
Abstract
Objectives:
Stress impacts on health, causing stress-related illness. The aim of this study was to investigate stress dampening effects of the homeopathic combination remedy dysto-loges® S on physiological and psychological measures during acute stress. Additionally, effects of the substance on sleep and life quality were investigated.
Design:
This randomized, double-blind, placebo-controlled single center study had a total duration of 15 days for each participant.
Setting/location:
The study was performed by Daacro, Trier, Germany.
Subjects:
We included 40 women aged 30–50 years that regularly experienced impaired well-being when feeling stressed.
Intervention:
Participants took three tablets daily for 14 days. On the final study day, participants took three pills in the morning and upon arrival at the study site. Thereafter, the Trier Social Stress Test (TSST) was performed.
Outcome measures:
Primary endpoints were saliva cortisol responses to the stress test. Secondary biological endpoints were plasma cortisol, adrenocorticotrophic hormone, epinephrine, and norepinephrine (NE) and heart rates. Psychological secondary endpoints were well-being, anxiety, stress, and insecurity during the stress test as well as sleep and quality of life.
Results:
Stress-induced cortisol levels did not differ between groups, but verum-treated participants were characterized by lower NE levels. Two weeks of treatment with the homeopathic substance resulted in a better sleep quality. Sleep improvement was associated with a higher hormonal response to the TSST in both groups. In addition, individuals with impaired sleep in the placebo group had higher unstimulated NE levels.
Conclusions:
This study provides preliminary evidence for beneficial effects of dysto-loges S on sleep quality. Improvement of sleep quality was positively associated with a normalized neuroendocrine stress response during acute stress, whereas an altered hormonal response was observed in participants with impaired sleep. We hypothesize that the test product may possibly reduce NE release.
Introduction
However, continuous exposure to stressors and consequent hyperactivation of the HPA-axis have been linked to a wide range of physical and psychological disturbances, such as gastrointestinal and cardiovascular disorders, depression, anxiety, sleep disorders, and emotional disturbances. 2 Some individuals, however, show a drop of cortisol levels after a prolonged period of stress, which is associated with fatigue, pain, and irritability. 3 Furthermore, flattened cortisol slopes and lower respiratory sinus arrhythmia during an acute stressor have been associated with disrupted sleep. 4 Women seem to be particularly vulnerable to stress. While the reasons are not fully understood yet, differences in both biological and psychological stress responses are discussed. 5
In the present study, we investigated a homeopathic combination remedy (dysto-loges® S, Dr. Loges & Co GmbH, Schützenstrasses 5, D 21423 Winsen, Germany) used in the field of nervous disorders, such as sleep disorders, headache, and vertigo. 6 We tested the preparation for effects in women who experience physical symptoms without organic findings when feeling stressed. The first objective of the study was to assess effects of dysto- loges S on saliva cortisol responses to the Trier Social Stress Test (TSST), 7 an efficient laboratory protocol for inducing acute psychosocial stress in humans. 8 Furthermore, we measured additional stress-sensitive biological and psychological parameters as well as changes in general well-being and sleep quality to explore the possible impact of the homeopathic preparation on the stress response.
Materials and Methods
This study was approved by the Independent Ethics Committee of the Medical Association Rhineland-Palatinate and performed in accordance with the ethical principles of the Declaration of Helsinki that are consistent with the guidelines for Good Clinical Practice provided by the International Conferende on Harmonisation of Technical Requirements for registration of Pharmaceuticals for Human Use (ICH/GCP).
This was a randomized, double-blind, placebo-controlled single center study conducted at study sites of a contract research organization (Daacro) in Germany. Eligible participants were women aged 30–50 years that were employed full-time and met the eligibility criteria of experiencing physical symptoms without organic findings when stressed. Such symptoms included uneasiness, nervousness, attention deficit, tension, fatigue, sleep disorders, headaches, lack of concentration, and gastro-intestinal disorders. Exclusion criteria were smoking, alcohol/drug addiction, pregnancy, any acute or chronic diseases, any medication interfering with study outcome measures, lack of good health assessed by a physician and laboratory parameters, any other study participation during the past 6 months, and/or the lack of internet access at home.
The study included two visits for each participant. At the first visit, participants received extensive study information and signed an informed consent. A medical examination, including a hemogram, verified all inclusion and exclusion criteria. Physiological (a) and psychological (b) baseline measures were collected: (a) weight, height, waist–hip ratio, body mass index, and (b) psychometric questionnaires Trier Inventory for Chronic Stress 9 (TICS) and the State-Trait-Anxiety Questionnaire 10 (STAI-X2). Participants were randomly assigned to receive dysto-loges S or a matching placebo. Thereafter, participants were instructed about substance intake and electronic completion of the sleep questionnaires (visual analgue scales for sleep quality, VIS) 11 in the evening (VIS-A) and morning (VIS-M). The VIS was completed for 8 days: i.e., the first 7 days and nights of treatment as well as the evening of study day 14 and the following morning. The first VIS completion was done prior to substance administration. On the final study day (day 15), participants returned to the study site for their final appointment, which included the psycho-social stress test (TSST). 7 The duration of the final appointment was 2.5 hours in total.
After arrival at the study site, participants received an indwelling catheter and took their last treatment dose. Thereafter, questionnaire data and saliva and blood samples were collected in regard to the TSST. The TSST is a motivated performance task consisting of a brief introduction by the study manager (2 minutes) and a preparation period for the participant (3 minutes), followed by a test period in which the participant applies for an imaginary job (5 minutes) and performs mental arithmetic (5 minutes) in front of an audience. The total exposure time adds up to 15 minutes.
With respect to the TSST, pre-stress and post-stress psychometric assessments regarding participants' state anxiety (STAI X1) and multidimensional mood states
12
(MDBF) were performed. Additionally, visual analogue scales
13
(VAS) for perceived stress, anxiety, and insecurity were used prior to, during, and immediately after the TSST. Heart rates were recorded for 55 minutes continuously starting 20 minutes prior to the TSST with a Polar device (S610i, Polar Electro GmbH, Büttelborn, Germany). Saliva and plasma cortisol sampling took place prior to (−2 minutes) and after the TSST (+1, +10, +20, +30, +45, +60 minutes). Furthermore, serum samples for ACTH, NE, and E determination were collected 2 minutes prior to and 1 minute after the TSST. All biological and psychological data were collected between 2:00 and 6:00
Saliva cortisol samples were collected using Salivettes® (Sarstedt, Nümbrecht, Germany) and analyzed employing a time-resolved immunoassay with fluorometric detection 14 (Wallac, Turku, Finland). Blood samples were collected by a physician in (EDTA)-Monovettes® (Sarstedt). Plasma cortisol and ACTH levels were determined using enzyme-linked immunosorbent assays (IBL, Hamburg, Germany). Catecholamines were analyzed employing a high pressure liquid chromatography and an electro-chemical detector (Chromsystems GmbH Munich, Germany).
Intervention
Participants either received dysto-loges S or a matching placebo in tablet form. dysto-loges S is sold in pharmacies over the counter in Germany. As active agents, dysto-loges S tablets contain Passiflora incarnata TM (mother tincture, 13 mg) along with Gelsemium D4 (39 mg), Reserpinum D6 (31.2 mg), Coffea D6 (33.3 mg), and Veratrum D6 (33.3 mg). Placebo tablets only contained the inactive components of dysto-loges S (i.e., corn starch, lactose monohydrate, and magnesium stearate). Test and placebo substances were identical in odor, taste, and color. Packaging and labeling of the study medication was done by the Pharmacy of the University Clinic Mainz, Germany. Daacro received the prepacked bottles, which were numbered according to the randomization sequence. All participants were asked to take three tablets of dysto-loges S or the matching placebo daily for the duration of 14 days. The women were instructed to take one tablet before each meal (breakfast, lunch, and dinner) and hold it in their mouth until dissolved, without consuming caffeinated drinks or essential oils at the same time. On the last study day (day 15), participants took three tablets before breakfast and an additional three tablets upon arrival at the Daacro study site. Treatment compliance was monitored by MEMS (Medication Event Monitoring System, AARDEX Ltd., Zug, Switzerland). MEMS containers have an electronic lid that records time and date of each opening. Therefore, opening of the container was reliably monitored and it was assumed that the substance was taken. Previous studies revealed compliance was improved when participants were aware of the monitoring procedure. 15
Sample size calculation
Sample size calculation was based on the main outcome measure cortisol and was calculated with G*Power 3.1.2. 16 using F-test family functions for repeated measures. We defined α-error probability as 0.05 and the β-error as 0.20. Sample size was supposed to be large enough to reveal a small to medium effect (effect size f=0.18). A sample size of n=20 individuals per group was determined referring to a total sample size of N=40.
Randomization
The randomization sequence was stratified with a 1:1 allocation using random blocks of variable sizes with the computer software SPSS 17.0 (IBM Corporation, Somer, NY). The randomization sequence was generated by an employee of Trier University with no clinical involvement in the trial. Participants were sequentially enrolled by the study manager, assigned a random number, and given the tablets in the corresponding bottle. The randomization schedule was concealed from the study manager enrolling the participants as well as from the study assistant and medical staff. Information concerning the allocation of participants was sequentially numbered and sealed in envelopes that were kept by the CEO of the contract research organization. Envelopes were opened only after study termination.
Statistical analysis
The sleep questionnaires (VIS-A and VIS-M) were analyzed using data collected on the first day (baseline), and after 7 as well as 14 days of substance intake. For analyses of heart rate, means were computed for seven time intervals: sitting and standing prior to the TSST, preparation for the TSST, job interview during the TSST, TSST arithmetic, and standing and sitting after TSST. For the ancillary analysis, we tested the effect of sleep improvement on physiological stress measures. Consequently, we further assigned subjects to subgroups according to improvement of sleep quality, which was determined by subtracting the baseline from values collected after the treatment period. Increases of the physiological parameters saliva and plasma cortisol, ACTH, E, NE, and heart rate were calculated by subtracting the baseline from maximum values.
For data analysis, we used the intention-to-treat principle. Statistics were performed with R Statistical Computing version 2.10.0. 17 Residuals were tested for normality visually with the qq-plot and with the Shapiro-Wilk test prior to statistical analyses. Accordingly, right-skewed data were transformed using logarithmic functions and left-skewed with mathematical root functions. Means (SE) are shown for all data presented in figures. Means (lower and upper confidence intervals [CI]) are shown for the primary endpoint and all secondary outcome measures.
Baseline values for demographic and psychological parameters were compared using the t-test for independent samples. The primary study endpoints was the stress-induced change of cortisol levels. Secondary biological endpoints were plasma cortisol, ACTH, catecholamines, and heart rates. Secondary psychological endpoints were perceived stress, anxiety, insecurity, mood, calmness, alertness, and life and sleep quality. For investigating effects of the homeopathic test substance on primary and secondary study outcomes, mixed-effects models were used. Mixed-effect models were fitted with the lme4 package with Laplace approximation of the likelihood function. 18 The p-values were calculated by likelihood-ratio tests based on changes in deviance (using maximum likelihood estimates) when each term was dropped from the full (main effects) model. Interactions were tested by considering changes when these were added to the model. 19 Mixed-effects models included experimental group as two-level factor and number of measurements of the dependent variable (time); individual identity was included as a random factor. In addition, an ancillary analysis was performed to investigate the relationship of sleep quality and experimental group affiliation on biological stress measures. For this, univariate ANOVAs were used which included subgroup and experimental group as two-level factor. Only significant interactions are reported. Effect sizes are reported for all results either calculated as Nagelkerke's pseudo R 2 (mixed-effects models) or η2 (univariate ANOVA).
Results
Baseline demographics
A total of 50 women were enrolled in this study, of which 10 were excluded because they did not meet the inclusion criteria. Forty healthy women entered the study (first participant enrolled: November 27, 2009; last participant completed: December 22, 2009). One participant withdrew from the study due to personal problems; 39 participants completed this study. The intention-to-treat principle was used for data analysis. A participant flow is presented in Fig. 1.

Participant flow diagram.
There were no group differences regarding baseline demographic parameters (Table 1). In addition, participants of both experimental groups had similar scores in trait anxiety (STAI X2: placebo: mean [SE] 42.85 (2.69), treatment: 47.10 (2.62); t=1.13, p=0.264) and perceived stress (PSS: 28.45 [1.77], 26.56 [2.14]; t=−0.69, p=0.496). Furthermore, women of both groups reported similar levels in chronic stress on the Trier Inventory for Chronic Stress (TICS; screening scale: 21.65 (2.05), 26.10 (3.17); t=1.15, p=0.258).
Data are means (SE).
p values base on t-tests for independent samples.
No adverse events were reported during substance intake. Compliance was very good; one participant violated the study protocol by taking one instead of three tablets per day at home.
Endocrine and autonomic measures
The TSST induced significant increases in saliva and plasma cortisol, catecholamines, and ACTH and heart rate in both the verum and the placebo groups (Tables 2 and 3). Participants treated with the homeopathic combination remedy had significantly lower NE levels as compared to the placebo group before and after the TSST (Fig. 2). 12% of between group variance in NE levels were accounted for by the treatment. There was no significant difference between verum and placebo treatment regarding stress-induced saliva and plasma cortisol levels, ACTH, and E levels. In addition, group comparison of heart rates revealed no differences.
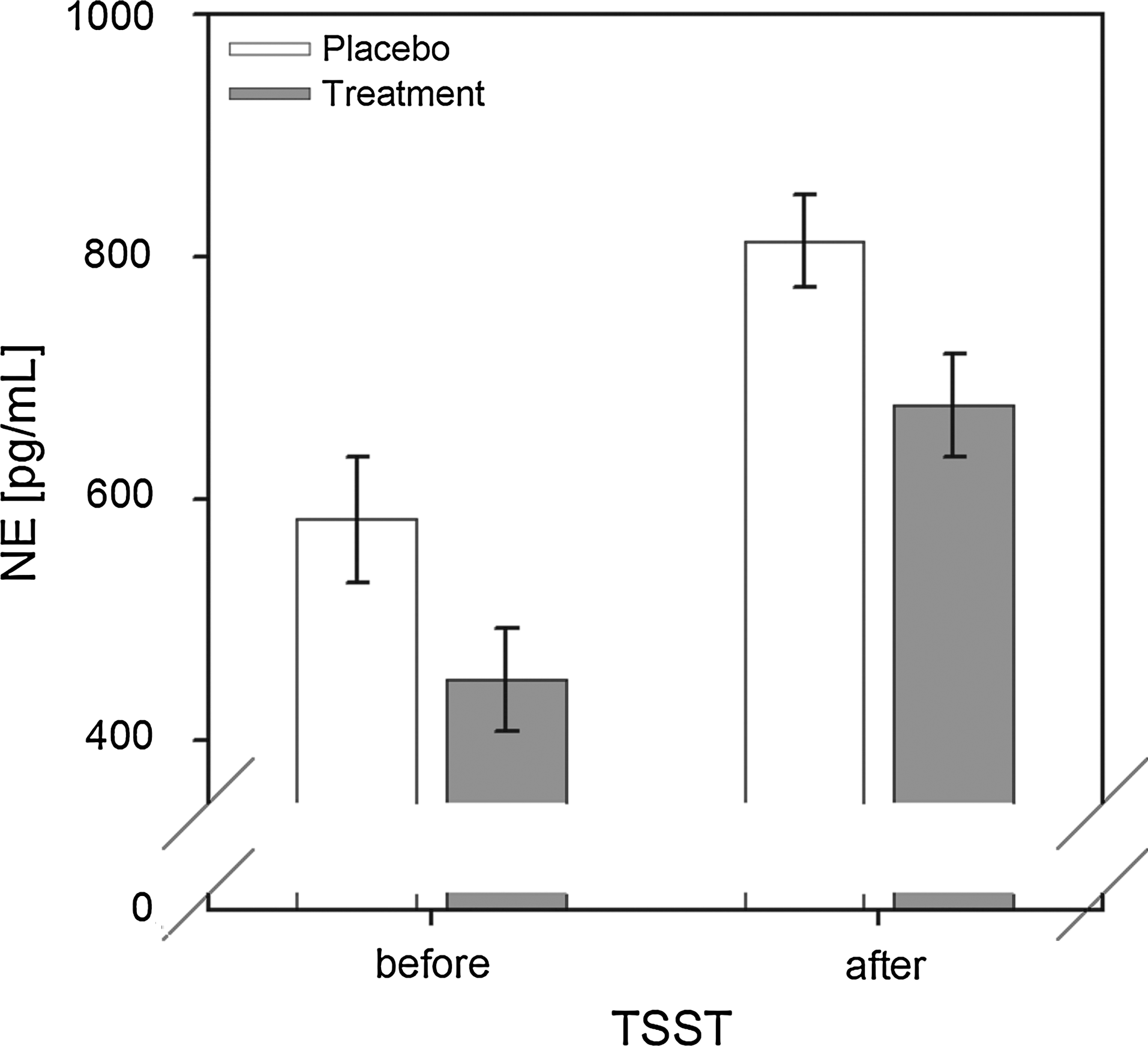
Norepinephrine (NE) levels before and after the Trier Social Stress Test (TSST) of experimental groups. Data are means (±SE).
ACTH, adrenocorticotrophic hormone; STAI, State-Trait-Anxiety Questionnaire; MDBF, multidimensional mood states; VAS, visual analogue scales; VIS, visual analogue scales for sleep quality.
p values are based on linear mixed model including time (=number of measurements) and group affiliation as factor as well as the random factor individual identity.
Questionnaires
Both experimental groups reported increases of stress perception, anxiety, and insecurity, as well as a decrease in positive mood, calmness, and alertness in response to the TSST. Values of psychological parameters did not significantly differ between verum and placebo. Data are provided in Tables 2 and 3.
Throughout the 14 treatment days, participants from both experimental groups reported a general improvement of their physical and mental health state: women reported being less stressed and experiencing fewer stress-related symptoms. In addition, they reported better concentration and easefulness and having fewer sleep disruptions per night (Tables 2 and 3). Furthermore, participants of the verum group had significantly improved sleep after the treatment period (p=0.010, R 2 =0.21; Table 2, Fig. 3). Sleep quality improved by around 30% in the verum group, and 21% of between group variance in sleep quality were accounted for by the treatment. In contrast, sleep quality did not differ between baseline and after treatment in the placebo group. There were no significant group differences in stress perception and stress symptoms, easefulness, and concentration as well as in time needed for falling asleep and in awakening at night.

Comparison of sleep quality between experimental groups. Data are means (±SE).
Effects of sleep quality on the physiological stress response
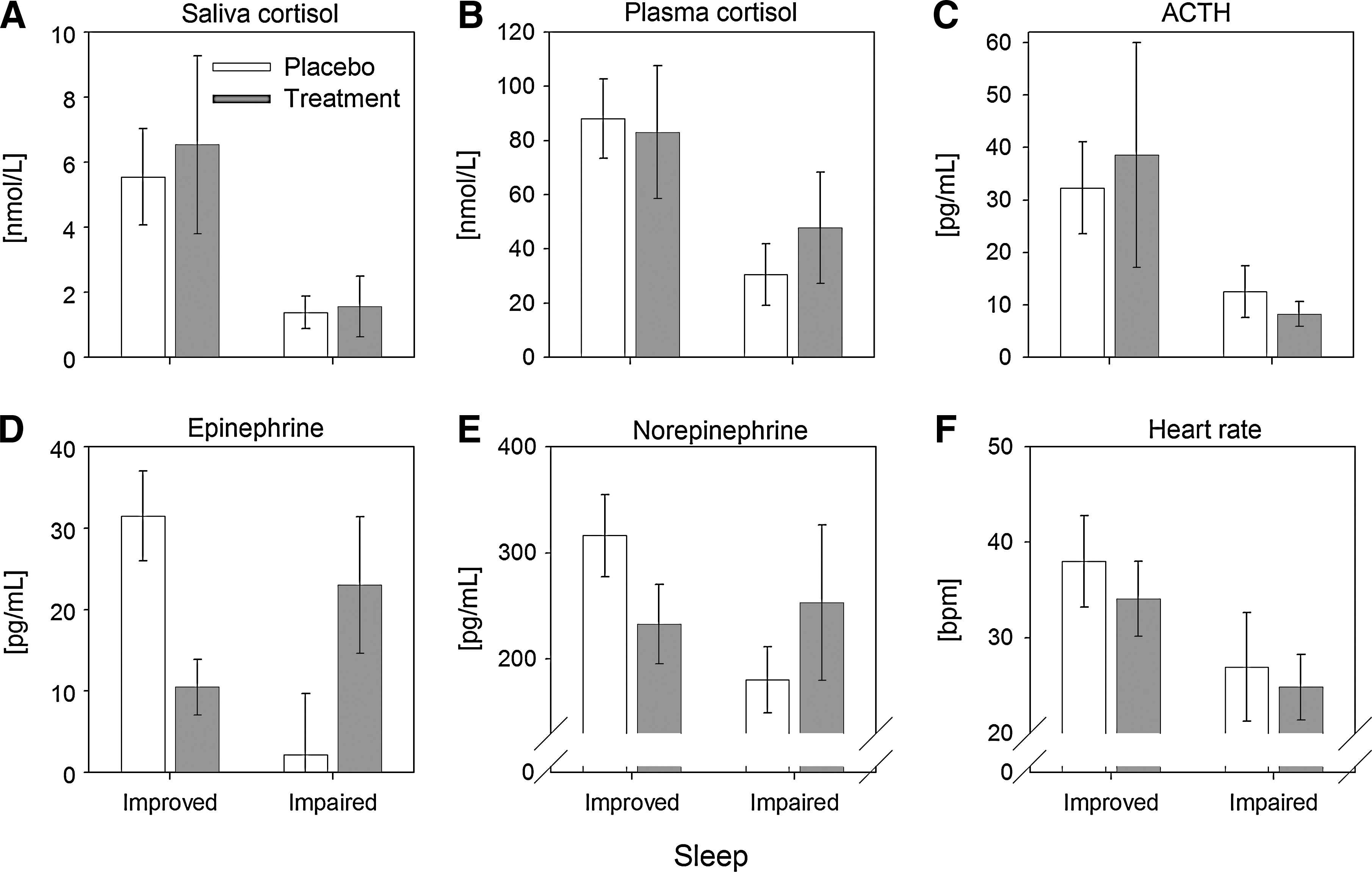
Saliva cortisol levels were blunted in participants with impaired sleep. This observation became most obvious after stress exposure (p=0.033, R 2 =0.18, Fig. 4A). In addition, participants of both experimental groups with improved sleep had similar NE levels prior to and after the TSST. In contrast, by trend, placebo individuals with impaired sleep had higher NE levels prior to the TSST as compared to participants with impaired sleep of the verum group (p=0.072, R 2 =0.11, Fig. 4B).

Saliva cortisol
Improved or impaired sleep quality affected saliva and plasma cortisol and ACTH and heart rate increases. Participants characterized by an improvement in sleep had higher saliva and plasma cortisol increases as well as ACTH and heart rate increases as compared to participants with impaired sleep quality (Table 4, Fig. 5). Furthermore, verum-treated participants with improved sleep quality had significantly lower E increases than placebo participants with sleep improvement (F=11.64, p=0.002, η2=0.29). This was not found for verum and placebo participants with impaired sleep quality. In addition, in the placebo group, the increase in NE was marginally lower in individuals characterized by impaired sleep as compared to participants with an improved sleep (F=2.99, p=0.095, η2=0.10).
Comparison of the stress-induced increase in hormonal parameters
p values are based on linear models which included experimental group affiliation and sleep group (improved/impaired sleep) as a two-level factor.
Discussion
We observed that participants from both experimental groups reported improved physical and mental health after verum or placebo intake. Thus, an expectation of positive treatment effects may have played an important role in our approach. Similar effects were reported for homeopathic treatment in anxiety disorders. 20
In response to the TSST, participants of both experimental groups had similar values in saliva and plasma cortisol and ACTH, heart rates, and E. Interestingly, however, plasma levels of NE were significantly lower in the treatment group before and after the TSST, with a comparable increase to psychosocial challenge in both experimental groups. Reserpine, one ingredient of dysto-loges S, results in a depletion of NE in both the brain and the sympathetic nervous system. This leaves the impression that homeopathic diluted (potentized) reserpine is able to induce the same effect. Notably, noradrenergic neurons in the brain can easily be sensitized by pharmacological and psychological challenges thus becoming hyperresponsive even to minor stimuli. 21 Under such conditions, a highly diluted administration of reserpine may possibly result in a response of noradrenergic neurons. Since the classic experiments on sensitization by Erik Kandel, 22 it became obvious that such principles exist even beyond classical conditioning. Yet, in laboratory models it was frequently shown that homeopathic potencies do not follow a classical dose–response relationship regarding their mere dilution level. 23 Thus, another explanation for the observed effects may still be an unknown mode of action of homeopathic dilutions.
Tonic activity of the dorsal noradrenergic system varies with individual alertness: during wakefulness, locus coeruleus (LC) neurons fire tonically with bursts of phasic, stimuli-related activity. 24 During non-REM sleep, NE release decreases gradually with sleep depth, while there is almost no noradrenergic activity during REM sleep. 25 Thus, a depletion of NE may significantly improve sleep quality, as observed in the treatment group. Furthermore, a subgroup analysis regarding improved or impaired sleep showed that placebo-treated individuals with impaired sleep had higher resting NE levels. Previous study have shown that prolonged strain such as sleep disruption or deprivation or fragmented sleep leads to altered challenged and unchallenged hormonal responses. 26 For example, a higher sympathetic activation is needed for maintaining wakefulness during a state of sleep debt after reduction of sleep time. 27 Moreover, it has been observed that prolonged total sleep deprivation leads to progressive NE increase in humans 28 and rats, 29 a state that is associated with exhaustion. 29 Additionally, other studies on humans showed that increased sympathetic activation is more related to fragmented and disrupted sleep than to sleep deprivation. 30,31
Increased NE concentrations and sleep disturbances have been observed in individuals that were exposed to chronic stress. 32 Furthermore, increased catecholamine levels have been reported for patients suffering from stress-related disorders with low cortisol outputs. 33,34 Hypocortisolism is particular found in individuals suffering from stress-related disorders such as chronic fatigue, burnout, and vital exhaustion. 35 –37 In our study, impaired sleep was also associated with a blunted cortisol response after stress exposure. Since cortisol exerts an inhibitory influence on catecholamine synthesis and release, our results may suggest that the lack of cortisol availability may have resulted in increased NE levels in the placebo group with impaired sleep. However, the exact mechanisms are not fully understood yet. 38 –40
Our results suggest that impaired sleep is associated with an altered hormonal response under stimulated and unstimulated conditions. Increased NE levels and hypocortisolism in individuals with impaired sleep may present signs of fatigue and exhaustion, triggering physical disorders in the long-run. The intake of dysto-loges S was associated with lower NE levels and improved sleep quality, possibly promoting an enhancement of overall quality of life. However, these interpretations are limited by the fact that NE levels were not assessed before the treatment period. Thus, one cannot exclude that NE levels in the treatment group were lower even before substance intake. This clearly needs to be analyzed in a replication study that includes baseline measurements. Furthermore, our main focus was on the biological response during an acute stressor and aspects of sleeping behavior were assessed only secondarily. Thus, we encourage future research primarily focusing on sleep.
Conclusions
Pharmacological effects of homeopathic remedies are a matter of long-lasting controversy. Nevertheless, it has already been shown that a homeopathic combination remedy against chronic infections was able to increase parameters of the nonspecific immune defense. 41 The data from this study support the viewpoint that such an effect is possible and measurable. Participants treated with dysto-loges S reported significantly better sleep quality than participants in the placebo group. Furthermore, we found significant differences between the placebo group and the verum group for plasma NE, and it is intriguing that the homeopathic drug may have induced these effects. Whether this is due to a hypersensitive response of target tissues to very small amounts of active compounds or to the claimed energetic effect of homeopathy remains speculative.
Footnotes
Acknowledgments
The authors would like to acknowledge the financial support of Dr. Loges & Co. GmbH for this study. We thank the anonymous referees for their comments.
Disclosure Statement
No competing financial interests exist.