
Abstract
Background:
Individuals with prehypertension are at risk of hypertension and cardiovascular diseases, and yet efficient interventions are lagging behind. Studies indicate that heart rate variability–biofeedback (HRV-BF) increases HRV and baroreflex sensitivity (BRS) as well as reduces related pathological symptoms, suggesting potentially beneficial effects of HRV-BF on prehypertension, but little is known about these effects. In this study, these effects were investigated and their mechanisms were explored.
Objectives:
The effect of HRV-BF on prehypertension in young adults and its potential mechanism were explored.
Design:
Forty-three (43) individuals with prehypertension were recruited and classified into three categories: HRV-BF group, slow abdominal breathing group, and control group. All groups were assessed with measurements of noninvasive blood pressure (BP), BRS, respiration, and galvanic skin response (GSR) at pre-intervention, in the entire process of each session, at postintervention, as well as at a 3-month follow-up.
Interventions:
Subjects participated in a 10-session HRV-BF protocol or simple slow abdominal breathing protocol conducted over 5 weeks. A 3-month follow-up was also performed on these individuals.
Results:
The incidence of prehypertension was as high as 14.5% in young college students. Individuals with prehypertension were lower in BRS (7.5±5.2 ms/mm Hg) and HRV (log(10)-transformed of the standard deviation of normal-to-normal beats [SDNN]=1.62±0.13 ms, lgTotal power of spectral density in the range of frequencies between 0 and 0.4Hz (TP)=8.02±0.55 ms2) than those with normal blood pressure (BRS=18.4±7.4 ms/mm Hg, lgSDNN=1.79±0.10 ms, lgTP=8.68±0.85 ms2). HRV–BF reduced blood pressure (from 131.7±8.7/79.3±4.7 mm Hg to 118.9±7.3 mm Hg/71.9±4.9 mm Hg, p<0.01), increased BRS (from 7.0±5.9 ms/mm Hg to 15.8±5.3 ms/mm Hg, p<0.01) and increased HRV (lgSDNN from 1.61±0.11 to 1.75±0.05 ms, and lgTP from 8.07±0.54 to 9.08±0.41 ms2, p<0.01). These effects were more obvious than those of the slow-breathing group, and remained for at least 3 months. HRV-BF also significantly increased vagus-associated HRV indices and decreased GSR (indices of sympathetic tone).
Conclusions:
These effects suggest that HRV-BF, a novel behavioral neurocardiac intervention, could enhance BRS, improve the cardiac autonomic tone, and facilitate BP adjustment for individuals with prehypertension.
Introduction
The JNC-7 report has recommended the adoption of healthy lifestyles to treatment and prevention of prehypertension, but amelioration of prehypertension by lifestyle modifications can often be unreliable. 11 Drug therapy for prehypertension is not yet recommended, except for individuals with diabetes, chronic kidney diseases, and perhaps existing coronary artery diseases. 12 Biofeedback, a nonpharmacological intervention, is presumably an effective method for the treatment of hypertension, 13 but little is known about its effects on prehypertension. In this regard, our laboratory provided the evidence that electromyographic biofeedback could lower BP in individuals with prehypertension. 14
Heart rate variability–biofeedback (HRV-BF), also known as respiratory sinus arrhythmia (RSA) biofeedback, involves the lowering of the breathing rate to the frequency at which the amplitude of HRV is maximized. This frequency is called resonant frequency (RF). Vaschillo et al. 15 have found that breathing at one's RF stimulates the baroreceptor, producing a high amplitude of HR due to resonance characteristics of the cardiovascular system. This method is promising for treating a variety of abnormalities characterized by autonomic nervous system dysfunction, including asthma, post-traumatic stress disorder, fibromyalgia, heart failure, and depression. 16 –20 Several studies have proven that patients with essential hypertension, even at an early stage, displayed a decrease in HRV, an increase in sympathetic activity, and a reduction in parasympathetic activity of the autonomic nervous system. 21,22 Zingerman's research suggested 23 that HRV-BF could increase HRV and decrease BP in patients with hypertension. Another study in 2003 demonstrated that, 3 months after HRV-BF, the treatment group exhibited a mean adjusted reduction of 10.6 mm Hg in systolic BP (SBP) and of 6.3 mm Hg in diastolic BP (DBP). 24 However, aside from these studies, little is known about HRV-BF for the treatment of hypertension, especially for prehypertension. Therefore, this study planned to assess the effect of HRV-BF on prehypertension, and to compare the efficacy of HRV-BF with that of simple slow breathing at 6 cycles/min on the decrease of BP. It was expected that HRV-BF should have greater modulatory effects than simple paced breathing at 6 cycles/min. It was also planned to investigate the effects of HRV-BF on autonomic modulation and BRS, and to provide new research data to elucidate the mechanism by which HRV-BF regulates BP.
Methods
Subjects
First, the baseline characteristics of 45 asymptomatic subjects with prehypertension were compared with 44 normotensive persons who are sophomores in Zhongshan School of Medicine, Sun Yet-sen University (mean age: 22.3 years). All subjects signed an informed consent form before the study enrollment. Forty-three (43) prehypertensive volunteers were randomly assigned to a HRV-BF group (n=18), a slow abdominal breathing (SAB) group (n=15), and a control group (n=10), according to the random digits table. There were no statistical differences in age and body–mass index between these three groups. All subjects with prehypertension were recommended for lifestyle modification according to the report of JNC-7.
Measurement of physiologic variables
zA Spirit Nexus-16B (Netherlands Spirit-Ming) and its software (Biotrace+ version 1.20, Mind media B.V. Netherlands) were used for physiologic data acquisition, processing, and application of HRV-BF. Galvanic skin response (GSR) was measured by the skin's conductance between two small metal electrodes placed on the walls of the index finger tip and the ring finger tip, and it had been measured in μSiemens. Respiration (RSP) was recorded by strain gauges placed around the abdomen. Blood oxygen level in the extremities was measured with photoplethysmography by employing a pulse oximetry (SpO2) sensor. BP was measured at the brachial artery of left arm using an electronic blood pressure monitor with an inflatable cuff, repeated three times at each site, and averaged. BRS was measured by a passive head-up tilt. 25 –27 The heart rate and the interbeat interval (IBI) data were derived from the blood volume pulse sensor. HRV, assessed in the frequency domain, was computed by fast Fourier transforms on the IBI data.
In order to eliminate the impact of changes of BP, HRV, GSR, and other anthropometric indices at different times of the day, subjects were examined at the same time on the day of the study. All tests were carried out at sea level at 21°C and with 60% relative humidity.
Protocols
Subjects participated in a 10-session HRV-BF protocol conducted over 5 weeks. Details of the procedure for HRV-BF have been described elsewhere. 15 Briefly, in the first session, participants were asked to breathe abdominally for 2 minutes at each of five specific frequencies (6.5, 6.0, 5.5, 5.0, and 4.5 cycles/min, respectively) in order to determine individual RF. The “pacing stimulus” was provided for this purpose: a light display that moved up and down on the computer screen at the target respiratory rate. Participants were instructed to breathe at the rate indicated by the stimulus. The particular frequency with the highest amplitude of low-frequency heart rate oscillations was considered to be an individual's RF.
In the subsequent sessions, individuals were directly given biofeedback for cardiac variability, and were instructed to increase the amplitude of heart rate fluctuation that occurred in conjunction. The feedback took several forms, one of which used a beat-to-beat cardiotachometer, superimposed on a measure of respiratory activity. Participants were instructed to breathe approximately in phase with heart rate changes and make the heart rate go up as far as possible and down as far as possible with the goal of maximally increasing the amplitude of HRV. In another form, participants were displayed a dynamic power spectrum analysis of heart rate, within the band of 0.005–0.4 Hz. The display was updated approximately every second. Participants were instructed to increase the power spectrum peak that occurred at approximately RF.
The exact RF differs from person to person and also can change over time within an individual, and therefore, the precise RF had to be determined before biofeedback training was executed in subsequent sessions. If there were any changes of RF, participants were instructed to breathe at this new resonant frequency in the biofeedback training sessions and home practices. Throughout the sessions, participants were instructed to practice breathing at his or her own RF at home for a 20-minute period twice a day using a respiratory audio guide.
Subjects in the SAB group and active control group received the same duration and frequency of the protocols as those in the HRV-BF group. For the SAB group, subjects controlled breathing at 6 cycles/min by the RSP pacer in 20 minutes, and were instructed to practice breathing at this frequency at home for a 20-minute period twice a day using the respiratory audio guide. For the control group, subjects were instructed to breathe spontaneously and sit in front of the computer screen, but were not instructed to breathe in a paced way or to maximize their HRV. In order to avoid hyperventilation, subjects of the HRV-BF and SAB groups were cautioned to breathe shallowly and naturally.
For the follow-up study, participants in the HRV-BF and SAB groups were told to practice abdominal breathing at least 20 minutes per day. While the breathing frequency was his/her RF in the last session for participants in the HRV-BF group, it was constant at 6 cycles/min for those in the SAB group.
Statistical analysis
Data were expressed as mean±standard deviation. Variables deviated from the normal distribution (positively skewed), including standard deviation of normal-to-normal beats (SDNN), square root of the mean of the sum of differences between subsequent IBI (RMSSD), total power of spectral density in the range of frequencies between 0 and 0.4 Hz (TP), very low-frequency power from 0.0033 to 0.04 Hz (VLF), LF and HF, were log-transformed (log10) before the correlation study. Differences between the means of the HRV-BF, SAB, and control groups were assessed by one-way analysis of variance with least significant difference multiple range tests. The difference of the pre- and postintervention of the same treatment group was analyzed using the paired t test. The correlation analysis was performed using Pearson correlation coefficient.
Results
Baseline characteristics of prehypertensive and normotensive subjects
Three hundred and ten (310) colleges students were screened for prehypertension, and it was found that the prevalence of prehypertension was 14.5%, higher in men than in women (24% and 4.6%, respectively, χ2=23.6, p<0.01). Vagus-associated HRV was significantly lower in prehypertensive subjects than in normotensive subjects, while GSR was the opposite (Table 1).
Values are mean±standard deviation or number.
Differences between prehypertensive and normotensive subjects.
SBP, systolic blood pressure; DBP, diastolic blood pressure; NS, not significant; GSR, galvanic skin response; SDNN, standard deviation of the interbeat interval (IBI); RMSSD, square root of the mean of the sum of differences between subsequent IBI; NN50, number of subsequent pairs that differ more than 50 ms; pNN50, NN50 expressed as a percentage of the total; TP, total power of spectral density in the range of frequencies between 0 and 0.4 Hz (ms2); VLF, very low frequency power from 0.0033 to 0.04 Hz; LF, low-frequency power from 0.04 to 0.15 Hz; HF, high-frequency power from 0.15 to 0.4 Hz; LF norm, normalized low frequency after application of a mathematical ratio on LF; LF norm=LF/(TP – VLF)*100; nu, normalized unit; HF norm, normalized high frequency after application of a mathematical ratio on HF; HF norm=HF/(TP-VLF)*100; LF/HF, ratio of the LF norm over the HF norm; RSP, respiration.
The BRS of prehypertensive subjects and the correlation between BRS and LF
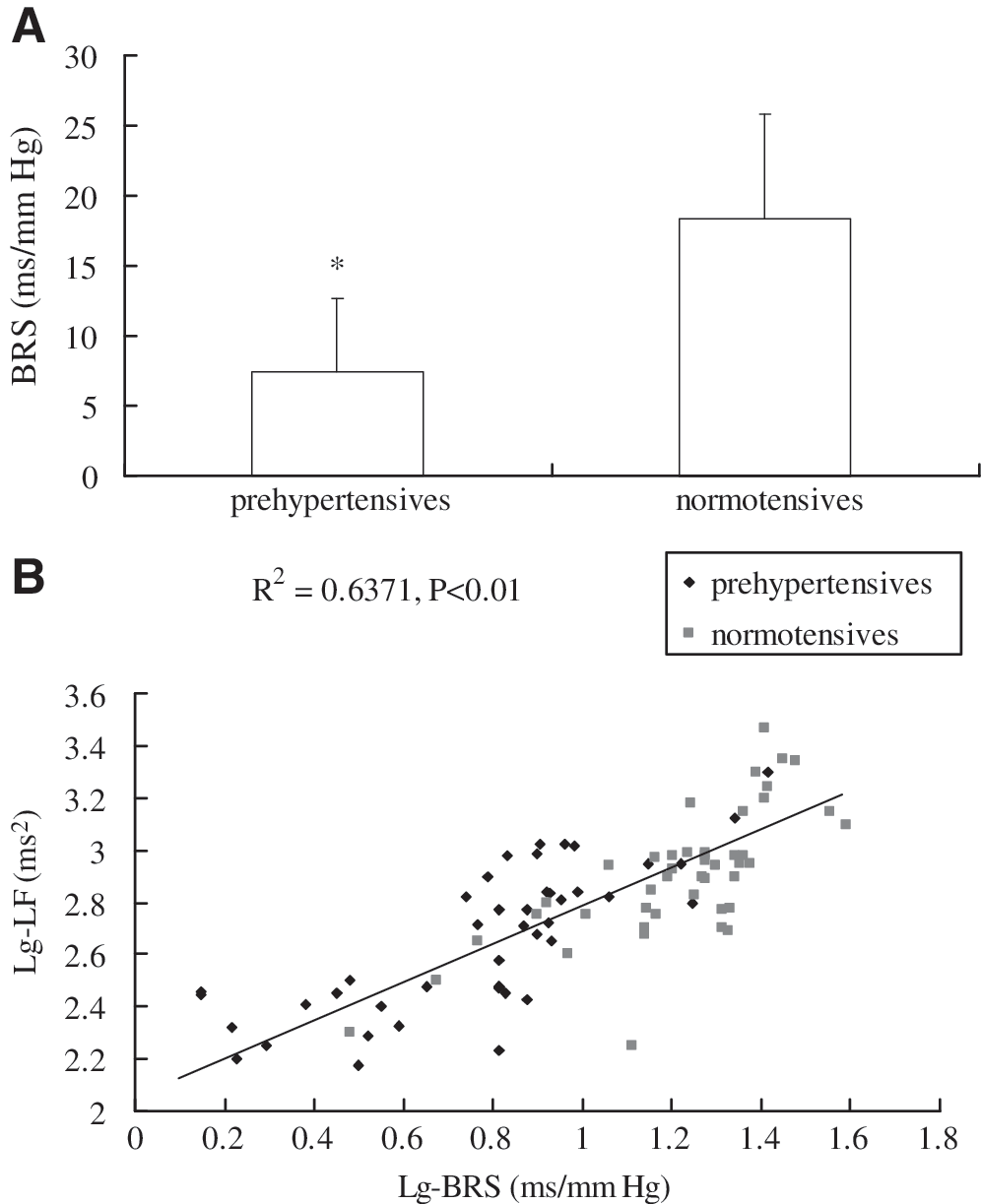
The BRS of prehypertensive subjects was significantly lower than that of normotensive subjects (7.5±5.2, and 18.4±7.4 ms/mm Hg, respectively, p<0.01) (Fig. 1A). The correlation between the BRS and LF of all 89 subjects was analyzed and it was found that log-transformed LF power correlated positively with log-transformed BRS (R 2=0.6371, p<0.01) (Fig. 1B).
Overall effects of HRV-BF and SAB on blood pressure
The HRV-BF significantly decreased SBP and DBP (from 131.7±8.7/79.3±4.7 mm Hg to 118.9±7.3/71.9±4.9 mm Hg, p<0.01), and this effect lasted for at least 3 months during follow-up (118.9±6.6/72.4±5.6 mm Hg, compared with pre-intervention p<0.01). The SAB also significantly decreased BP (from 131.3±7.6/80.1±5.7 mm Hg to 123.6±6.6/75.7±3.9 mm Hg, p<0.01), and this effect lasted for at least 3 months during follow-up (124.3±7.1/75.0±2.7 mm Hg, compared with pre-intervention p<0.05). The control group showed no significant differences in pre- and postintervention or in follow-up study. Postintervention and follow-up SBP in the HRV-BF group were significantly lower than those of the SAB group. Postintervention DBP in the HRV-BF group was significantly lower than that of the SAB group, whereas the follow-up study showed the same trend, with no significant change, however (Fig. 2). All groups showed no significant changes in HR.

Acute effects of HRV-BF and SAB on blood pressure within sessions
Baseline BP (30-minute quiet rest before training) and recovery BP (after 40-minute training) in sessions 1, 4, 7, and 10 were analyzed. Decrease of SBP or DBP means the baseline minus the recovery of SBP or DBP. Figure 3A shows that HRV-BF and SAB significantly lowered the SBP more than control in sessions 1, 4, and 7 (reduction of 7.0±3.4, 6.4±2.6 mm Hg for session 1, 11.2±5.0, 6.9±3.4 mm Hg reduction for session 4, and 8.8±4.2, and 4.7±3.2 mm Hg for session 7, respectively, p<0.05). In session 10, HRV-BF significantly lowered the SBP than control (reduction of 6.1±2.3 mm Hg, p<0.05), whereas SAB showed the same trend, but not statistically significant. More importantly, HRV-BF decreased SBP more than SAB did in sessions 4, 7, and 10 (p<0.05), although the difference in session 1 was insignificant. Figure 3B shows the effects of both interventions on DBP. The results were similar to those for SBP with the exceptions that the decrease by SAB was not significantly different than control in session 7, and the decrease by HRV-BF was not significantly different from that by SAB in session 10.

Effects of HRV-BF and SAB on BRS
HRV-BF and SAB significantly increased BRS (from 7.0±5.0 to 15.8±5.3 ms/mm Hg; and from 7.8±4.6 to 11.0±4.0 ms/mm Hg, respectively, p<0.01). On the other hand, the control group showed no significant changes. HRV-BF exerted a greater effect of normalizing the BRS than SAB did (comparison between pre- and postintervention of HRV-BF and SAB, p<0.01) (Fig. 4).
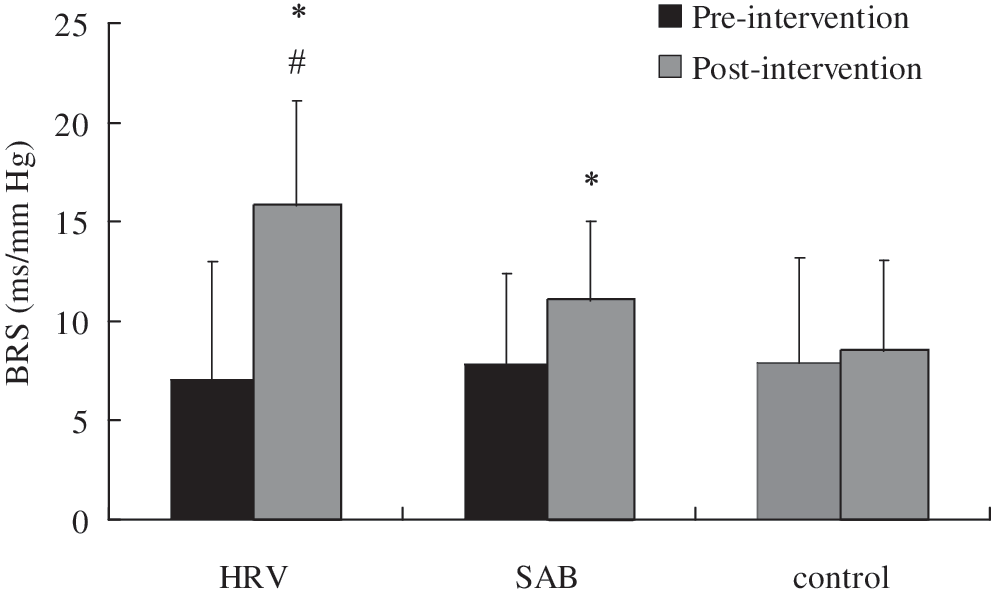
Effects of heart rate variability (HRV)–biofeedback on baroreflex sensitivity (BRS). *p<0.01 versus pre-intervention, #p<0.01 versus slow abdominal breathing (SAB) group.
Changes of the anthropometric indices before and after intervention
For the HRV-BF group, postintervention analysis of the anthropometric indices indicated that SDNN, TP, RMSSD, pNN50, VLF, LF, and HF were significantly increased (p<0.01) and GSR was significantly decreased (p<0.01). For the SAB group, SDNN, TP, VLF, and LF were significantly increased (p<0.05), with minor and no significant changes of HF and GSR. Also, LF norm, HF norm, and LF/HF and other anthropometric measures, including HR, SpO2, and RSP rate of pre- and postintervention showed no changes in both groups. Moreover, SDNN, TP, RMSSD, HF, and pNN50 were significantly higher after HRV-BF intervention than after SAB intervention (p<0.05; Table 2).
p, pre versus post heart rate variability–biofeedback (HRV-BF); ** p, pre- versus post- slow abdominal breathing (SAB); *** p, post HRV-BF versus post-SAB.
HR-BF, heart rate variability–biofeedback; log(10)SDNN, standard deviation of normal-to-normal beats; RMSSD, square root of the mean of the sum of differences between subsequent interbeat interval; NS, not significant; VLF, very low-frequency power from 0.0033 to 0.04 Hz; LF, low-frequency power from 0.04 to 0.15 Hz; HF, high-frequency power from 0.15 to 0.4 Hz; TP, total power of spectral density in the range of frequencies between 0 and 0.4 Hz (ms2); LFnorm(nu), normalized low frequency after application of a mathematical ratio on LF, LF norm=LF/(TP−VLF)×100; HFnorm(nu), normalized high frequency after application of a mathematical ratio on HF; LF/HF, ratio of the LF norm over the HF norm; pNN50, number of subsequent pairs that differ more than 50 ms expressed as a percentage of the total; GSR, galvanic skin response; SpO2, pulse oximetry; HR-BVP, heart rate from blood volume pulse; RSP, respiration.
RF changes with the progression of HRV-BF treatment
Before treatment, RF of participants in HRV-BF differed from person to person (6 cycles/min for 11 subjects, 6.5 cycles/min for 4 subjects, and 5.5 cycles/min for 3 subjects) with a mean baseline RF value of 6.03±0.32 cycles/min. RF was significantly decreased over time during training (5.61±0.40, 5.25±0.41, and 5.09±0.30 cycles/min in sessions 4, 7, and 10, respectively, p<0.01) (Fig. 5).
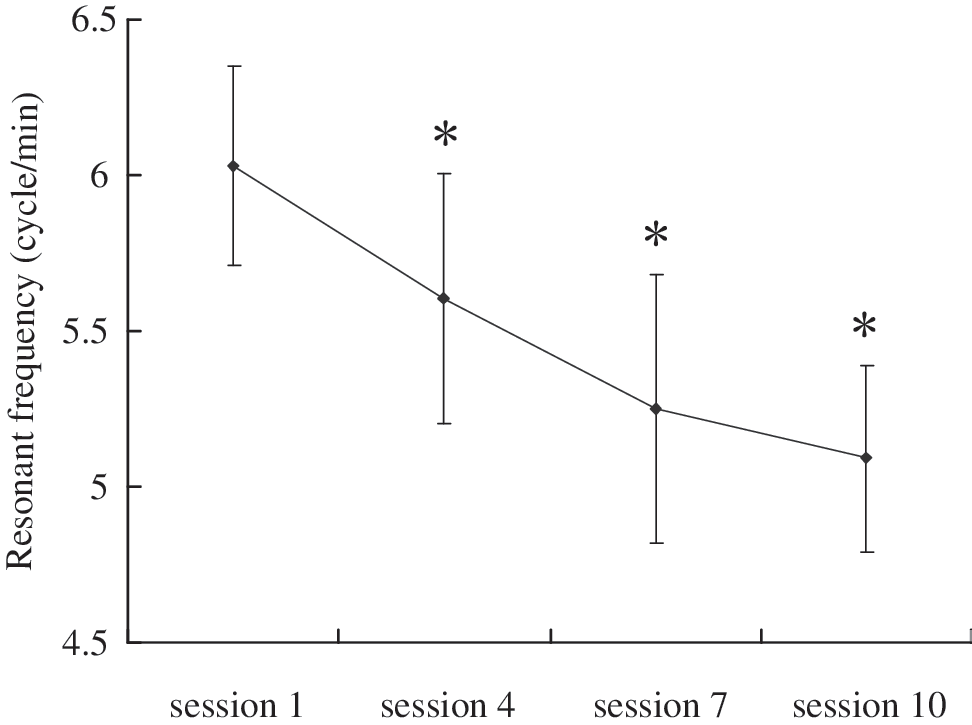
Resonant frequency changed during the progress of the treatment. *p<0.01 versus session 1.
Changes of the anthropometric indices for participants breathing in RF
In order to investigate whether breathing in RF was more beneficial than breathing in other frequencies, 10-session post-HRV-BF intervention subjects were instructed to breathe in his/her RF, RF plus 0.5 cycle/min, and RF minus 0.5 cycle/min. Individuals breathing in his/her RF resulted in significantly higher SDNN, TP, pNN50, and RMSSD and significantly lower GSR than breathing in other frequencies. HF for breathing in RF was slightly higher than that of breathing in other frequencies, but the differences were not significant. LFnorm, HFnorm, LF/HF, and HR had no significant differences among these breathing frequencies (Table 3).
p, resonant frequency (RF) versus RF+0.50; ** p, RF versus RF –0.5.
RSP, respiration; LF, low-frequency power from 0.04 to 0.15 Hz; SDNN, standard deviation of the interbeat interval; TP, total power of spectral density in the range of frequencies between 0 and 0.4 Hz (ms2); RNSSD, square root of the mean of the sum of differences between subsequent interbeat interval; VLF, very low-frequency power from 0.0033 to 0.04 Hz; HF, high frequency; LF/HF, ratio of the LF norm over the HF norm; pNN50, number of subsequent pairs that differ more than 50 ms expressed as a percentage of the total; GSR, galvanic skin response; HR, heart rate.
Discussion
Prehypertension, which first appeared in the Seventh Report of the Joint National Committee (JNC 7) in 2003, defined as BP between 120–139 mm Hg and 80–89 mm Hg, is a major public health concern. Prehypertension is highly prevalent and associated with the traditional cardiovascular risk factors. Individuals classified as prehypertensive were more likely to develop hypertension compared with those with normal BP. 28,29 The current study showed that the prevalence was 14.5% for young people in China, and it was higher in men than in women.
Studies have shown that baroreflex gain may be reduced in hypertensive subjects. 30,31 However, data are still scarce about BRS in prehypertensive individuals. In this study, it was found that BRS of those with prehypertension was significantly lower than that of subjects who were normotensive. Also, decreased HRV has been associated with increased cardiac mortality and morbidity. 32 In the current results, HRV analysis for those who were prehypertensive showed that the indices representative of the total variance (SDNN and TP) and absolute values of LF and HF components were lower than those who were normotensive. All of these differences showed that BRS and HRV of prehypertensive subjects have been altered.
RSA is the variation of heart rate that accompanies breathing. Heart rate increases during inhalation and decreases during exhalation. HRV-BF, also called RSA biofeedback, forces each individual to breathe within the low-frequency range, namely, the RF. This maximizes RSA and markedly increases HRV. Low-frequency oscillations of HR (0.04–0.15 Hz) are thought to be affected by both sympathetic and parasympathetic activity and are tightly correlated with measures of baroreflex activity. 33 –37 The results of this study showed that LF oscillations of heart rate correlated positively with the BRS, suggesting that a reduction of the absolute values of LF may be related to the lowering of BRS for those with prehypertension and to the reduction of the total variance. HRV-BF caused people to breathe at a rate at which RF occurs for heart rate oscillations, namely, cardiac rhythms associated with respiration and those caused by baroreflex activity (LF oscillations). This might present some treatment opportunities.
This controlled randomized pilot study is among the first to assess the feasibility of an HRV-BF as an intervention for prehypertension. These results have shown that prehypertensive participants could lower their SBP by 13.8 mm Hg and DBP by 7.2 mm Hg through 10-session HRV-BF. This BP-lowering effect lasted at least 3 months after treatment. Studies 31,38 showed that paced breathing, and particularly slow breathing at 6 cycles/min, reduced BP of hypertensive patients. In this study, results of the SAB group were consistent with these findings. Postintervention BP comparison between the HRV-BF group and the SAB group indicated that HRV-BF had significantly greater reductions in SBP than SAB did, and the trend for reduction of DBP was also present, but not statistically significant, probably because DBP of prehypertensive individuals was not as high. In addition, this study also found that subjects in sessions 4–7 of HRV-BF intervention had greater reductions in BP than subjects of SAB intervention, but the difference was less after session 7, probably due to a lower baseline BP.
There were many possible explanations for the effects of HRV-BF intervention on prehypertension. First, BRS can be enhanced significantly by HRV-BF, and this effect was significantly greater than with SAB. Vaschillo and colleagues provided evidence that breathing at RF by HRV-BF stimulated the baroreflexes and then “exercised” them. 39 The present authors have confirmed that HRV-BF training combined with breathing instructions could increase BRS more effectively than simple slow breathing, thereby producing a greater level of BP regulation. Second, over a 5-week intervention period, pre- and postintervention HRV of the HRV-BF group were significantly higher than those of the SAB group. For postintervention, vagus-associated HRV indices, including RMSSD, pNN50, and HF power, were significantly increased. These findings indicated that HRV-BF could increase the vagal tone. Additionally, our results showed that GSR, the index of sympathetic arousal, was significantly decreased after 10 sessions of HRV-BF, while no significant changes of this indicator were found after SAB. Since elevated sympathetic tone is an important factor in the development of hypertension, 40 HRV-BF, as a way of training people to learn how to relax and lower sympathetic arousal, has already been helpful for the regulation of BP. All of these autonomic responses contribute to the reduction of BP. Collectively, HRV-BF, based on the premise that breathing at one's RF could strengthen baroreflexes, increase vagal activity, and reduce sympathetic activity, was conducive to the lowering of BP. Irrespective of what mechanism is most important, it is reasonable to assume that changes in autonomic nervous activity and in BRS are interrelated. 41
The exact frequency at which resonance occurs tends to vary across individuals. The results of this study indicated that the average RF was 6.0±0.3 at the beginning, and then gradually decreased. Additionally, these results demonstrated that individuals breathing in the RF could result in significantly higher SDNN, pNN50, and RMSSD and significantly lower GSR than breathing in other frequencies. It thus might be expected that HRV-BF should exert greater modulatory effects than simple paced breathing at 6 cycles/min.
Conclusions
Overall, results from this study have shown that individuals with prehypertension had blunted baroreflex gain and impaired HRV. HRV-BF could improve these abnormalities, thus facilitating the regulation of BP. This technique is confirmed to be an effective intervention, which is easy to learn and has no adverse side-effects for individuals with prehypertension. Further research should focus on the generalization of this intervention among individuals of all ages with prehypertension or even with hypertension, as well as its in-depth mechanism in the modulation of BP.
Footnotes
Acknowledgments
This work was supported by the funded projects of Science and technology projects in Guangdong Province (No.: 2008B030301098) and the Science and technology projects in Guangzhou (No.: 2007J1-C0171). We acknowledge Prof. Chiu Shuen Hui (Indiana University–Purdue University Indianapolis) for reading and correcting the manuscript.
Disclosure Statement
There are no conflicts of interest.