
Abstract
Objectives:
The aim of this pilot study was to investigate the effects of therapeutic horseback riding on behavior, health-related quality of life, and motor performance in children with attention deficit hyperactivity disorder (ADHD).
Design:
The study employed a time series quasi-experimental design with two pretests and two post-tests conducted 8 weeks apart.
Setting/location:
The study was conducted at a riding school in Levanger, Norway.
Subjects:
The subjects comprised a convenience sample of 5 children aged 10–11 years with ADHD.
Methods:
Subjects received a 1-hour therapeutic horseback riding twice a week for 8 weeks as intervention.
Outcome measures:
Behavior and health-related quality of life was assessed using Strength and Difficulties Questionnaire (SDQ) and The KINDLR–Health-Related Quality of Life Questionnaire, respectively. The Modified Function-Neurological Assessment and the Movement Assessment Battery for Children assessed the subject's motor performance.
Results:
The pre- and post-tests scores were compared with the Wilcoxon paired sample tests and the Friedman test for nonparametric multiple test samples. Positive differences (p≤0.05) between the test results at pretest 2 and post-test 1 were noted for the behavior SDQ subscore “Total difficulties” reported by children (12.8±5.8), by parents (16.6±8.2), and by teachers (15.0±5.2). A significant difference (p<0.05) for the “Total difficulties” in SDQ was found between all 4 tests. In relation to quality of life, significant differences in the “Total score” (67.2±14.7) were reported by the children themselves. The motor performance improved after the intervention. The effect sizes and power were established.
Conclusions:
The results of the present study indicate that therapeutic horseback riding had a positive effect on 5 children with ADHD in several domains of the social role behavior, quality of life, and motor performance. This pilot study constitutes a good scientific prospect for future studies.
Introduction
Hippotherapy is used to increase strength, balance, posture, and function. 10 Therapeutic horseback riding is a physiotherapeutic treatment, using a horse as an implement, and the treatment strategy is using the multidimensional movement of the horse. It is assumed to have an effect in four different ways: sensomotoric, 11 neuromotoric, 12 psychomotoric, 13 and sociomotoric. 14,15
The main aim of therapeutic horseback riding is that the subject also will function better off the horse. The conceptual framework of therapeutic horseback riding may be explained by using dynamic system theory along with theories of motor learning and sensory integration 16 and neuropsychologic theories, wherein motor planning and intellectual abilities are positively stimulated through stimulation of the vestibular system.
Tyler 17 suggests that depressed, stressed, and angry persons can experience a positive effect from the physiologic reactions that occur as a result of the rhythmic movement of the horse. There are several other therapies using rhythmic stimulation as a method 18 –21 that indicate the same effects on motor performance. Basile 22 noted no psychologic effects on behavior and self-esteem in children with ADHD using Equine Facilitated Psychotherapy.
With its proposed effects on the four levels of sensomotor, neuromotor, psychomotor, and sociomotor abilities, therapeutic horseback riding has the potential to be an effective treatment intervention for children with ADHD, with an expectation of carryover into daily life.
The main objective of this pilot study was to reveal trends and effects of therapeutic horseback riding on children with ADHD using the Strength and Difficulties Questionnaire (SDQ), 23,24 KINDLR–Health-Related Quality of Life Questionnaire (HQoL), 25 Movement Assessment Battery for Children (MABC) 26 and Modified Function Neurological Assessment (MFNU)* as outcome measures. Secondary objectives were to indicate in which domains the positive alterations appear. Additionally, this pilot study was aiming to explore the scientific assumptions for future studies.
Materials and Methods
Subjects
A convenience sample of 5 children with ADHD participated. The researcher contacted the Norwegian Association for ADHD to recruit subjects. The subjects were required to have a primary diagnose of ADHD. The diagnosis was made by an independent psychiatric specialist team using standardized screening methods and a double-blind test procedure. The subjects, aged 10–11 years, who reacted positively on the medicament (Concerta®) and took the medicine for more than 1 year, were selected. Earlier horseback riding and severe comorbidities (e.g., severe behavioral problems such as obsessive–compulsive disorder) were exclusion criteria. Ten (10) children fulfilled the criteria and were willing to participate in the study. Finally, 5 subjects were selected at random. No girl participated due to the fact that no girl met the requirements.
Parental written consent was obtained. The study was approved by the Norwegian Ethical Committee and followed the principles outlined in the Declaration of Helsinki. All children had medical clearance to ride a horse and a referral for physical therapy from their primary physicians. The researcher did not know any of the subjects. The sample size was limited by pedagogic causes because children with this diagnosis and this form of therapy need a more individual approach.
Horseback riding
In this study, therapeutic horseback riding is understood to be a therapy that combines both the specific advantages of hippotherapy and recreational therapeutic horseback riding. In the latter, equestrian skills are the main objectives. Important issues in hippotherapy were space and time understanding/attention, and executing tasks in a particular space and time construction alone and together with other subjects or parents.
The five trained horses were owned by one of the hired instructors, who did know each particular horse. The medium-sized horses were chosen based on characteristics in gate length, and size in height and width. Those characteristics give different stimulations to the rider, but at the start the personal interaction between the child and the horse were also of importance. All the horses had medium level in dressage. The researcher selected the appropriate horse for each subject. In addition, the movements of the horses were modified during treatment sessions depending on the needs, abilities, and responses of the subjects. These rhythm variations were used with purpose and consequently, but there were also moments of tranquility and relaxation. Two (2) times they practiced horse vaulting with special tasks. Each session was carried out in a very structured way and ended with a short debriefing. Other important issues were cooperation, responsibility, sociability, and respect.
Design
The differences between the subjects were kept as small as possible to augment reliability. Other similar effect studies recommend in their discussion a more homogeneous sample. 10,12 All of the boys had the same medication treatment and fulfilled the selection criteria. To strengthen the internal validity, none of the subjects got supplementary therapies throughout the 24-week study. The only concurrent event that may have affected the results was the summer vacation between pretest 1 and pretest 2. Other factors that could have had an impact on the internal validity could be history, training effect in filling out the tests, and the occasionally delayed reporting by the teachers.
A time series quasi-experimental research design with four test dates was selected. The time interval between test dates was held constant at 8 weeks. A therapeutic horseback riding class of 60 minutes twice weekly for 8 weeks was provided between pretest 2 and post-test 1. The implementer of therapeutic horseback riding was a physical therapist with 25 years of practice experience and registered as a therapeutic riding/hippotherapy instructor (certified by the Norwegian Physiotherapist Association).
Measures
The SDQ, KindlR-HQoL, MABC, and MNFU were selected as quantitative measures for the selected outcomes.
The SDQ recorded by subjects, parents, and teachers is a brief behavioral screening questionnaire assessing mental health in children and adolescents, aged 4–16 years. 23,24 Reliability and validity were found to be satisfactory in European studies with best results for parent report.
KindlR-HQoL recorded by subjects and parents is a questionnaire measuring health-related quality of life in children and adolescents, for use in clinical populations but also with healthy children and adolescents. 25 In this study, the version for children aged 8–12 years and the proxy version for parents were used.
MABC is an age-regulated standardized clinical test to measure and assess manual skills, eye–hand coordination, and balance. 26 The version for children aged 9–10 years and 11–12 years was used. MABC is a primarily quantitative test with possibilities for qualitative evaluations.
MFNU is a clinical qualitative assessment test to screen children with motor performance problems. This test is sensitive to identify motor difficulties in children with ADHD. The version for children aged 8–11 years was used.
Testing procedure
All four test batteries were carried out on each test date. An independent trained physiotherapist administrated the MFNU and MABC. The test results were not discussed with the researcher during or after the study. The SDQ and KINDL-HQoL were administered by the researcher. The specific rules characteristic to self-reported questionnaires were followed.
Pretreatment phase
The subjects were tested at baseline pretest 1. The form teachers of the subjects were asked by an information letter to fill out the teacher version of the SDQ. Several days before pretest 2, the subjects got an invitation letter for pretest 2, inquiring about concurrent events. All subjects showed up for pretest 2. The only event reported was school vacation.
Treatment phase
The children had therapeutic horseback riding in a group, twice weekly for 8 consecutive weeks, in an enclosed area 20×40 m or outdoors in the woods. The parents were present in each session. Two hired (2) instructors were present to give commands to the subjects. They were informed in advance about the study and they were instructed in what kind of approach and tasks the researcher wanted to accomplish in accordance with the principles of therapeutic riding/hippotherapy. Thus, the researcher had his hands free to look at reactions of the subjects and give individual responses to these. Individual therapeutic horseback riding appointments were 60 minutes, but the actual amount of time on the horse varied. At the start, a lot of time was spent on caring for the horses and learning about how to manage them. The actual riding time was about 15 minutes. After a few times, the riding time increased to about 40 minutes on the horse; the rest of the time was spent on grooming horses.
The four riding tours in the woods were used as a reward for their good effort. At the first riding lesson, the parents held the horses in a line. Gradually, after two sessions, the subjects had to steer their horses themselves. They learned to ride figures and react instantly and consequently on the commands. In the beginning, they had to concentrate on their own horses, but gradually, they had to look at the other subjects and their horses to keep the same distance between them and to react together at the same moment. The parents were instructed to fulfill some exercises together with their children by specific rules. The children were asked to vary their positions on the horse: forward facing, rear facing, side facing, modified side sitting, prone, quadruped, and standing. Meanwhile, the tempo of the horses was varied from halt, walk, trot, and gallop. While riding on the horse, the subjects were encouraged to maintain postural alignment with symmetry of head, trunk, and lower and upper extremities. To keep the spirit up, once in a while the sessions were ended with simple kinds of mounted games. Rhythm variations were used with a purpose and consequently, but moments of tranquility and relaxation were part of the arrangement. The subjects had to ride occasionally without a saddle.
Post-treatment phase
Post-test 1 was carried out during the week after the final therapeutic horseback riding session. The post-test 2 was 8 weeks later. To examine confounding variables, the parents were asked to report concurrent events.
Data analysis
SPSS version 15 (SPSS Inc., Chicago, IL), was used to complete all analyses. 1. A binomial statistic method was used to quantify the general nature of the information. 2. Wilcoxon paired-sample test was used to determine the difference of the mean of pretest 2 and post-test 1. 3. Friedman test for repeated measures was used to determine the difference between the two pretests and the two post-tests. 4. The effect size (ES) was calculated as proposed by Looney and colleagues.
27
The power was calculated using GPowerR.
28
Results
The results of the different tests showed an improvement in various domains of behavior, quality of life, and motor performance of the children from pretest 2 to post-test 1. The effects according to behavior and quality of life diminished from post-test 1 to post-test 2, while the effects of both the ABC- and MFNU-test show a further improvement.
Behavior (SDQ)
The single subject scores for the 5 participants from pretest 2 and post-test 1 revealed that the behavioral patterns were ameliorated according to the parents, teacher, and the subjects (Fig. 1).
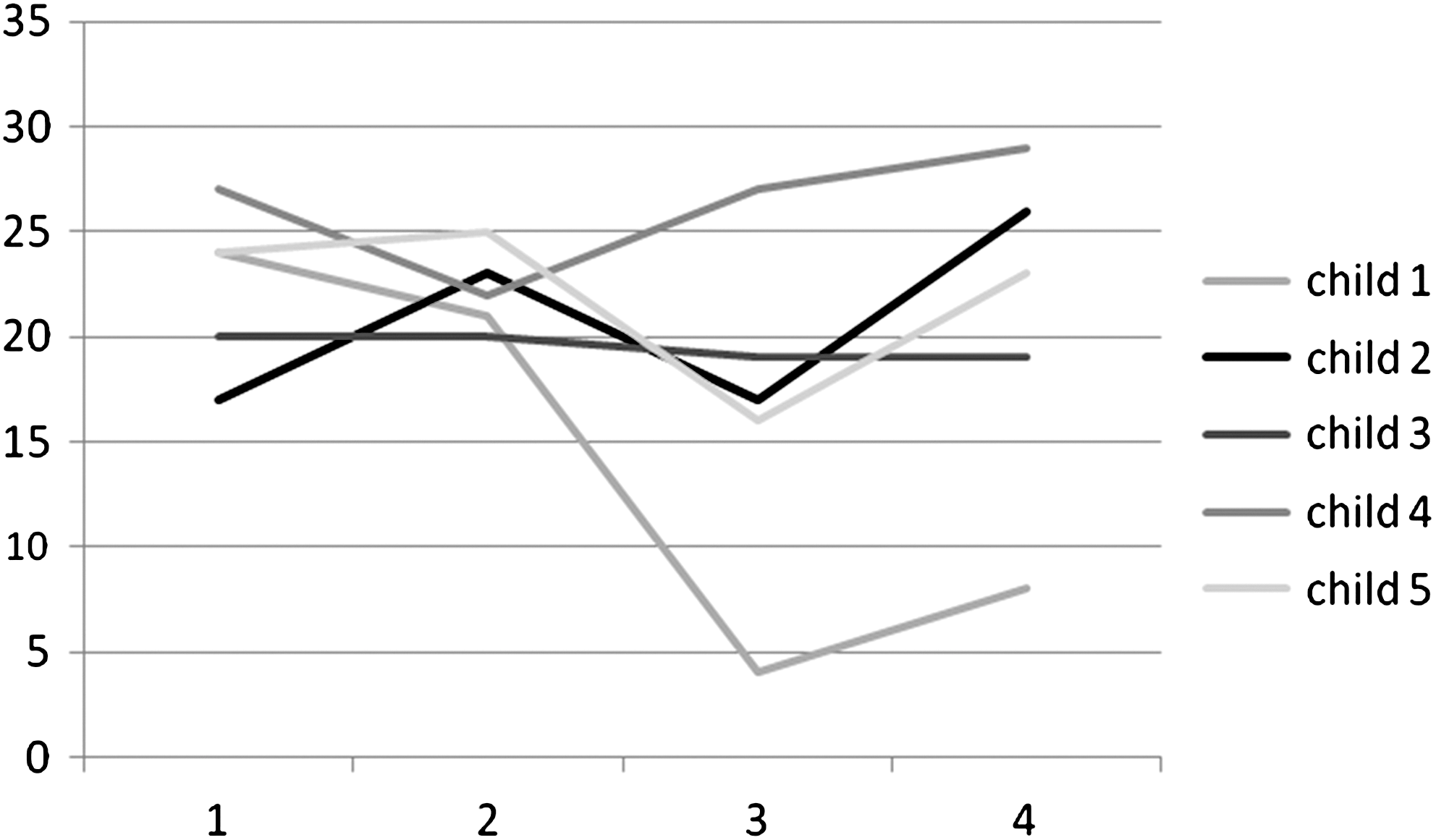
Trends of behavioral assessment values of the Strength and Difficulties Questionnaire (0–30; reported sum scores by parents) in 5 children from pretest 1 (1) to post-test 2 (4). Diminishing value means improvement.
In a clinical diagnostic perspective, using percentile norms standardized for British 11–15-year-old boys, all participants were in the 10 upper percentiles before the intervention, indicating treatment. After the intervention, it was shown that only 2 of 5 boys' behavior indicated treatment, as reported by their parents.
The mean values for the subtests were studied, and graphs of the test scores were used to depict the general nature of the information. From pretest 2 to post-test 1, the mean values of the SDQ test (parents, teacher, and the participants themselves) revealed positive changes for 15 of the 18 subtests.
The nonparametric Wilcoxon test showed a significant difference for four of the six items of the SDQ test reported by subjects (Emotional symptoms, Conduct problems, Hyperactivity/inattention, and Total difficulties). The parents reported a significant change for two of the six subtests (Hyperactivity/inattention and Total difficulties). The teachers also noted a significant positive change for Total difficulties (Fig. 2).

Means of subtest scores and mean of total score on pre- and post-tests of the Strength and Difficulty (SDQ) test, parent version. n=5. A decreasing mean value of the scores indicates a positive trend. A significant difference (p≤0.05) between the means of the subtest scores on pretest 2 and post-test 1 for domain Hyperactivity/inattention, and total score of the subtests Total difficulties.
Finally, all the data were analyzed using a Friedman test, revealing a significant positive change for behavior (Total Difficulties) between all the pre- and post-tests.
From post-test 1 to post-test 2, there is a decline of the positive effect on the behavior of the participants, but a better result can still be noted for 3 of the 5 participants in comparison to pretest 2. Just 1 of the 5 boys had a behavior that did not indicate treatment.
Quality-of-life data (HQoL)
The single-subject quality-of-life data revealed amelioration for only 2 of the 5 participants, as reported by the parents and the children (Fig. 3).
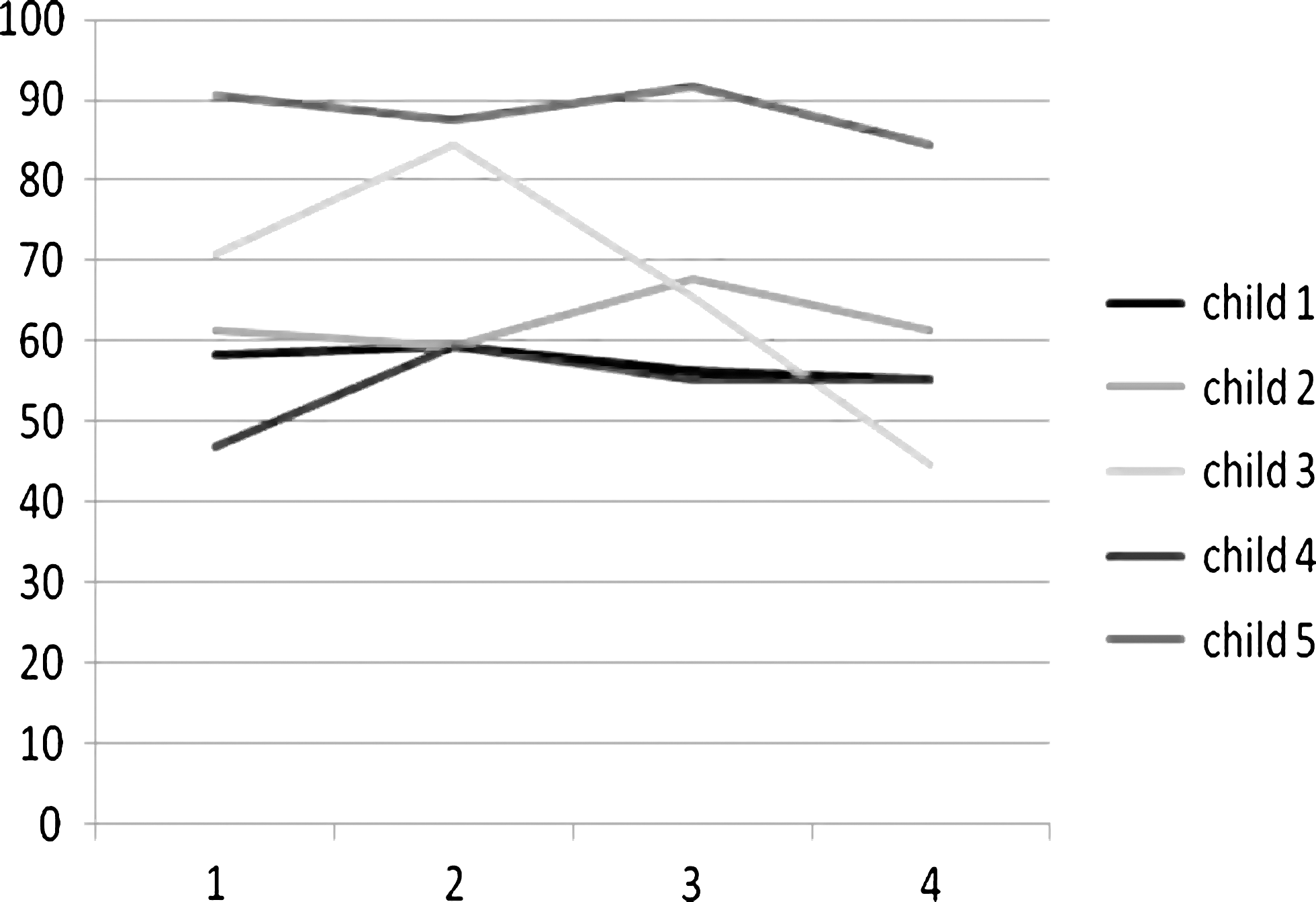
Trends of KindlR–Health-Related Quality of Life Questionnaire assessment values (0–90; reported sum scores in percent by children) in 5 children from pretest 1 (1) to post-test 2 (4). Increasing value means improvement.
In a clinical diagnostic perspective, the self-reported total scores were compared with the standardized reference values for corresponding age, gender, and health status group. Before the intervention, 3 children had a HQoL score as low as chronically ill boys. After the intervention, only 2 children assessed their HQoL as low as chronically ill boys.
Six (6) of 7 items reported by parents showed positive changes in the mean scores from pretest 2 to post-test 1. Only the item “Family” showed a negative tendency. The QoL scores reported by the subjects showed a positive trend from pretest 2 to post-test 1 for just one domain. However, when the scores from pretest 2 are excluded, with the fact they were taken after the summer vacation being a possible confounder, the scores from pretest 1 to post-test 1 showed a positive trend for 4 of 7 scores (Fig. 4).

Means of subtest scores and mean of total score on pre- and post-tests of the Kindl R–Health-Related Quality of Life test, children version. n=5. An increasing mean value of the scores indicates a positive trend. There was no significant difference (p≤0.05) between the means of the subtest scores or total score of the subtests on pretest 2 and post-test 1.
The Wilcoxon test showed that the parents reported a significant positive change for two of seven items (Psychic well-being and School). The boys themselves reported no significant positive changes at post-test 1.
The parents reported a further augmentation in the quality of life for 3 of the 5 participants from post-test 1 to post-test 2. On the other hand, just 1 child noted a further amelioration in his quality of life. For the other 4, the positive tendency declined, but the scores remained positive in comparison to pretest 2. In the QoL test, the subjects noted a positive significant change for the item “Total score” at post-test 2.
The motor performance (MABC, MFNU)
The single subject scores for motor performance were better at post-test 1 for 3 of 5 participants (Fig. 5).

Trends of motor performance assessment values (0–60; sum-score movement Assessment Battery for Children and Modified Function–Neurological Assessment in 5 children from pretest 1 (1) to post-test 2 (4). Diminishing value means improvement.
For both motor performance tests, the mean test results revealed a positive change after the intervention and the motor performance improvement became significant 2 months after the therapeutic horseback riding for 4 of 5 participants.
Table 1 presents the means, standard deviation, effect size, and power for the different domains that showed a positive significant change after the intervention. The effect size was calculated using the pretest standard deviation for repeated measure. The positive changes due to the intervention seemed to be meaningful (ES=0.21–6.30). The power varied from 0.11 to 1.
Effect Sizes (ES) and Power of the significant differences between the means (m) of the subtest scores and total score of the subtests on different test domains of behavior (Strength and Difficulties Questionnaire, SDQ), quality of life (KINDLR-HQoL), and motor performance (Movement Assessment Battery for Children, MABC; Modified Function Neurological Assessment, MFNU).
p<0.05.
ES: 0.20=small; 0.50=moderate.
Power: 0=low; 1=strong.
Discussion
The purpose of the present study was to evaluate the effect of therapeutic horseback riding on children with ADHD. The primary objective was to determine whether therapeutic horseback riding had a positive effect on behavior, health-related quality of life, and motor performance.
The results demonstrate a treatment effect on behavior and on quality of life after the intervention phase, while there was no significant change during the nontreatment phase. On the other hand, the positive change in motor performance after the intervention became significant in the post-treatment phase. This strengthens the research hypothesis and may illuminate a certain carryover effect of therapeutic horseback riding on the motor functioning in daily life, also after ending the intervention.
The secondary objective was to define in which domains of behavior—quality of life and motor performance—the positive alterations appeared. The results were studied in two different ways.
First, the tendencies of the single subject scores were studied to detect clinical changes individually by using clinical standardized reference values. Most boys achieved a better behavior, quality of life, and motor performance after the intervention, reported by the parents, teacher, and themselves.
Second, the means of the different subtests and items were analyzed to find on which levels changes appeared. The teachers, parents, and the participants reported a significant positive change for the daily life behavior. The participants themselves reported that the impact of all these behavioral difficulties was significantly diminished after the intervention. The boys also reported that the problems in the area of the emotions, conduct, and hyperactivity/inattention changed significantly. The latter was also confirmed by the parents. This is congruent with the study of Bizub and colleagues. 13 The parents also reported an amelioration of daily life quality related to the school environment. The results of the present study assume that therapeutic horseback riding may be used to support and improve the altered learning mechanism in boys with ADHD.† The parents also reported that their children had a positive change in social context, but the boys themselves experienced that the relationship with peers (SDQ) and friends (QoL) did not change positively. An explanation can be that peers may react to a sudden social behavior change, caused by an alteration in self-esteem or self-confidence. The subjects reported that their social qualifications became better directly after, but also further after ending the intervention. This finding is congruent with the studies of Tucker 15 and Macauley and Gutierrez 14 and provides better understanding of the different parts of social life and the challenges these subjects face.
A possible confounder was the school vacation between pretest 1 and pretest 2. The boys reported a relatively too large amelioration in all aspects of quality of life at pretest 2. An explanation can be that the boys were feeling better after 2 months of holidays, without the demands of daily school life. If the results of pretest 1 were compared to the results of post-test 1, the trend would have been even more positive. At post-test 1 and 2, the parents felt that the quality of life in the family situation was diminished. A possible explanation may be that the 2 months with therapeutic riding had been strenuous and that the family situation altered in regard to the interaction with the boys. They reported that the boys became more reflective on how they acted and felt in the family situation. The findings of the present study are congruent with the statement of Klassen and colleagues 29 and Antshel and Remer 30 that ADHD has a significant impact on multiple domains of the health-related quality of life in children. The present study suggests that the quality of life for these boys can be ameliorated.
The motor performance results showed a positive tendency after the intervention and became significant 2 months after ending the intervention. This may be as a result of motor learning and sensory integration 16 and its carryover effect on daily life functioning. These findings are congruent with earlier studies. 11,12 The relation between motor regulation, attention, and executive functions suggests that technologies aimed at strengthening motor planning, sequencing, timing, and rhythm may have a role in improving the capacity to attend and learn. 31 Other rhythm training 21 using vestibular stimulation established limited amelioration in motor control and attention, but there were minor carryover effects and little improvement in behavior. These latter improvements could be established using therapeutic horseback riding, where the most palpable, sociable, and three-dimensional materials are used. 32 It has to be mentioned that it was not the presence of the horse that was responsible for the positive changes, but the physical interaction and the riding on the horse might have caused the positive alterations. 22 Incongruent with the findings of Butte and colleagues, 33 it was not difficult to have the boys participate in this physical activity.
This pilot study tried to establish an estimate of the ES. The power was kept as high as possible by using strong treatments (8 weeks, twice a week), administering those treatments consistently (in relation to the riding program and instructors), and trying to use the right statistics. Nevertheless, due to the low sample size and no control group, the power was relatively low for most of the subtests. Varying the α up to 0.2 was another possibility and pertinent in a pilot study. The positive trends would have become more significant, but the type I error would have become too large.
Limitations and strengths
Although the sample was limited to only 5 children, the results show significant changes. This limitation created the possibility to study those children more extensively.
Implications for future studies
Even though a planned protocol for testing and intervention was followed, replicating this study is a challenge. Therapeutic horseback riding is a treatment strategy with multiple options. From selection of the horse, equipment, movement patterns of the horse during the treatment, and positional changes of the participant, the researcher used his knowledge and experience to choose the best combination for each individual. This study could be expanded to a multicenter trial after establishing a treatment protocol to improve control of the independent variables.
Conclusions
The use of therapeutic horseback riding could, as a result of this present study, be a viable treatment strategy as a part of a multimodal therapy for children with ADHD. The study assumes positive trends in certain domains of behavior, quality of life, and motor performance. This pilot study provides good scientific prospects for future studies to document these positive trends on larger samples.
Footnotes
Acknowledgments
The researchers wish to thank the Norwegian Foundation for Health and Rehabilitation for their financial support.
Disclosure Statement
No competing financial interests exist.
*
Larsen Stray L. Motoric function in children with AD/HD: A retrospective study of motor problems in children with AD/HD based on Modifisert Funksjonnevrologisk Undersøkelse (MNFU, modified function-neurological assessment). Master of Science dissertation, Faculty of medicine, University of Bergen, 2001.
†
Aase H. Altered reinforcement mechanisms in children with Attention-Deficit/Hyperactivity Disorder (AD/HD). Doctoral thesis, University of Oslo, 2007.