
Abstract
Objectives:
The objective of this study was to test a model of placebo effects in the context of a general model of health care outcomes.
Design:
The design of this study was a multisite, double-blind, placebo-controlled crossover trial.
Settings:
The study was conducted at The University of Washington Hospital, Seattle, Washington, Cooper Hospital/University Medical Center, Camden, New Jersey, and at the Neurology Center of Fairfax, Fairfax, Virginia.
Subjects:
One hundred and seventeen (117) patients diagnosed with Multiple Sclerosis were enrolled in the study.
Intervention:
Subjects had daily exposure to a pulsing electromagnetic generator.
Outcome measures:
The outcome measures were the average score of three quality-of-life indices: the Modified Fatigue Impact Scale, the Medical Outcomes Study Pain Effects Scale, and the Spasticity Effects Scale.
Results:
Placebo responders scored higher in the personality trait of Absorption compared with nonresponders (p<0.01). Placebo responders were more confident that the sham device was active compared to placebo nonresponders (p<0.009). The two factors of confidence in the treatment and Absorption accurately identified 80% of placebo responders in a discriminant analysis (p<0.0004).
Conclusions:
Placebo effects are best understood when integrated in a general model of health care outcomes.
Introduction
A recent Newsweek article described the “drumbeat of studies on the therapeutic power of placebos” and focused on the mixed feeling people have about these effects. 6 The author compared placebos to the magic feather of Dumbo the flying elephant. Dumbo believed the feather would keep him airborne but he eventually discovered those powers were actually under his control, when he accidentally dropped the flying placebo. Apparently many people react with outrage when studies suggest they may have been paying for expensive magic feathers instead of effective medications and surgeries. Why are people not more pleased with placebos and take them as evidence of innate healing capacities?
It is proposed that the integration of a scientific model of placebo effects within a general model of health care outcomes could finally end the placebo debate and help to integrate these powerful effects into the health care system. Conceptually, the model rests on the understanding of the importance of a person (individual difference) and situation (expectation) interaction. Each factor has a long history in the study of placebo responding. However, it is proposed that the situation-specific interaction of the two factors is essential for understanding placebo responding and the reliable prediction of the effect.
Positive expectancy is recognized as a central component of placebo phenomena by all placebo theorists. 7,8 However, the same cannot be said for individual differences. The search for a placebo personality factor was the focus of decades of placebo research, but this effort was largely abandoned because of inconsistent results. 9 The widespread conclusion that there is no reliable individual difference factor at work in placebo responding has been a major stumbling block for placebo theorists for decades. This research question has been plagued by inconsistent results over the years, with evidence found for an individual difference factor in one research setting and then not another. Even though researchers have been frustrated in the search for a single factor that would reliably identify placebo responders across settings, the question of whether “placebo responders” exist continues to be raised and remains a question for placebo theorists to this day. 10
The proposed model emphasizes that the search for a placebo personality factor must be combined with the measurement of situational expectancy. It is necessary to consider treatment expectation, which varies considerably based on a host of situational and person-historical factors. In fact, according to the model, an individual who has negative expectations regarding treatment effectiveness would likely produce a stronger than average “nocebo” effect, washing out individual differences if both factors were not jointly taken into consideration. 11 A central feature of the model is that it predicts the difficulty in identifying “placebo responders” consistently across clinical trials. A placebo-prone personality will only manifest a placebo effect in the presence of positive beliefs, and these naturally vary from one situation to another.
The personality trait of Absorption has been found to be consistently correlated with hypnotizability, but it is a broader construct, measuring openness and receptivity to sensory experiences and a propensity for sustained, focused attention. 12 The Absorption Scale is a subscale of the Multi-Dimensional Personality Questionnaire 13 and is correlated with the Openness factor of the NEO (Neuroticism, Extraversion, Openness) Personality Inventory. Studies show that Absorption has a genetic basis and is higher in women compared to men, and higher in children compared to adults. 14 High Absorption scorers possess natural trance abilities and can produce a variety of physiologic changes in laboratory settings. 15 Thus, high Absorption scorers have enhanced self-regulation capacities that might be engaged toward a therapeutic outcome. However, as Tellegen has described, the effects of high Absorption can go in either a positive or negative direction, depending on the situation, and this interaction may be manifest in the complexities of placebo phenomena.
This study was designed to test a model of placebo response in a clinical trial of a pulsing magnet for the treatment of multiple sclerosis (MS). The results of the trial indicate that the active device was more effective than the sham; participants using the active device reported reduced fatigue (p=0.04) and improved overall quality of life (p=0.03), while no treatment effects for bladder control or disability were shown. Results for spasticity were mixed. 16 As in many clinical trials, some participants reported significant clinical improvement while receiving sham treatment: the so-called “placebo effect.” The participants' confidence in the treatment and the personality trait of Absorption were measured to evaluate a two-factor model of placebo effects, as a special case of a general model of health care outcomes.
Materials and Methods
Design
This study was conducted in the context of a randomized, double-blind, placebo-controlled, crossover trial. The study lasted 10 weeks, with two 4-week treatment sessions separated by a 2-week washout period. Symptom surveys were administered prior to treatment as a baseline measure and immediately following the two treatments sessions. Paired t tests were used to compare changes from baseline symptom severity during the active and placebo treatment sessions.
Subjects
Three (3) research sites (The University of Washington Medical Center, the Neurology Center of Fairfax, VA, and the Multiple Sclerosis Association of American, Cherry Hill, NJ) recruited subjects through flyers, mailing, lists, and word of mouth, and enrolled 145 subjects, with 117 subjects completing the study. Participants who failed to complete the study most often stopped due to medical problems or conflicting treatments for their MS. Psychologic data were available on 110 subjects who contributed to the placebo analysis; 78% were female and 22% were male, with an age range of 21–64. Details on subject recruitment, eligibility criteria, attrition, disease stage, and medications are given in the clinical trial report. 16
Procedure
Subjects were randomly assigned to the “treatment first” or “placebo first” condition upon arrival to the first treatment session. The device used to generate the electromagnetic pulse, which cannot be felt, was worn next to the skin. Placebo devices were identical to the magnetic ones, with the exception that the inside coil had been disconnected so that no pulse could be generated. Details on specifications of pulsing magnetic and placebo devices, as well as instructions to patients on use of the device, are given in the trial report. 16
Measures
The outcome measures used to classify participants as treatment and placebo responders was a composite measure based on three scales of the MS Quality of Life Inventory (MSQLI). The MSQLI was developed and validated by the Consortium of Multiple Sclerosis Centers Health Services Research Subcommittee. It is a comprehensive assessment battery designed to be used in clinical trials and includes scales measuring fatigue, pain, and spasticity. The overall quality of life index (3 QLI) is an average of fatigue, spasticity, and pain scales.
The Tellegen Absorption Scale is a 34 true/false-item subscale of the Multidimensional Personality Questionnaire.
The Positive and Negative Affect Scale (PANAS) is a 20-item scale comprising 10 positive adjectives interspersed with 10 negative adjectives. Each item is rated on a 1–5-point scale. Internal consistency (coefficient α) is reported at .88 for the Positive Affect Scale and .87 for the negative Affect Scale, with factorial and external validity for these scales also demonstrated.
Confidence ratings of placebo versus active device
Subjects were asked to say which device they thought they had been on during the last 4 weeks, at the end of the crossover trial, and to give a confidence rating on a scale of 0–10, with 0 meaning “not at all confident” and 10=“extremely confident.” Judgment that the placebo was the active device resulted in a positive score with a magnitude of the confidence rating. Conversely, if judgment was that the placebo was the placebo device, the confidence rating of the placebo was a negative score, with the magnitude of the rating.
Results
Sample
Of the 145 participants enrolled in the clinical trial, 117 completed the study. A detailed account of the sample is given in the clinical trial report. 16 Psychologic data were obtained from 110 participants—90 females and 20 males. Participants ranged in age from 21 to 64, with an average age of 46.
Categorization of placebo responders
Participants were categorized as placebo responders if they scored in the upper quintile on improved quality of life, as measured by the 3 QLI (an average of three symptom scales measuring pain, fatigue, and spasticity) after receiving treatment with a sham device. Twenty-two (22) of the 110 participants were classified as placebo responders, scoring .68 or higher on the 3 QLI difference scores. Eighty-eight (88) of the 110 participants were classified as placebo nonresponders. Using the same criterion, 50% of the participants responded to the active treatment (n=55), and these are termed treatment responders.
Placebo responders and placebo nonresponders
Placebo responders were compared to placebo nonresponders on measures of Absorption, Negative Affect, Positive Affect, and confidence ratings using a repeated-measures analysis of variance (SAS 6.11). Placebo responders scored higher on Absorption, with a mean of 19.4 (standard deviation [SD]=6.7) compared to the placebo nonresponders mean of 14.9 (SD=7.2), (F=6.33, p<0.01). Placebo responders gave higher confidence ratings that the placebo was the active device with a mean of 3.15 (SD=6.7) compared to a mean rating of .84 (SD=5.8) by participants who did not respond to placebo (F=7.22, p<0.009). Differences in Negative Affect (PANAS) were marginally significant, with placebo responders reporting a mean of 23.2 (SD=9.2) and nonresponders a mean of 19.5 (SD=7.5, F=3.58, p<0.06). There was no difference between the groups in Positive Affect.
Treatment responders and nonresponders
A similar analysis was done comparing treatment responders to nonresponders. There were no significant differences between these groups on Absorption, confidence in the treatment, or the PANAS. Figure 1 compares Absorption scores of placebo responders and treatment responders across the distribution of symptom improvement. The trend of an increasing contribution of Absorption with symptom improvement is evident in the treatment responders and significantly so in the placebo responders.
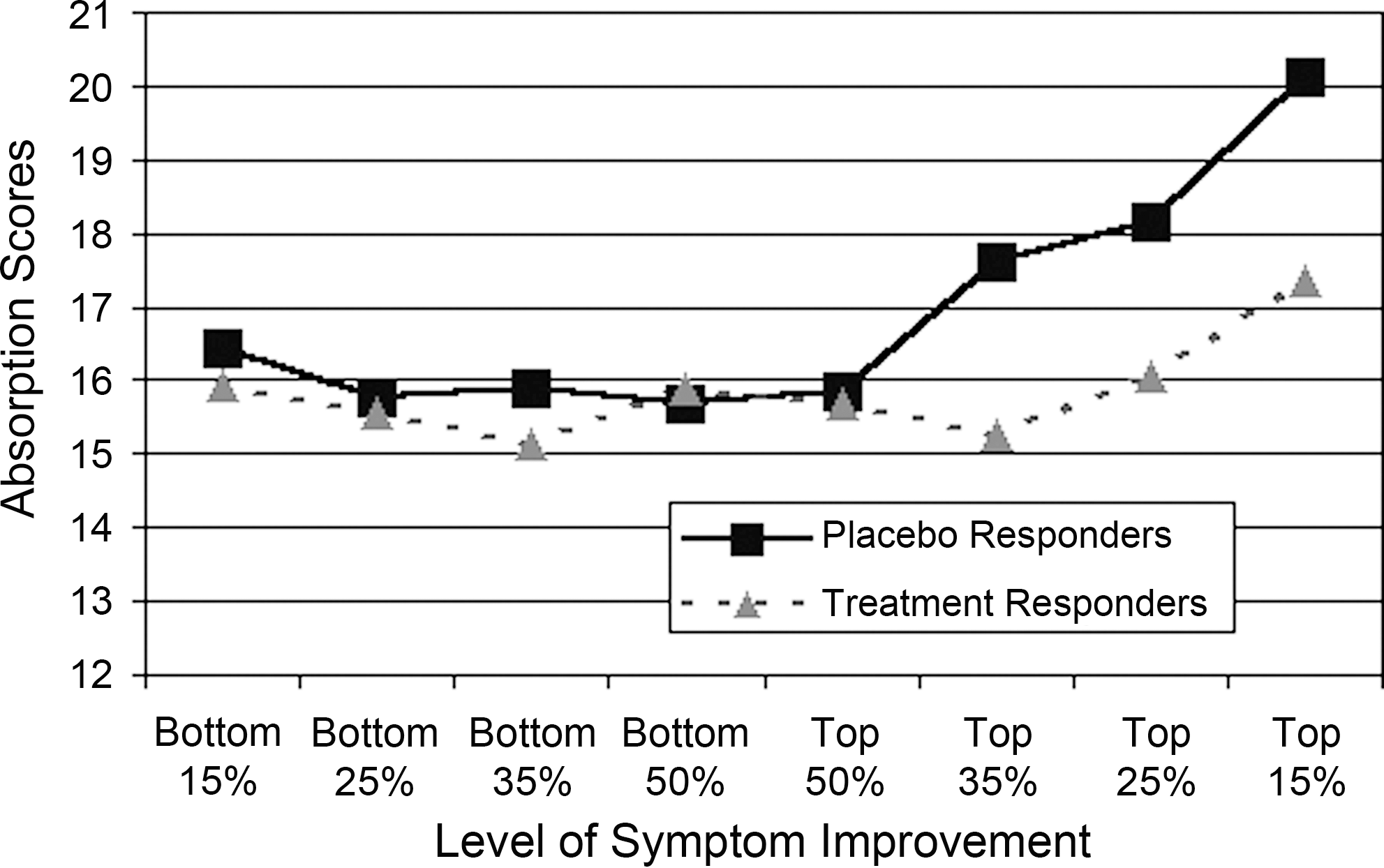
Absorption scores of placebo responders and treatment responders at increasing levels of symptom improvement (n=16–56).
Discriminant analysis
Absorption scores and confidence ratings that the placebo was the active treatment were used to classify patients as placebo responders and nonresponders in a discriminant analysis. The multivariate F [2,99]=8.45, p<0.0004, with 80% of the placebo responders correctly classified and 72% of the nonresponders correctly classified. The addition of negative affect scores to the discriminant analysis did not add to the correct identification of placebo responders. All analyses were conducted using SAS Version 6.11.
Discussion
This study provides support for a two-factor model of placebo responding. As expected, placebo responders were more confident that the sham treatment was the active device compared to the nonresponders. A recent review of the placebo response focused on the importance of positive expectancy and suggested that both cognitive and emotional factors mediate these effects. Positive beliefs or confidence in the treatment coupled with a desire to feel better activate processes that result in positive outcomes. 7 As stated earlier, the consensus among placebo theorists leaves no doubt that positive expectancy is an essential factor in understanding placebo effects.
Recent studies of the disease-specific pathways that are activated by positive expectancies have helped to transform this “soft” psychologic factor into a “hard” physiologic factor with physically measurable effects. For example, in Parkinson's disease, “expectation-induced release of dopamine in the striatum and changes of firing patterns of subthalamic nucleus neurons” is contrasted with “expectation-induced activation of endogenous opioids and cholecystokinin” in pain control studies. 5 This review ended with a question for future directions: the unresolved issue of why some people respond to placebos whereas others do not.
In this study, placebo responders scored higher on the Absorption Scale compared to placebo nonresponders. The interpretation of this factor deserves a fresh look as it may be colored by biases from the past about the nature of this individual difference. Numerous research studies have reliably shown that Absorption is modestly (yet very consistently) correlated with hypnotizability. Hypnotizability is often associated with “suggestibility,” with perhaps the sense of a weak-willed character or unbridled fantasy-proneness, the “unreality factor” that has plagued placebo theory for decades. It may be more enlightening to view these individual differences as a natural endowment in self-regulation skills: a potential innate strength rather than a simple weakness with a natural ability for self-directed healing in response to health challenges. Decades of research have reliably demonstrated that individuals scoring high in Absorption can skillfully modulate an impressive array of physiologic processes in laboratory settings. Compared to low Absorption controls, high Absorption scorers can quickly and significantly change muscle tension (as measured by electromyography), hand temperature, blood pressure, heart rate, immune parameters such as Immunoglobulin A, auditory evoked potentials, regional cerebral blood flow, R-III nociceptive reflex, and inflammatory responses. 14 Figure 1 illustrates a trend for higher Absorption scores in treatment responders as well as placebo responders. The graph draws attention to the likely contribution of person factors in both treatment and placebo healing and the appropriateness of an integrated model for therapeutic outcomes rather than a placebo model per se.
The literature suggests that the mind–body control of high Absorption scorers is similar to the self-regulation skills that many are seeking to develop with meditation, mindfulness, yoga, and qigong. The ability to still the mind and sustain focused attention, coupled with positive intention could modulate physiologic pathways at the heart of placebo phenomena and mind–body therapies. The regular practice of mind–body control and the cultivation of positive attitudes may enhance regulation at higher levels, improving the regularity of circadian and other rhythms, thus promoting greater balance of a large array of regulatory substances.
Benedetti has described placebo phenomena as activating an “endogenous pharmacy” and points to the role of both expectation and conditioning, with conditioning playing a greater role in certain pathways such as immune modulation. 5 The connection between Absorption and enhanced conditioning effects has been well described by Wickramasekera. 17 His “high-risk” model focuses on the somatic vulnerability of high Absorption individuals who suffer from negative biases in perception. 18 Wickramasekera's clinical model is more directly illustrative of the nocebo effect, defined as “a phenomenon that is opposite to the placebo effect whereby expectation of a negative outcome leads to the worsening of a symptom.” 11 It may prove fruitful to further study how high Absorption might specifically amplify the conditioning effects proposed to mediate placebo phenomena. As an example, Challis and Stam found that high Absorption was associated with anticipatory nausea and vomiting in patients with cancer undergoing chemotherapy, significantly contributing to the conditioning model in predicting which patients would develop these effects. 19 As has been learned from the conditioning literature, effective cues for triggering placebo responding would be expected to be salient and repeated features of the therapeutic setting associated with positive expectancy. The nocebo phenomena described by these researchers are important for our model as they directly illustrate the power of a negative interaction of the two factors.
Many health care practitioners and researchers have made the case that placebo effects should be recognized as powerful therapeutic effects and incorporated into clinical practice to achieve maximum therapeutic effect. 20 –25 Many physicians admit to prescribing placebos to contribute to patient wellness, even though this “dark secret” is not condoned and is considered to be ethically questionable. This ethical dilemma can be resolved by a more direct approach. High Absorption individuals may benefit from encouragement to utilize their innate self-regulation skills toward maximum therapeutic effect. Persons with average Absorption scores can be encouraged to become more skilled at self-regulation through mind–body therapies. Wickramasekera's treatment model begins with biofeedback to cultivate mind–body awareness and direct experience (mindfulness) of the shift from a negative to a positive mental attitude. The similarity of this clinical model to the proposed placebo model illustrates the generality of a two-factor mind–body model for health care.
Limitations of the proposed model
The simplicity of the model might be considered a limitation. The model does not specifically address the many factors that contribute to confidence in the treatment, such as cost, pill color, pill size, or confidence-enhancing paraphernalia. The role of provider and patient interaction are also not specifically addressed. While it is true that confidence in the treatment may be driven by a host of situational treatment factors, these potentially numerous and powerful effects are simply represented in the model under a “bottom-line” expectancy factor.
The model also does not directly address the role of stress reduction. The transforming of negative affect (stress) into positive beliefs and feelings (hope) may be at the heart of placebo processes, and the degree of this change may contribute substantially to the overall magnitude of the effect. The strength of placebo responding in domains such as pain and depression clearly indicate the importance of the shift from a negative to a positive state. Price's recent review of placebo theory describes the negative to positive shift in placebo responding in basic motivational terms. The desire to avoid pain transforms to the desire to feel good (pleasure), driven by the belief in imminent improvement. This constitutes a major motivational shift with important psychologic and physiologic effects. In this study, negative affect was high in the placebo responders (with marginal statistical significance), but negative affect did not independently contribute to the classification of placebo-responders. Negative affect was also high in people at the bottom of the placebo response distribution, those who did not believe that sham treatment was the active device. While the shift from negative to positive affect may be the hallmark of placebo responding, negative affect alone is not sufficient and can play a role in people who worsen as well (nocebo effects). However, the importance of the motivational shift from a negative to a positive state for a theory of placebo should not be ignored and could be measured in future studies to further explicate the model. The basic two-factor model can be further tested with the basic measurement tools of expectancy and Absorption, and the simplicity of this assessment is important for ease of data collection in clinical settings.
Conclusions
This model has the potential for the prediction of placebo responders and providing statistical control of placebo effects, a goal that motivated the early decades of placebo research. More importantly, the recognition that positive expectancy and expert self-regulation skills significantly contribute to health outcomes can help to integrate these powerful effects into the health care system. This movement is well under way as studies continue to support the efficacy of self-regulation skills, such as mindfulness meditation and yoga. The “positive psychology” movement is shifting attention to the power of positive expectation and increased awareness of the undermining nature of negative expectancy and pessimistic language, especially in vulnerable populations such as those with pain and depression, both known for high placebo effects. Practitioners of the art of health care have always recognized the importance of motivated and empowered patients and the power of a kind word and a ray of hope. This is the time to quantify these factors, integrating art and science, and finally solving (and forgiving Descartes for) the mind–body problem.
Footnotes
Acknowledgments
This study was conducted with partial support from grant award 5 U24 DE 11924 funded by the National Center for Complementary and Alternative Medicine and the National Institute of Dental Research of the U.S. National Institutes of Health and by a grant from the Multiple Sclerosis Foundation. We gratefully acknowledge the contributions of Martha Lappin, PhD, Fraser Lawrie, MS, Todd L. Richards, PhD, and Eric Kraemer, MD in the collection of additional data in their multisite clinical trial.
Disclosure Statement
No competing financial interests exist.