests that patterns of depressive and manic symptoms occur along a continuum, and that “mood disorders” do not exist as discrete diagnostic entities. 17,18 Evidence supports that unipolar depression and bipolar II depression occur across a spectrum, with 30% of patients diagnosed with major depressive disorder experiencing various bipolar symptoms (e.g., agitation, racing thoughts, and decreased sleep). 17 While BD I presents as a distinct psychiatric disorder that fulfills specific diagnostic criteria, BD II and cyclothymic disorder are more variable in presentation.
It is estimated that two thirds of individuals diagnosed with BD experience moderate or severe symptoms in any given year. 19 Bipolar patients experience depressive symptoms three times more often than mania, and five times more often than rapid cycling or mixed episodes. 20 A diagnosis of BD is one of the highest risk factors for suicide. 21 BD usually presents in a rhythmic manner, oscillating between episodes of mania and depression, with several risk factors and triggers contributing to the rate of relapse and failed response to treatment (Fig. 1).
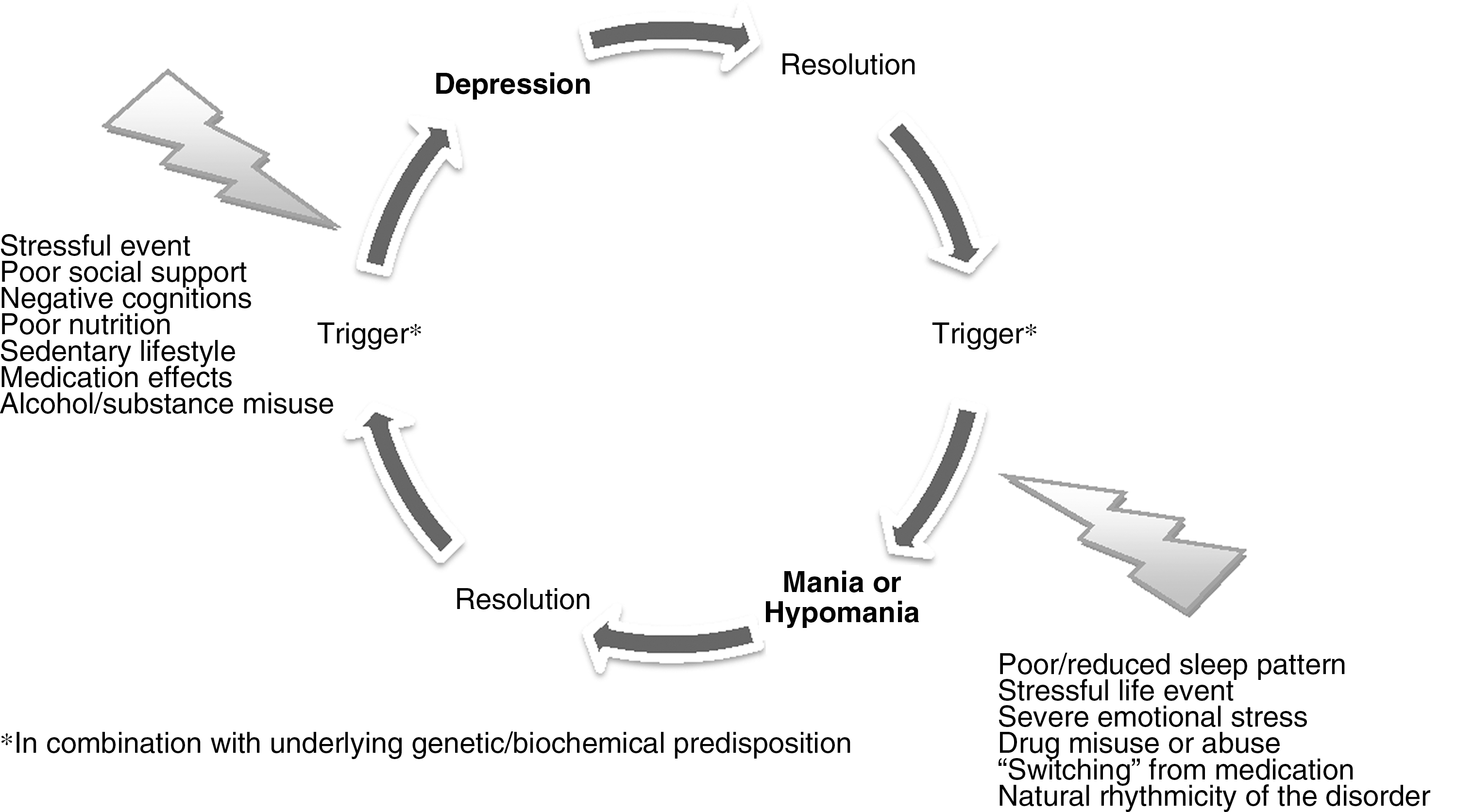
Basic cycle of bipolar disorder.
Conventional treatment
Conventional pharmacotherapies are an important and often necessary treatment of both the depressive and manic phases of BD. First-line treatments of BD include mood stabilizers (e.g., lithium carbonate, carbamazepine, and valproate), antidepressants, antipsychotics, and sedative–hypnotics. 15,19 Antipsychotics are used to treat agitation and psychosis, which occur frequently in acute mania, and select antipsychotics have been found to be effective mood stabilizers. Sedative-hypnotics are sometimes prescribed for the severe insomnia that accompanies mania, as well as for daytime management of agitation and anxiety. 22
Side-effects often occur with these medications, having a mixed record of success due to their limited efficacy and high rates of treatment discontinuation. 21 Fewer than half of patients who take a conventional mood stabilizer or other psychotropic medications following an initial manic episode report sustained control of their symptoms. 23 As many as one half of all bipolar patients who take mood stabilizers do not experience good control of their symptoms or refuse to take medications, and approximately 50% discontinue their medications because of serious adverse effects including tremor, weight gain, thyroid dysfunction, elevated liver enzymes, and many others. 24 People diagnosed with BDs should be maintained on a consistent, long-term pharmacotherapeutic regimen to reduce the rate of rehospitalization, and increase chances of full remission. 25 In patients diagnosed with BD, stressors, seasonal change, reduced sleep, and stimulants or recreational drug use may provoke an episode of hypomania (although sometimes the trigger may have no apparent cause). 15 Regular exercise, good nutrition, a strong social support network, and a predictable low-stress environment help reduce relapse risk. 19, 26 –28
Psychotherapy and psychosocial interventions in stable bipolar patients may potentially reduce relapse risk by providing psychologic support, enhancing medication adherence, and helping patients address warning signs of recurring depressive or manic episodes before more serious symptoms emerge. 27 Relapse prevention usually involves use of “life charts” and an effective stress management plan. An example is the novel BD relapse prevention program (called MAPS), which has evidence in reducing relapse of mania and BD depression. The Australian-developed MAPS program was studied in a clinical trial involving 84 participants with BD, and was conducted over 12 weeks. 29 Participants were randomized to either the program involving education on BD (symptoms, monitoring triggers, and symptom management skills), in addition to goal setting, medication management, and relapse prevention planning; or a control group consisting of treatment as usual plus telephone calls. Results revealed that participants who received the group-based intervention were significantly (p=0.04) less likely to have a relapse of mania or depression, and spent less time unwell.
Clinical considerations
When considering recommending CAM or integrative treatments for BD (in concert with traditional psychotropic medications), it is essential to first carefully examine the evidence for both conventional and nonconventional therapies. In this article, an integrative model is proposed that incorporates select CAM therapies in combination with conventional psychotropic medications. We recommend against the use of CAM or integrative therapies whose safety and efficacy is not supported by strong research evidence. This caveat applies even more so to the management of severe symptoms of bipolar depression or mania. Mental health care providers should always recommend those therapies supported by the highest level of evidence, 30 and in spite of their limited efficacy and unresolved safety issues, mood stabilizers and select antipsychotics should always be regarded as the first-line treatments of the severe form of bipolar illness (i.e., BD I). 31
Prior to diagnosing bipolar mood disorder, a period of mania or hypomania lasting several days must be established in the context of a broader pattern of impairment that may include decreased need for sleep, flight of ideas, grandiosity, excessive or unrealistic spending, or hypersexual activity. A life chart can help establish a pattern of cyclic mood changes and associated impairments in social activity, academic performance, and work. An important initial consideration when prescribing CAM in persons diagnosed with BD depends upon which phase are they in (i.e., mania, depression, or remission). A careful history is needed to establish a persisting pattern of mood changes fluctuating between depression and mania or hypomania. Conventional laboratory tests and functional brain imaging studies can be used to rule out medical disorders that can mimic symptoms of depressed mood or mania including, for example, thyroid disease, strokes (especially in the right frontal area of the brain), multiple sclerosis, seizure, or other neurologic disorders. 32 Irritability or euphoria alternating with periods of depressed mood is sometimes associated with chronic abuse of stimulants, marijuana, or other drugs. Thus, screening for substance abuse should be done before a formal diagnosis of BD is made. 33
In persons in the manic phase of BD type I, hospitalization is usually required, at which time adjunctive use of magnesium, choline, branch-chained amino acids, or
For patients in the depressed phase, the treatment approach is different. It is important to note that depression symptoms are often misdiagnosed as major depressive disorder when in fact they are the depressive phase of BD. Thus, careful screening is essential in all patients presenting with depressed mood including assessment of the length, frequency, and severity of depressive episodes, identification of precipitating stressors, and evaluation of suicidality. Assessment should include a urine drug and alcohol screen and a review of their sleep pattern and level of stress. CAM therapies for bipolar depressed patients include select nutrients (
All bipolar patients being treated for depressed mood are at risk of “switching” to mania and should be closely monitored. A personalized relapse prevention program including patient and family education about early warning signs of recurring depressed mood or mania, and a well-thought-out plan is an essential component of care for all bipolar patients. Important safety considerations are raised by the use of CAM therapies that have efficacy in major depressive disorder but that have not been established as safe in bipolar depressed mood and found to not increase the risk of switching to mania. Case reports implicate select natural products used to treat major depressive disorder, such as Hypericum perforatum,
41
Ephedra sinica,
42
or
A significant percentage of individuals diagnosed with BD use nonpharmacologic modalities adjunctively with prescription medications. However, with the exception of the nutrient interventions reviewed in this article, there is relatively little evidence for the safety and efficacy of the majority of such integrative treatments. Finally, while exercise should be encouraged in all BD patients because of established benefits to general health and mood, those patients taking lithium should consult their physician before starting a rigorous exercise program. Lithium is excreted with perspiration, and strenuous physical activity that involves significant sweating may lower lithium levels in the blood; at least one such case has been reported. 46
Clinical Evidence of CAM in BD
Omega-3
Countries where there is high fish consumption have relatively lower prevalence rates of BD. 47 Several clinical trials have studied omega-3s including fish oil and purified eicosapentaenoic acid (EPA) or docosahexaenoic acid (DHA), as a monotherapy or as an adjunctive intervention in BD. An early RCT involving 44 participants using a combination of EPA and DHA (9.6 g/day) with conventional drug therapies revealed positive results on measures of depressed mood in terms of response and remission rates on The Hamilton Depression Rating Scale (HAMD) (d=1.40). 48,49 No significant effect on mania outcomes occurred. A 26-week open-label adjuvant study by Osher and colleagues 50 in 12 participants with BD I revealed that 8 of 10 participants with 1 month of EPA were responders on HAMD (d=1.23). It should be noted that while these open-label studies are positive, confidence in these should be tempered because they are not controlled. A 12-week, three-arm controlled study involving 75 participants using 1 g or 2 g of EPA combined with any class of psychotropic medication revealed a small but significantly greater reduction on the HAMD from either dose, compared with placebo (1 g: d=0.90, 2 g: d=0.50). 51 However, no significant effect for mania was achieved on The Young Mania Rating Scale (YMRS). 52 A later RCT conducted by the research group 53 using 2 g of EPA versus placebo over 12 weeks in 14 female participants with BD I revealed positive, but not statistically significant effects on depression outcomes. A novel 4-week adjunctive study involving 21 participants with BD I by Hirashima and colleagues 54 revealed no significant differences between EPA 5 g plus DHA 3 g and a nontreatment control. Interestingly, however, brain resonance imaging showed that T2 levels were reduced in the treatment group, denoting increased neuronal cell membrane fluidity (Table 2).
✓ Potential use in bipolar mania or bipolar depression; NK, not known; BCAA, branch chain amino acids; A, Several repeated clinical trials (with some positive results); B, unreplicated positive study; C, small study, or inconclusive results; D, several clinical trials reveal mainly negative results.
A larger study (n=121) using 6 g of EPA in combination with at least one mood stabilizer in patients diagnosed with rapidly cycling bipolar disorder also found no benefit over placebo on reducing mania on YMRS. 55 Also, a small RCT with 15 participants, using 4.4 g of EPA and 6.6 g of DHA/day adjunctively with 20 mg/kg/day of valproate, also revealed no benefit over placebo for reducing mania. 56 Two open label studies have been published on omega-3s in pediatric BD: an adjuvancy study and a monotherapy study. Clayton et al. 57 conducted a 6-week study involving 18 adolescents with BD I or II using omega-3 (DHA 1560 mg and EPA 360 mg per day) and found significantly reduced clinician-rated mania and depression from baseline. A study by Wozniak and colleagues 58 also revealed significant reductions on YMRS (d=0.90) and BPRS (d=0.83) compared to baseline using 1290 mg–4300 mg of fish oil in 20 adolescents who met DSM-IV-TR criteria for BD and had a YMRS score of >15.
Current evidence weakly supports use of omega-3 preparations in combination with conventional psychotropic medications in the depressive phase of BD; however, omega-3s probably have little or no clinical effect in attenuating mania. Although considered a very safe intervention, rare cases of increased bleeding times, but not increased risk of bleeding, have been reported in patients taking aspirin or anticoagulants together with omega-3s. 35
Amino acids
Bipolar patients may be genetically susceptible to mood swings when certain amino acids or other micronutrients are lacking in the diet. 59 Findings of two small RCTs suggest that certain branch-chained amino acids may rapidly improve acute mania by interfering with synthesis of norepinephrine and dopamine. 60 In one study, 25 bipolar patients randomized to a blend of the branch-chained amino acids leucine, isoleucine, and valine (60 g/day) versus placebo experienced significant reductions in the severity of mania within 6 hours. 60 Reductions in mania were sustained with repeated administration of the amino acid drink. N-acetylcysteine (NAC) is an amino acid with strong antioxidant properties that has been used to treat a range of inflammatory disorders. 61 In novel research, Berk and colleagues 62 conducted a 24-week RCT using 1 g twice per day of NAC versus placebo in a sample of 75 participants stable on medication or therapy with DSM-IV-TR-diagnosed BD I or BD II. Results revealed that NAC significantly reduced bipolar depression on the Montgomery Depression Rating Scale (MADRS) 63 and the Bipolar Depression Rating Scale with strong effect sizes respectively of 1.04 and 0.83. No significant effect was found on mania outcomes, although it should be noted that YMRS mania levels were very low; thus, significant changes were unlikely to occur.
Restricting or excluding
Vitamins and minerals
Magnesium may be an effective adjunctive therapy for treatment of acute mania or rapidly cycling BD. In a small open trial, oral magnesium supplementation had comparable efficacy to lithium in rapid cycling bipolar patients. 66 In a small case series, intravenous magnesium sulfate used as an adjunctive with lithium, haloperidol, and a benzodiazepine in bipolar patients with severe treatment-resistant mania resulted in significant improvement in global functioning and reduction in the severity of mania. 67 Many patients treated with intravenous magnesium sulfate remained stable on lower doses of conventional medications. An RCT used 375 mg of magnesium oxide versus glucose placebo over 16 weeks in 20 participants with prior DSM-IV diagnosed mania and >6 months on a stable mood stabilizer (verapamil). Results revealed a significant reduction on mania compared to control at week 16. 68
Two (2) clinical trials using inositol (12 g and 5–20 g) adjunctively with maintenance doses of mood stabilizers have been conducted. Both RCTs 69,70 had small samples (n=24 and 26, respectively), and were conducted over 6 weeks. Results in both studies revealed no significant differences between inositol or placebo on depression or mania outcome scales. Clinical response, however, was noted in 12/21 participants taking inositol on pooled results of both studies on HAMD and MADRS.
Folic acid has been studied in one early trial as an adjunctive in BD patients stabilized on lithium. A 52-week RCT by Coppen and colleagues 71 compared 200 μg of folic acid versus placebo tablets in 102 participants taking lithium. Results revealed that the completers in the folic acid group (n=41) had significantly lower Beck Depression Inventory scores than the control group, with a strong effect size of 1.07.
A proprietary 36-ingredient formula of vitamins and minerals may significantly reduce symptoms of mania, depressed mood, and psychosis in bipolar patients when taken alone or used adjunctively with conventional mood stabilizers. Six (6) of 11 completers had clinical response with strong effect sizes (HAMD: 1.70, YMRS: 0.83). In one case series, 11 bipolar patients who completed a 6-month protocol were able to reduce their conventional mood stabilizers by half while improving clinically. 72 In another case series, 13 of 19 bipolar patients who continued on the nutrient formula remained stable after discontinuing conventional mood stabilizers. 73 Some patients stopped taking the formula because of nausea and diarrhea, and 3 patients resumed conventional mood stabilizers because of recurring manic symptoms. Researchers believe the formula works by correcting metabolic errors that result in bipolar-like symptoms in genetically predisposed individuals when certain micronutrients are deficient in the diet. 74,75
Choline is necessary for the biosynthesis of acetylcholine, and abnormal low brain levels of acetylcholine may contribute to some cases of mania. 76 Findings of a small open study suggest that phosphatidylcholine (15 g–30 g/day) may reduce the severity of mania and depressed mood in bipolar patients. 77 It should be noted that two nonresponders were also taking hypermetabolic doses of thyroid medication. Clinical improvement correlated with increased intensity of the basal ganglia choline signal as measured on proton magnetic resonance imaging. The effect of choline on depressive symptoms was variable. 77
Findings of a small open study suggest that patients diagnosed with BD who exhibit mania or depressed mood may respond to low doses (50 μg with each meal) of a natural lithium preparation. 78 Post-treatment serum lithium levels were undetectable in patients who responded to trace lithium supplementation. Findings from animal research and a small open study suggest that bipolar patients who take potassium 20 mEq twice daily with their conventional lithium therapy experience fewer side-effects, including tremor, compared to patients who take lithium alone. 79 No changes in serum lithium levels were reported in patients taking potassium. Pending confirmation of these findings by a larger double-blind trial, potassium supplementation may provide a safe, cost-effective integrative approach for the management of bipolar patients who are unable to tolerate therapeutic doses of lithium due to tremor and other adverse effects (patients who have cardiac arrhythmias or are taking anti-arrhythmic medications should consult their physicians before considering taking a potassium supplementation).
Herbal medicines
Findings of a large 12-week placebo-controlled trial involving a sample of 58 BD patients suggest that a proprietary Chinese compound herbal formula consisting of at least 11 herbs may enhance the effect of conventional mood stabilizers for treatment of the depressive phase of BD. 80 Bipolar depressed (but not manic) patients randomized to the herbal formula plus carbamazepine experienced significantly greater reductions in the severity of depressed mood compared to matched patients receiving a mood stabilizer only. These findings were replicated in a subsequent study, which confirmed that bipolar depressed patients treated with the herbal formula improved more than patients treated with a placebo, with a strong effect size (d=0.98) between treatments at week 12. 80
Early studies suggested that the Ayurvedic plant medicine Rauwolfia serpentina and an alkaloid derivative, reserpine, was an effective treatment of BD by augmenting the antimanic efficacy of lithium without risk of toxic interactions. 81,82 However, therapeutic use of this plant in various Western countries is restricted due to the presence of the alkaloid reserpine, which has potent effects on blood pressure and the central nervous system. A previous review published in Journal of Alternative and Complementary Medicine 83 of placebo-controlled trials comparing H. perforatum to placebo or conventional antidepressants concluded that the herbal medicine is potentially beneficial for mild to moderate depressive symptoms. Although this herb may potentially be beneficial in the depressive phase of BD, no studies on this have been conducted to date. Several case reports of mania induction with St. John's wort 41,84 and potential serious interactions with many drugs 85 have resulted in limited use of this herbal for the treatment of BD.
Acupuncture
The art of acupuncture has been used for millennia in Eastern cultures for treating a range of illnesses including mental disorders. Research in the area of unipolar depression has revealed mixed but mainly positive results. A two-part clinical trial has been conducted examining the safety, effectiveness, and acceptability of adjunctive acupuncture in the treatment of hypomania and depression associated with bipolar disorder. 86 In the first study, 20 patients experiencing symptoms of mood elevation were given targeted acupuncture (points specific to symptoms) versus “sham” acupuncture (nonacupoint needling) over 12 weeks, while for 26 patients experiencing symptoms of depression, targeted acupuncture was compared to (off the meridian) acupuncture for nonpsychiatric health concerns over 8 weeks. While the results revealed that acupuncture treatment reduce of symptoms (mood elevation in Study I, depression in Study II), a nonstatistical difference occurred between treatments, with all patients experiencing improvement over the course of study (Fig. 2).

Treatment decision tree (adapted from Lake, J. in Sarris, J. and Wardle, J 1 . Clinical Naturopathy: An Evidence-Based Guide to Practice © 2010, Elsevier, Australia). BP, bipolar disorder; TSH, thyroid-stimulating hormone; CAM, complementary and alternative medicine.
Conclusions
Bipolar disorder may potentially be effectively managed using an integrative approach. While use of select nutrients combined with medication in BD is supported by strong evidence, to date herbal medicines have not been adequately evaluated. Surprisingly, other CAM modalities potentially used by bipolar patients are currently not supported by clinical trial evidence. Interventions such as manual therapies (e.g., acupuncture, massage), dietary modification, meditation, or mind–body practices (e.g., t'ai chi or yoga) are supported by some evidence in psychiatric disorders; however, their beneficial effects in patients diagnosed with BD are currently unknown or inconclusive. However, while these interventions may not be “directly effective” in the treatment of BD, they have general beneficial effects on physical and mental health and quality of life, are probably associated with reduced stress and improved functioning in general, and thus may potentially reduce the severity of bipolar symptoms and risk of relapse. It is hoped this article illuminates the current evidence of CAM for the integrative management of BD, and may encourage further discussion and research in this area.
Footnotes
Acknowledgments
This publication is a collaboration from The International Network of Integrative Mental Health (
Disclosure Statement
No competing financial interests exist.