
Abstract
Background:
This study aimed to evaluate the effects of noninvasive acupoint stimulation therapy with middle-frequency electrical waves on dysmenorrhea in young women.
Methods:
This randomized controlled trial enrolled 66 gynecology patients who had primary dysmenorrhea, which was defined as painful menstruation without pelvic pathology (secondary dysmenorrhea). Pathology was ruled out by gynecological ultrasound examination and serum concentration of CA-125. Subjects were randomly assigned to an experimental group (n=34) and control group (n=32). Main outcome measures included McGill Questionnaire Short-form and numerical rating scale for pain intensity. Acupuncture-like trancutaneous electrical nerve stimulation (AL-TENS) of middle-frequency (1000 Hz–10,000 Hz) was applied at Hegu (LI4) and Sanyinjiao (SP6) points in the experimental group twice weekly for 8 weeks; the control group received AL-TENS on nonacupoints. Pre- and postintervention results were recorded.
Results:
Prior to AL-TENS intervention, no significant differences were found in pain scale and pain intensity between experimental and control groups. After AL-TENS intervention, average total pain score in the experimental group was significantly lower than in the control group (experimental group 2.9±1.2, control group 5.4±2.2; p<0.001). Significant differences were observed between experimental and control groups in average change in pain scores between pre- and postintervention (experimental group 4.5±1.9, control group 1.39±2.0; p<0.001). Pain severity at postintervention was also significantly different between groups (p<0.001).
Conclusions:
Noninvasive electro-acupuncture stimulation therapy with middle-frequency electric waves applied at both Hegu (LI4) and Sanyinjiao (SP6) acupoints mitigates pain in dysmenorrhea.
Introduction
Dysmenorrhea is prevalent among adolescent girls and young women in their 20s and has been estimated to be more than 75% globally. 4 It is one of the most common gynecologic problems causing young women to seek medical care. 3 Estimates of prevalence vary around the world, ranging from 56.4% in mainland China 5 to 51% in Turkey, 6 67% in Sweden, 7 80% in Western Australia, 8 85% in Spain 9 and 60–90% in the United States. 1,10 One recent study reported a prevalence rate of 73.3% among Taiwanese high-school girls (average age 16.7 years). 11 An estimated 42–51% of dysmenorrheic young women reported missing either school or work due to severe menstrual pain. 12 Dysmenorrhea affected performance in work and school, daily activities, social life and quality of life. 9
Many factors have been shown to be associated with dysmenorrhea. Chung et al. (2005) conducted a study of nurses in Taiwan, finding that 30% complained of dysmenorrhea. 13 In that study population, age, marital status, and perceived life satisfaction were significantly related to dysmenorrhea. In the study conducted by Banikaraim et al., 58% of women suffering from dysmenorrhea chose bed rest and 52% took medications to relieve pain, while only 14% sought medical assistance. 9
Treatment of primary dysmenorrhea relies on the differential diagnosis to distinguish between primary and secondary dysmenorrhea. Besides initial pelvic examinations, underlying causes of secondary dysmenorrhea are usually identified through gynecologic ultrasound and assays for cancer antigen 125 (CA-125). The upper limit of normal range for CA-125 is 35 U/mL, and elevated values can be a sign of endometriosis, pelvic inflammatory disease, intrauterine adhesions, congenital malformations, ovarian chocolate cysts, ovarian cancer, adenomyoma, uterine polyps, or other pathology. 14
If pelvic pathology is completely ruled out, primary dysmenorrhea is treated according to severity of symptoms, including pain relief (e.g., nonsteroidal anti-inflammatory drugs), use of oral contraceptives to inhibit ovulation, dietary measures (e.g., low-fat or vegetarian diet and omega-3 fatty acid supplements), topical low-level heat treatment, and also reassurance and education about the condition. Surgery is generally not indicated for primary dysmenorrhea. 3 Other alternative therapies have been investigated although not extensively, including acupuncture 15 and acupressure. 16 A randomized, controlled prospective clinical study was conducted in 1987 to investigate the effectiveness of acupuncture in managing the pain of primary dysmenorrheal. The result of a clinical trial indicated a 41% reduction of analgesic medication use by women in the experimental acupuncture group compared to controls receiving random point or “sham” acupuncture. 17
Acupuncture-like transcutaneous electrical nerve stimulations (TENS) has been used to alleviate the neuropathic pain and chronic pain associated with cancer treatments. 18,19 The present study investigated the effects of acupuncture-like transcutaneous electrical nerve stimulation (AL-TENS) at Hegu (LI4) and Sanyinjiao (SP6) acupoints 20 on the changes in abdominal pain associated with primary dysmenorrhea.
Materials and Methods
Patients
The study was conducted between March 1 and May 31, 2008. Patients were recruited from the gynecology department of Taiwan Adventist Hospital, a regional teaching hospital in Taipei, Taiwan. A total of 66 subjects were enrolled and randomly allocated into an experimental group (n=34) and a control group (n=32). Average age in the experimental group was 27.0±4.6 and 26.9±5.4 in the control group. Inclusion criteria included women who had regular menstrual cycles and who had been diagnosed with primary dysmenorrhea, were not pregnant, and were symptomatic within the past 6 months. Primary dysmenorrhea was defined as painful menstruation without pelvic pathology, which excluded patients with secondary dysmenorrhea whose pain arose from a definitive gynecologic condition. Primary dysmenorrhea was confirmed by negative pelvic ultrasound examination performed by study gynecologists and a serum CA-125 value of <35 U/mL (or decreased to 40 U/mL on a second serum sample). Subjects were excluded if any pelvic pathology was identified by pelvic ultrasound examination and/or if serum CA-125 value was elevated (>35 U/mL).
To comply with medical ethics principles and respect the rights of study subjects, researchers explained the purpose of this research and its related safety measures before recruitment. All study procedures were approved by the committee at the National Taipei College of Nursing, and all patients included in the study agreed to participate and signed the informed consent form. Full compliance with the Helsinki Declaration was applied during the study.
Study design
After obtaining informed consent from all study subjects, researchers collected demographic data and recorded patients' baseline values for the main outcome measures of the study, including the short-form of the McGill Pain Questionnaire (SF-MPQ) and the numerical rating scale (NRS) for pain intensity. The SF-MPQ and NRS were again applied after patients completed the 16th intervention session and postintervention values were recorded.
Instruments
For evaluating subjects' pre- and postintervention pain associated with dysmenorrhea, the pain level of dysmenorrhea was measured by the SF-MPQ. 21
The Chinese SF-MPQ used in evaluating the women's pain perception showed good internal consistency (Cronbach's α=0.61–0.63). 22 The MPQ focuses on pain evaluation and is widely used to evaluate childbirth pain, postsurgical pain, cancer pain, and various types of chronic pain. 20 In the SF-MPQ, descriptors 1–12 (throbbing, shooting, stabbing, sharp, cramping, gnawing, hot-burning, aching, heavy, tender, splitting, and sore) represent the sensory dimension of pain experience and 13–16 (tiring–exhausting, sickening, fearful, punishing–cruel) represent the affective dimension. The questionnaire is scored using a four point Likert scale (0=no pain, 1=mild; 2=moderate, and 3=severe). Pain scores are derived from the sum of the intensity ratings for the sensory and affective scale. 23
Changes in chronic pain intensity were measured by the NRS, an 11-point numerical pain rating scale developed by Farrar et al. in 2001. 24 Higher scores indicate greater pain intensity. The NRS categorizes intensity of pain as mild (scores 1–3), intermediate (scores 4–6), and severe (scores 7–10).
Intervention
In this study, AL-TENS therapy was delivered by the Middle-frequency Electrical Stimulator (GM390TE; “GEMORE” Multi-Function Electrotherapy Stimulator). The electrodes were made of optic fiber. This device provides a noninvasive method requiring only attachment of electrical spacers onto the skin surface to deliver low-level electrical waves. For the TENS therapy, <1000 Hz was routinely defined as low frequency, 1000–10,000 Hz as middle frequency, and >10,000 Hz as high frequency. The frequency used in this study was 120 Hz per second with 8 middle frequency short pulses (8pps). The instrument has two operation modes (Mode 1: 4000 Hz; Mode 2: 2500 Hz) and a digital display for the operation settings. Modulation of the frequency is achieved by adjusting the intensity. The frequency and intensity of stimulation was adjusted until a tolerable level was reached for each subject; this may mean a higher frequency with intensity that does not produce motor contraction or lower frequency with an intensity that does result in motor contraction. For all patients and controls, the therapy started at Mode 2. If the patients did not perceive any numbness/tingling feelings at the treatment site for Mode 2, 5 minutes after the beginning of the therapy, the frequency was increased to Mode 1.
The instrument was operated by researchers during the whole research process. Subjects assumed comfortable sitting positions, and the electrical spacers were attached to the acupoints of Hegu (L14) on both hands and the acupoints of Sanyinjiao (SP6) on both legs. 20 The stimulation lasted for 20 minutes and was performed twice a week for 8 weeks, for a total of 16 sessions. For the control group, Mode 2 was used to stimulate two pseudopoints on both hands and two pseudopoints on both legs instead. During the stimulation, researchers supervised and observed responses of study subjects. If any discomfort was noted, immediate pause of treatment was applied and, if discomfort was determined to be too strong for the patient, consideration was given to excluding the subject from further treatment. No patients were excluded during the 16 sessions.
Statistical analysis
Data were expressed as mean±standard deviation, and n (%) for continuous, and categorical parameters. A box-plot graph showed changes in total scores of MPQ-SF questionnaires, and a bar chart showed dispersion of pain severity. Two-tailed t test and Fisher's exact test were performed to compare differences between groups. Statistical significance was established as p<0.05. Statistical analyses were performed using SPSS 15.0 statistics software (SPSS Inc., Chicago, IL).
Results
Preintervention demographics and clinical characteristics were not significantly different between groups (Table 1). Average age was 27.0±4.6 in the experimental group, and 26.9±5.4 in control group. Average total pain score of MPQ-SF at preintervention was 7.5±1.5 and 7.3±1.4 in experimental group and control group, respectively (p=0.664). Pain severity observed in the experimental group included 20 subjects (58.8%) who felt uncomfortable, 10 (29.4%) who felt pain, and 4 (11.8%) who felt severe pain. In the control group, 17 subjects (53.1%) felt uncomfortable, 14 (43.8%) felt pain, and 1 (3.1%) felt severe pain (p=0.260).
Data were expressed as amean±standard deviation, and b n(%).
Age of first menstruation; 1 subject in experimental group and 3 subjects in control group did not remember age of first menstruation.
p-values were determined by atwo-tailed t-test and bFisher's exact test.
MPQ-SF, short-form of the McGill Pain Questionnaire; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Changes in total scores of MPQ-SF by group are shown in Table 2 and Figure 1. Average total pain score of the experimental group was significantly lower than that of the control group (experimental group 2.9±1.2, control group 5.4±2.2, p<0.001). Average change of total pain score from preintervention score was significantly different between groups (experimental group 4.5±1.9, control group: 1.39±2.0, p<0.001). In addition, pain severity scores according to NRS were significantly different between groups (p<0.001) (Table 2). Pain severity seems to have decreased somewhat more in the experimental group than in the control group. Figure 2 shows changes of percentage of pain severity by group between pre- and postinterventions.
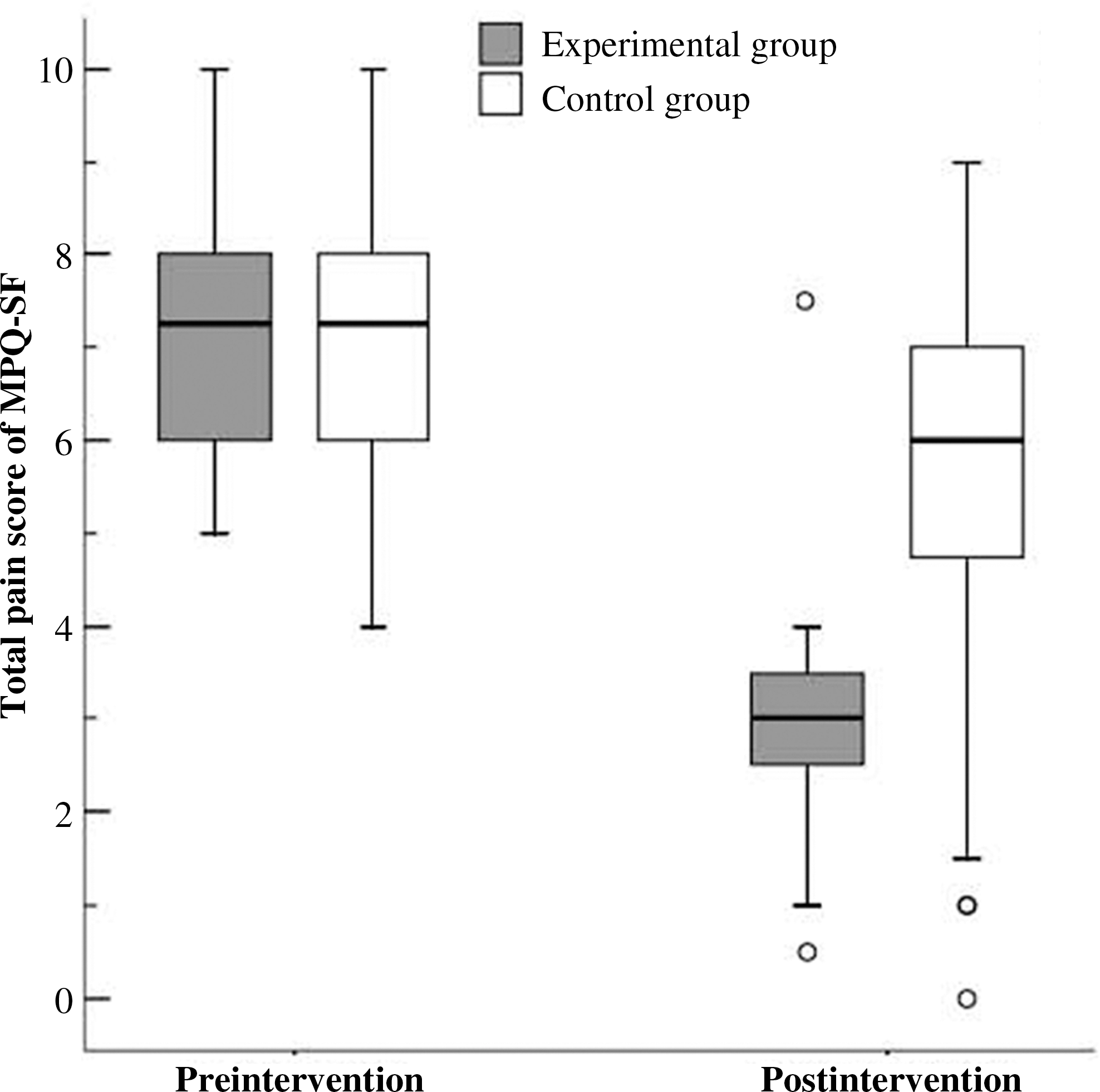
Box plot of total pain scores of short-form of the McGill Pain Questionnaire (MPQ-SF) in each category shows percentage of pain severity by group, between pre- and postintervention.
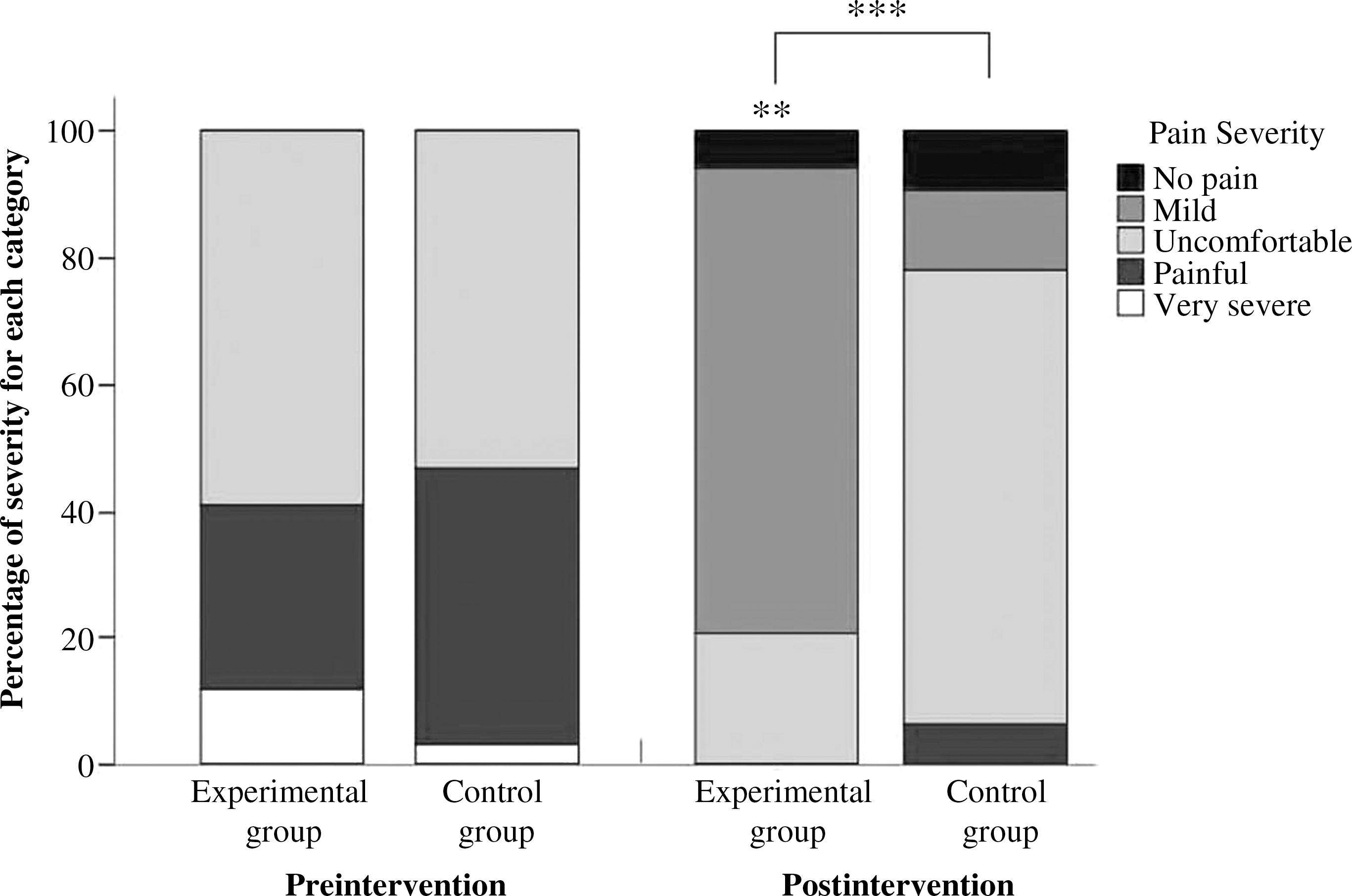
Percentage of severity for each pain level. **p<0.01 indicates that change in percentage of severity was significantly improved postintervention in the experimental group compared to preintervention. ***p<0.001 indicates that change in percentage of severity at postintervention was significantly different between experimental and control groups.
Data were expressed as amean±standard deviation, and b n (%).
p<0.001, through atwo-sample t test, and bFisher's exact test.
MPQ-SF, short-form of the McGill Pain Questionnaire.
Discussion
In this study, when study subjects with primary dysmenorrhea were evaluated prior to intervention, no significant differences were found in pain scale and pain intensity between the experimental group and the control group. After intervention of middle-frequency electrical waves to two distinct acupoints, Hegu (LI4) and Sanyinjiao (SP6), in the experimental group and nonacupoints in controls, the main findings were that the experimental group had significant differences in pain scale, pain intensity, and discomfort scale compared to the control group.
Noninvasive electrical stimulation therapy has been widely adopted for analgesic purposes in muscular rehabilitation. 15 To apply this technique, spacers are used to transmit small-pulse or middle-frequency electrical waves that pass through the skin at specific points, triggering nerves and muscular contractions. Subsequently, patients experience better full-range joint movements, increased vascular circulation, reduced muscle spasms, and reduced spasm-related pain. 15
AL-TENS is an accepted form of electrical stimulation therapy. It can be distinguished from the widely used TENS by the sites of stimulation. TENS focuses on the actual pain spots or areas close to them, and AL-TENS delivers stimulation therapy to specific acupoints reflecting the corresponding diseases being treated. These acupoints correspond to the points and meridians well understood and used by acupuncturists who use a traditional needling technique. Acupoint stimulation is believed to relieve pain through increasing the pain threshold and stimulating the production of endorphins. 25
Acupuncture itself has been used for treatment of gynecologic and obstetric conditions such as amenorrhea, menorrhagia, dysmenorrhea, infertility, and difficulties encountered in labor and delivery. In a pioneering study using acupuncture to mitigate the pain of primary dysmenorrhea in 43 women in four groups for 1 year, 10 of 11 women (90.9%) who received real acupuncture showed marked improvement (i.e., reduction in pain, compared with 4 of 11 [36.4%] who received placebo acupuncture). 17 The “real” acupuncture applied needles bilaterally on Gongsun (SP4) and Taixi (K3) points on the feet; Zusanli (ST36) on the knees; Zichong (ST30), Qugu (CV2) and Guanyuan (CV4) in the suprapubic region; and Neiguan (CX6) on the forearms. Results of that early study (1987) suggested that acupuncture was a viable option for managing dysmenorrhea. 17 In the present study, electroacupuncture stimulation therapy with middle-frequency electric waves was applied bilaterally at Hegu (LI4) and Sanyinjiao (SP6) acupoints on the hands and feet, respectively, in the experimental group, resulting in greater reduction of dysmenorrheal pain severity in that group than the application of AL-TENS stimulation at nonacupoints in a control group.
Middle-frequency electrical waves are defined as electrical waves with a frequency of 1000 Hz–10,000 Hz. Waves of this frequency have better tissue transmission than short waves and are able to infiltrate into deeper tissues. In recent years, electrical stimulation therapy has been applied for pain relief, 16 rehabilitation of muscle power in the limbs of patients who have had a stroke, 26 pelvic muscle training for patients with urinary incontinence, 27 nausea and vomiting after surgery or chemotherapy, 28 muscle soreness due to sports injury, 18 chronic pain associated with breast cancer treatment, 19 and improving the healing of wounds and bone fracture, 28 among other possible treatments.
As explained above, the intervention applied in the present study was a noninvasive electroacupuncture technique used to stimulate both Hegu (LI4) and Sanyinjiao (SP6) points on the hands and legs, respectively. These classically described meridians were selected for stimulation because of previously reported analgesic effects. 29 –31 Hegu (LI4) is located at the base of the V formed by the meta-carpal bones of the thumb and index finger. The cerebral areas activated by electroacupuncture of the right Hegu (LI4) point have been studied previously, notably by Wang et al. 30 The distribution of a signally deactivated area evoked by LI4 electroacupuncture was similar to the known distribution of anatomical orientation of pain in the brain, and closely related to the anatomical structure of the limbic system: areas that are possibly those of the cerebral regulating area influenced by the analgesic effect of electroacupuncture. 30
A prospective, randomized, double-blind study of 32 patients with bone fractures was conducted by Lang et al. (2007). 29 Acupressure was performed either at “true” points (e.g., Hegu [LI4]) or at “sham” points, meaning pseudo- or nonacupoints. Vital signs and pain and anxiety scores were recorded before and after the acupressure treatment. The trial concluded that acupressure in the prehospital setting effectively reduces pain and anxiety in patients with distal radial trauma. 29
In the current study, electroacupuncture was also applied to the Sanyinjiao (SP6) point located in the leg, 3 cm above the medial malleolus and posterior to the edge of the tibia. Another study similar to the current one used five instruments to collect pretest and post-test data at each acupressure intervention session, including (1) Visual Analogue Scale for pain; (2) the SF-MPQ; (3) the Menstrual Distress Questionnaire; (4) the Visual Analogue Scale for anxiety; and, for the experimental group only, (5) the Acupressure Self-Assessment Form. 31 Investigators compared results of using two matched acupoints with those of using a single point. Acupressure at Sanyinjiao (SP6) during the initial session reduced the pain and anxiety typical of dysmenorrhea. In the self-treatment follow-up session, acupressure at Sanyinjiao (SP6) significantly reduced menstrual pain but not anxiety. Thirty-one (31) (87%) of the 35 experimental participants reported that acupressure was helpful, and 33 (94%) were satisfied with acupressure in terms of its providing pain relief and psychologic support during dysmenorrhea. Findings of this group suggest that acupressure at Sanyinjiao (SP6) points can be an effective, low-cost intervention for reducing pain and anxiety in patients with dysmenorrhea. 31
This acupressure point has been shown to have an effect in dilation of the cervix and can be used to help the cervix to dilate efficiently. 32 Acupressure at Sanyinjiao point (SP6) reduced the duration and severity of pain of the active phase of labor, cesarean section rates, and necessity and amount of oxytocin administered. 32 Several investigators have studied the effects of Sanyinjiao (SP6) acupressure in reducing the pain level and menstrual distress resulting from dysmenorrhea. 32 –34 In one recent study, an acupressure group received 20 minutes of SP6 acupressure during the initial intervention session and was taught to perform the technique for themselves twice a day from the first to third days of their menstrual cycle, 3 months subsequent to the first session. Results indicated that SP6 acupressure had an immediate pain-relieving effect for dysmenorrhea. Moreover, acupressure applied to the SP6 acupoint for 3 consecutive months was effective in relieving both the pain and menstrual distress level resulting from dysmenorrhea. 33 A nonequivalent control group pre- and post-test design was employed in Korea to verify the effects of SP6 acupressure on skin temperature and dysmenorrhea. The trial concluded that acupressure to the SP6 meridian can be an effective noninvasive nursing intervention for alleviation of primary dysmenorrhea, with effects lasting more than 2 hours post-treatment. 34
Conclusions
In conclusion, the comparison in this study between pre- and postintervention evaluations of pain in young women with primary dysmenorrhea who received electrical acupoint stimulation is that the technique offers pain relieving benefits worthy of additional study. This initial trial suggests that noninvasive electroacupuncture stimulation therapy with middle-frequency electric waves applied at both Hegu (LI4) and Sanyinjiao (SP6) acupoints mitigates pain in dysmenorrhea.
Footnotes
Disclosure Statement
No competing financial interests exist.