
Abstract
Objectives:
The study objectives were to examine the effects of Chinese herbal fomentation on radiocephalic arteriovenous fistula (AVF) maturation.
Methods:
All patients' preoperative evaluation, operative procedure, and follow-up information records were reviewed to identify patients undergoing radiocephalic AVF procedures for maintenance hemodialysis. All patients underwent preoperative vessel ultrasound. The ultrasound examinations were repeated every 2 months after the operative procedure. From the day after the operation, the forearm of the patient is fomented with a mixture of Dan Shen and Hong Hua in dry powdered form dissolved in fresh warm water. The fomentation lasted for 60 minutes, once a day for 28 consecutive days.
Results:
Sixty-four (64) specific access site operations were yielded in 62 patients for analysis. Forty-nine (49; 76.6%) of the 64 fistulas were considered sonographically mature and 15 (23.4%) were deemed sonographically immature. The sonographically mature fistulas (n=46) that were suitable for puncture had blood flow of 655±132 mL/minute, and venous diameter of 4.5±0.3 mm. The most frequent complication was thrombosis before first use, which accounted for 6 AVFs failures to mature (0.16 per patient-year). There were two hospitalizations for fistula-related bacteremia in the group (0.05 per patient-year).
Conclusions:
The Chinese herbal fomentation reduced the frequency of early thrombosis of new AVFs and was accompanied by an increase in the proportion of AVFs that were suitable for dialysis.
Introduction
Traditional Chinese medicine (TCM) is a system of healing that originated thousands of years ago. It has evolved into a well-developed, coherent system of medicine that uses several modalities to treat and prevent illness. The research of Bao et al. found that recipe-steeping hands with Chinese medicine can improve ecchymoma and preserve the normal hemodynamics of AVF. 4 The purpose of this study was to retrospectively examine our institution's experience of Chinese herbal fomentation across 6 years with radiocephalic AVF procedures. Outcomes for the AVF were assessed and compared in terms of time to use, maturation rates, and complication rates.
Methods
This was a retrospective analysis. Hospital review board approval was obtained for this dialysis retrospective study, with waiver of informed consent. All patients' preoperative evaluation, operative procedure, and follow-up information records from the First Affiliated Hospital to Changchun University of Chinese Medicine, from December 2002 through January 2008 were reviewed retrospectively to identify patients undergoing radiocephalic AVF procedures for maintenance hemodialysis. Information about patient demographics, comorbidities, and previous dialysis access procedures was also collected. There were no inclusion and/or exclusion criteria. The analysis screened them all. All patients underwent preoperative vessel ultrasound during their initial clinical evaluation. The ultrasound examinations were repeated every 2 months after the operative procedure. Operations were performed on an outpatient basis unless the patient was hospitalized for other reasons. All radiocephalic wrist AVFs were constructed in the wrist region by the experienced nephrologists of our unit (Shengmao Liu and Ye Jia). Local anesthesia with 1% mepivacaine was used. In all cases, anastomoses were created in an end-to-side fashion (Fig. 1). The surgery procedure and fomentation were consistent in all cases selected.
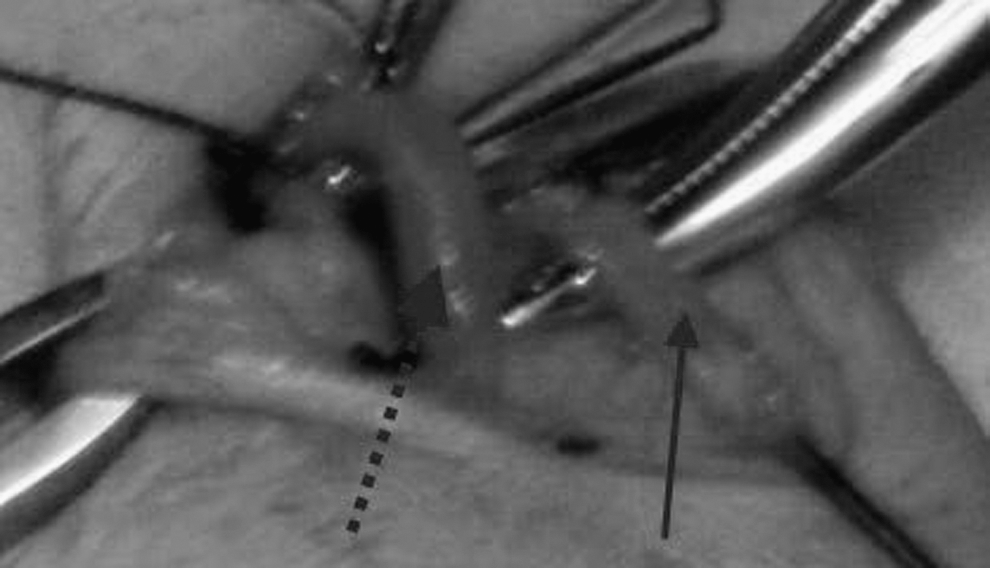
Anastomosis of radial artery with cephalic vein. Radial artery (solid arrow); cephalic vein (dotted arrow).
From the day after the operation, 2 cm away from the proximal part of suture, with the application size of 5.0×3.0 cm, the forearm of the patient was fomented with a mixture of Dan Shen (Salvia miltiorrhiza Bge.) 5 g and Hong Hua (Carthamus tinctorius L.) 5 g in dry powdered form dissolved in fresh warm water (20 mL, 35°C). The fomentation lasted for 60 minutes, once a day for 28 consecutive days (Fig. 2).

Chinese herbal fomentation 2 cm away from the proximal part of suture. Site of fomentation (solid arrow); site of suture (dotted arrow).
Ultrasonography (US) examination of the AVF was performed regularly for all patients. An overview of the AVF feeding artery, draining vein, and anastomotic region was obtained. During the examination, minimal pressure on the skin from the transducer was used to minimize vessel deformation. The largest anteroposterior diameter of the draining vein was measured in the transverse dimension. The internal diameter was measured in longitudinal section in the radial artery at the wrist and in the distal part of the forearm. The probe was aligned to show the intimal layers at the near and far walls to measure the distance from intima to intima perpendicular to the arterial wall. Blood flow measurements were obtained in the draining vein of the AVF. To decrease the possibility of encountering turbulent flow, these measurements were obtained in the middle of the forearm for a forearm AVF. All subjects underwent US vascular mapping with an HDI 5000 (Philips Ultrasound) scanner operated by registered diagnostic medical sonographers in the First Affiliated Hospital to Changchun University of Chinese Medicine.
A radiocephalic AVF at the wrist was created when basic criteria were met, as follows: (1) a normal and uninterrupted cephalic vein 2.5 mm or larger in diameter by ultrasound evaluation, and (2) a normal radial artery of 2.0 mm or larger in diameter by ultrasound examination. Right- or left-handedness was considered secondary to best available vessels in selecting the extremity for AVFs. The arteriotomy and venotomy sites were carefully chosen and aligned to guard against twisting or distortion when the anastomosis was completed.
A radiocephalic AVF at the wrist was determined to be sonographically mature when the criteria were met: (1) the minimal diameter was 4.0 mm or larger by ultrasound evaluation, (2) the blood flow access was 500 mL/min or more, and (3) the distance from the skin was no less than 5 mm. 5 If any criterion was not met, the fistula was considered sonographically immature.
The dialysis nurses attempted fistula cannulation on the basis of their clinical judgment and postoperative imaging results.
Data collection was performed at baseline and every 2 months thereafter until 6 months or ascertainment of fistula suitability.
Definitions
The principal outcome measures were maturation rate, time to first use, nonfunctional AVF, and rates of complications. Maturation was defined as successful cannulation for at least one complete hemodialysis session and an access that was able to deliver a flow rate of 350–400 mL/min without recirculation for the total duration of dialysis. Time to first use was defined as the interval between the creation of the AVF and its maturation. A nonfunctional AVF was an access that was not being successfully used for hemodialysis, regardless of whether it is patent. 6 Complications were inability to access because of thrombosis, stenosis, primary nonmaturation, and infection.
Statistical analyses
Results were shown as means±standard error of the mean unless otherwise described. Results were presented with corresponding 95% confidence intervals. Kaplan-Meier analysis was used to calculate the survival rate for AVF. Analyses were carried out using SPSS 16.0.
Results
Patient population
Sixty-nine (69) consecutive vascular access operations were performed on 67 patients at the dialysis center of the First Affiliated Hospital to Changchun University of Chinese Medicine. No grafts were used. Table 1 summarizes the demographic and clinical characteristics of patients who received a forearm access. In the 67 patients (31 men, 36 women; age range, 21–70 years; mean age, 45 years±12), 69 forearm fistulas were placed. Eighteen (18) patients had a forearm access constructed in the dominant-handed extremity. Of the population in our study, 53.7% (36 of 67) were diabetic. All patients underwent vascular mapping. The preoperative vascular mapping that was obtained prior to AVF placement showed vasculature suitable for a forearm fistula in the study population. Five (5) patients were excluded from the final access analysis as a result of death (n=3) of causes unrelated to dialysis access, revision because of steal syndrome (n=1), or change to peritoneal dialysis (n=1). Sixty-four (64) specific access site operations were yielded in 62 patients for analysis. Two (2) fistulas failed due to thrombosis and were not salvaged during the follow-up period. These 2 patients had successful AVFs created at the forearm in the other extremity. Baseline characteristics of the patients are shown in Table 1.
Cardiovascular disease was defined by a history of myocardial infarction, angina, coronary-artery angioplasty, coronary-artery bypass grafting, or congestive heart failure. Peripheral arterial disease was defined by a history of nontraumatic amputation, angioplasty or bypass surgery of the leg or foot, or claudication.
SD, standard deviation; BMI, body–mass index; ESRD, end-stage renal disease; ACE, angiotensin-converting enzyme; ARB, angiotensin-receptor blocker; RA, radial artery; CV, cephalic vein.
U.S. findings in fistulas
Forty-nine (49) (76.6%) of the 64 fistulas were considered sonographically mature and 15 (23.4%) were deemed sonographically immature. The sonographically mature fistulas (n=46) that were suitable for puncture had a blood flow of 655±132 mL/min, and a venous diameter of 4.5±0.3 mm. The blood flow was sufficient for adequate hemodialysis (Kt/V 1.26, ranging from 1.13 to 1.40 [K, dialyzer clearance of urine; t, dialysis time; V, volume of distribution of urea]). The distance from the skin was 3.2±0.5 mm. In the 15 sonographically immature fistulas, thrombosis was seen in 6 (40.0%). The cause of the other 9 (60.0%) unsuccessful fistulas was insufficient blood flow through the vein.
Access survival and frequency of access events
The mean duration of patient follow-up was 6.2 months. The clinical outcome (adequacy for dialysis) was known for 49 of 64 fistulas. Evaluation of technical success found that five AVFs were constructed in patients who had not yet started dialysis. These fistulas were determined to be technically successful. Forty-four (44) patients had native arteriovenous fistulas that were used successfully for repeated dialysis access. These 44 fistulas were initially cannulated 1.5–4 months (average, 2.2 months) after they were created, provided they were deemed adequately mature after US assessment.
The most frequent complication was thrombosis before first use, which accounted for six AVFs failures to mature (0.16 per patient-year). There were two hospitalizations for fistula-related bacteremia in the group (0.05 per patient-year). There were no deaths related to access-related infections in the study population. In 2 patients, the AVFs were patent but not dilated sufficiently for use in hemodialysis.
Maturation rate, and rate of complications at 2, 4, and 6 months are shown in Table 2 and Figure 3. The maturation rate for all AVFs was approximately 75% at 6-month follow-up.
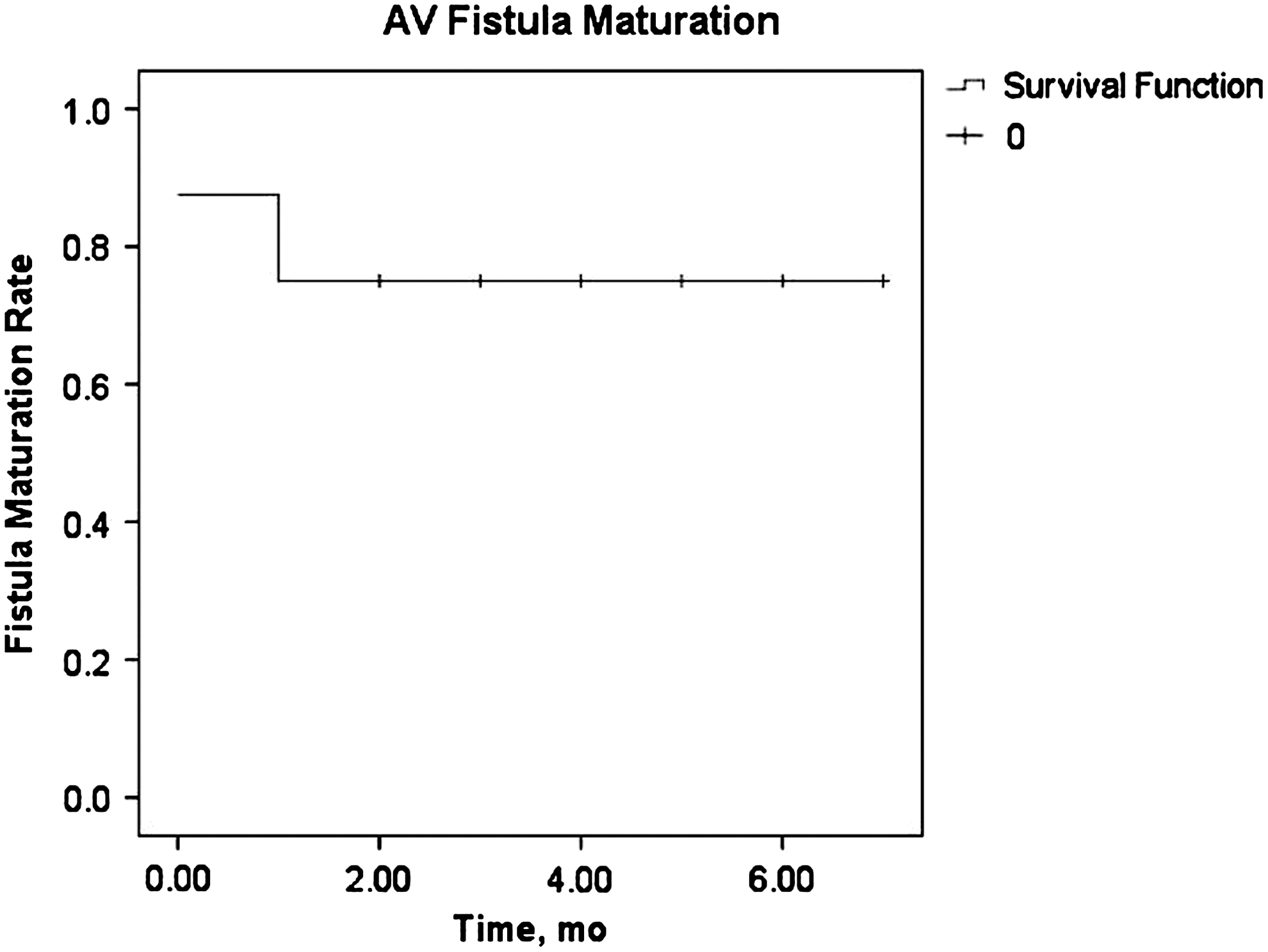
Kaplan-Meier survival analysis of the maturation rate for all arteriovenous (AV) fistulas.
AVF, arteriovenous fistula; mo, months.
Discussion
AVFs are the preferred hemodialysis vascular access because they have greater longevity and less frequent infections. 1 Radiocephalic AVFs are the primary shunts created for patients chronically undergoing hemodialysis in most hemodialysis centers in China. Vascular access complications account for 16%–25% of hospital admissions. 7 A significant number of AVFs (28%–53%) never mature adequately to support dialysis therapy. 8 –11 The mechanisms of AVF dysfunction are complex. Usually, an AVF is not used until 3 months after placement. Nephrologists often wait up to 6 months before declaring the fistula a failure. 12,13
Ultrasound examination has become a key element in preparation for dialysis access surgery. 14 –18 Patients in this report were evaluated preoperatively with ultrasound during their initial visit. This direct observation of the vascular anatomy was critical in selecting the best site and strategy for creating a successful AVF. Most patients are not suitable candidates for a radiocephalic AVF at the wrist, as determined by ultrasound evaluation. 11,19,20 Often, the cephalic vein at the wrist has been utilized for venipuncture and intravenous therapy access sites. The vein may be too small. Second, the draining vein may be located too deep within the subcutaneous tissues to allow safe cannulation. In addition, the radial artery at the wrist may be inadequate for a direct anastomosis. 21 Frequently, one extremity may offer good access opportunity after ultrasound examination of the opposite arm was not promising. With the early detection of these underlying anatomic problems, an immature fistula may be converted into a fistula that can be used for dialysis.
The draining vein needs to be of a certain size not only for successful cannulation but also for carrying adequate blood flow. The measurement of blood flow is recommended as the preferred method of surveillance for AVF. 22 Blood flow rate has been measured to be at least 350–500 mL/min in normally functioning AVFs. 23 Lin et al. 24 found a mean blood flow rate of 634 mL/min in 152 patients with successful AVFs. Mean blood flow rate in successful AVFs was reported by Wong et al. 25 to be approximately 650 mL/min at 12 weeks. In our study, the sonographically mature AVFs had a blood flow of 655±132 mL/min, which was sufficient for adequate hemodialysis.
In the herbal fomentation, both Dan Shen and Hong Hua have an inhibitory effect on thrombus formation. 26 –28 The thrombosis rate at 0.16 per patient-year at risk was well below current outcome goals (0.25 per patient-year). 29 The Chinese herbal fomentation reduced the frequency of early thrombosis of new AVFs and was accompanied by an increase in the proportion of AVFs that were suitable for dialysis.
The occurrence of adverse events in the study was rare. The reasons for 5 patients being excluded from the access analysis were due to causes unrelated to dialysis access. The occurrence of fistula-related bacteremia for hospitalizations was 0.05 per patient-year. This observational study cannot directly address the mechanisms by which early fistula maturation may be related to a lower risk of adverse events. Several potential mechanisms, however, have been proposed. Matured AVFs provide a higher blood flow rate; therefore, a higher dialysis dose may be achieved. 30 The lower rate of access-related complications may result in longer dialysis sessions. 31 This again may lead to a higher dialysis dose, less frequent hospital admissions, and other untoward effects. 32
The fomentation was well tolerated and did not increase bleeding events during the study period. Preoperative ultrasound examination avoided the development of stenosis of the draining vein and poor arterial inflow. All of these increased the probability of successful fistula maturation.
Chinese herbal fomentation offers other advantages. It is a noninvasive intervention that presents very few adverse side-effects and contraindications compared with other pharmacologic interventions. It is rapid to administer and is convenient for community-based settings.
This research also has some limitations. AVFs are preferred because of superior long-term patency. Follow-up time in our study was limited to 6 months. Extra follow-up time is required to obtain further insight into long-term AVF patency. There is no control group, so the results have some limitation. This study is also limited in its ability to detect significant predictors of nonfunctional AVF as a result of the small number (n=2).
Conclusions
In conclusion, Chinese herbal fomentation increases the proportion of AVFs maturation. This retrospective study provides evidence that Chinese herbal fomentation, a form of alternative medicine, is clinically useful for the maturation of AVFs.
Footnotes
Acknowledgments
Zhibin Cong, Wei Yan, and Yang Song (Department of Radiology, the First Affiliated Hospital to Changchun University of Chinese Medicine) are gratefully acknowledged for excellent work on database setup and maintenance.
Disclosure Statement
No competing financial interests exist.