
Abstract
Objectives:
This study sought to explore the characteristics of de qi using electroacupuncture at acupoints with different properties in the meridian category, histological type, and nerve innervations.
Methods:
Electroacupuncture was performed on 21 healthy volunteers at paired acupoints of ST36-GB34, CV4-CV12, ST36-ST28, PC6-PC7, and ST36-CV4. Upon acupuncture de qi, the intensities and the prevalence of individual sensations, sensation transmission, and the amplitude of electrical current were recorded. Chi-square, Fischer's exact test, Wilcoxon test, and two-sample paired t test were used to compare the components of de qi within each paired group.
Results:
Overall intensities and prevalence of individual sensations are fullness, numbness, soreness, tingling, heaviness, pressure, dull pain, warmness, and coolness in decreasing order. No significant difference was found in the prevalence of needling sensations between the two paired points (p>0.05). However, significant intensity differences (p<0.05) were showed in soreness, fullness, and heaviness between ST36-ST28, in fullness and numbness between ST36-CV4, and in fullness between CV4-CV12. Tingling sensation was stronger than heaviness and pressure at acupoints PC6-PC7 and ST36 (as paired with CV4). Sharp pain occurred in 10/216 tests (4.63%). Sensation transmission occurred highly (77.78%) on participants, and sensations mostly propagate over one joint but no further than two joints. Overall electrical current was 2.35±0.07 mA (mean±standard error). No significant difference was found between paired acupoints for the distance of sensation transmission and the amplitude of electrical current.
Conclusions:
Fullness, numbness, and soreness were the most common and obvious sensations associated with electroacupuncture. The difference of sensation intensities may be associated with different nerve innervations.
Introduction
Slightly different results have been reached by other researchers. In a survey with international acupuncture experts, MacPherson et al. 7 reported that aching, dull, heavy, numb, radiating, spreading, and tingling closely associate with acupuncture de qi in patients. Mao et al. 8 found that the most common types of needling sensations reported by subjects were distended (94%), sore (81%), electric (81%), and numb (78%), and 89% patients had propagation of the needling sensations. Hui et al. 9 found that aching, soreness, and pressure were the most common needling sensations in manual acupuncture at LI4, ST36, and LV3. However, in a randomized control trial, Kou et al. 10 found that acupuncture significantly induced higher visual analog scores values for numbness, pressure, warmness, and radiating paresthesia, but not for heaviness than sham acupuncture (nontraditional acupoints with 1–2-mm depth of needle insertion). In summary, the specific characteristics of needling sensations upon de qi of acupuncture vary in these studies, and most of the de qi results of these studies are based on manual acupuncture procedures, and little information on electroacupuncture is currently available.
As electroacupuncture (EA) becomes more popularized in clinical practice all over the world, systematical investigation on EA de qi sensations is becoming increasingly urgent. On the basis of the aforementioned acupuncture sensation literature and Traditional Chinese Medicine textbooks, 11,12 nine descriptors were selected to describe de qi needling sensations in the current EA study: soreness, fullness, numbness, warmness, heaviness, coolness, tingling, pressure, and dull pain. The aim of this study is to explore the characteristics of needling sensations with EA at acupoints of different properties.
Methods and Subjects
The needling sensation data were collected in a larger project applying functional magnetic resonance imaging (fMRI) to study the effects of acupuncture on brain activities; however, no fMRI data are demonstrated in the present article. Sensational data with sharp pain were deliberately removed because sharp pain has distinct hemodynamic responses as demonstrated by fMRI, and thus sensations with sharp pain are not considered de qi. 13,14 This study was performed at Guang'anmen Hospital, one of the largest tertiary-level teaching hospitals for Traditional Chinese Medicine in China. The hospital ethics committee approved the research protocol. Participants in this study were 22–28 years old, right-handed, young healthy volunteers, including 10 men and 11 women, 20 Chinese and 1 Mongolian. Prior to participation, all volunteers signed an informed consent form, were screened to eliminate those with major medical illnesses, history of head trauma, use of medications within 1 month, neuropsychiatric disorders, and prohibitions for MRI scanning.
EA procedures were performed by 2 acupuncturists with similar techniques on 10 and 11 subjects, respectively. The selected acupoints were paired as ST36-GB34, CV4-CV12, ST36-ST28, PC6-PC7, and ST36-CV4. Each pair of acupoints was randomly tested in one session, and in order to prevent confounding factors of previous needling procedures, at least 1 day's time interval between each experiment session was guaranteed for each participant.
For initial design, ST36 and GB34 share the same nerve innervations and the same histological type (segment L4–L5, muscle layer), but differ in meridian categories (Stomach versus Gallbladder); CV4 and CV12 are located in the same meridian and histological type (Ren meridian, connective tissue), but different nerve innervations (T7–8 versus T12); ST28 and ST36 belong to the same meridian and histological type (Stomach meridian, muscle layer), but the different nerve innervations (T12 versus L4-L5); PC6 and PC7 share the same meridian and nerve innervations (Pericardium meridian, C7), but differ in histological types (Muscle versus Tendon); ST36 and CV4 both are commonly used for health preservation, but are different in the abovementioned properties (Stomach versus Ren meridian, Muscle versus Connective tissue, L4-L5 versus T12).
Acupuncture protocol
Acupoints were localized according to Names and Localizations of Acupoints (GB/T12346-2006). 15 Silver needles (diameter 0.35 mm, length 40 mm) were used (Suzhou Medical Appliance Manufactory), together with a current-constant Han's Acupoint Nerve Stimulator LH204H (Neuroscience Research Center, Peking University, Beijing, China). The frequency of EA was set at 15 Hz.
The participants were in the supine position in the MRI scanner and were unable to see acupuncture procedures. Prior to study, acupuncturists instructed participants of possible de qi sensations and required them to report de qi sensations as well as sharp pain once they felt it; researchers in the team attached one electrode of the electric stimulator to the handle of the needle, and the other to the thenar skin of the palm. The needle was inserted perpendicularly to the skin surface to a depth of 0.5–3.0 cm depending on the acupoint. With manual acupuncture manipulations by 2 acupuncturists using a similar moderate reinforcing and reducing method, each participant reported de qi sensation; then an electric current was subsequently delivered to the handle of the needle. The researchers adjusted the electric current to the participant's best tolerated magnitude without noxious (sharp) pain. The experimental paradigm is shown in Figure 1. Periods of electric current delivery were interleaved with periods of needle at rest, each lasting 1 minute. The needle remained in place during the rest periods (without electric current delivery) R1, R2, and R3. Each procedure lasted a total of 5 minutes. At the end of each acupoint testing procedure, the participant was questioned by another researcher in the team with a prepared questionnaire to check whether each of the de qi sensations (soreness, fullness, numbness, warmness, heaviness, coolness, tingling, pressure, dull pain), sharp pain, or any other sensations occurred during the whole needle retention process, and to rate its intensity on a scale of 0–10 (1–3 mild, 4–6 moderate, 7–9 strong, 10 unbearable).
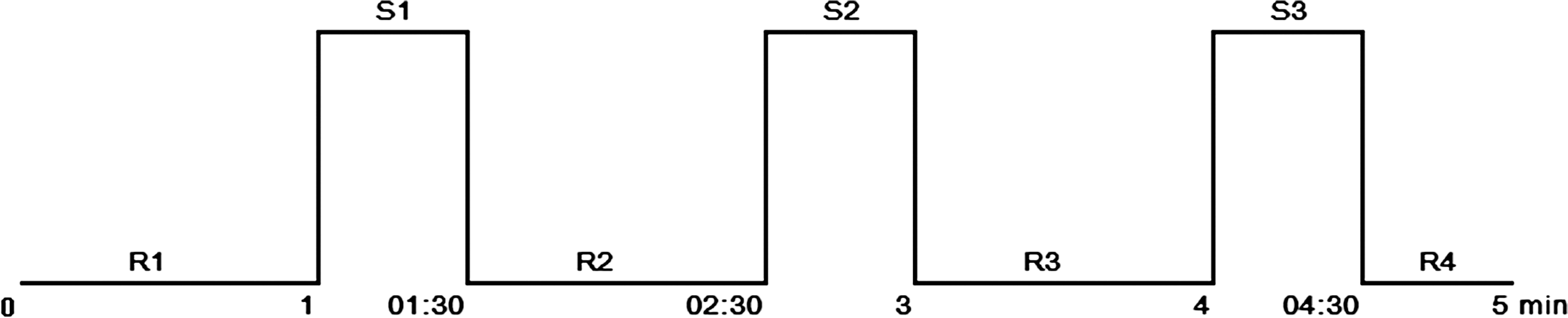
Needle was inserted in the acupoint before the functional magnetic resonance imaging scan started. R1, R2, R3 indicated no electric current was delivered; S1, S2, S3 indicated electric current on.
Statistical analysis
Statistical analysis was performed with the SPSS software package (version 11.5). Two (2) sample paired t tests were performed to compare the intensity of each individual sensation, sensation transmission, and best tolerated electric current between the paired acupoints (thresholded at p<0.05). Chi-square tests and Fischer's exact tests were used to compare the frequencies of sensation components for the paired acupoints. A total of 216 acupuncture procedures were performed, and all sensation data were retrieved through the questionnaire answered by participants after each EA procedure. Sharp pain occurred in 10 subjects (4.63%) during the entire 216 experiments. The data of 206 EA tests without sharp pain were analyzed for the characteristics of de qi sensation components. A total of 192 data (96 sessions of the paired acupoints) were collected for the analysis on needling sensations without sharp pain.
We quantitatively defined the sensation transmission reaching two joints or further as 3 points, one joint as 2 points, and local transmission as 1 point. The best tolerated currents of 198 data were recorded and analyzed.
Results
General characterization of de qi with EA
The sequence of the intensity and frequency of individual sensations in de qi profile were shown as follows (from higher to lower): fullness, numbness, soreness, tingling, heaviness, pressure, dull pain, warmness, and coolness. Fullness, numbness, and soreness were the most common sensations, followed by heaviness, pressure, and tingling; whereas dull pain, warmness, and coolness occurred less frequently. Similarly, the strongest needling sensations were noticed in fullness, numbness, and soreness, followed by heaviness, pressure, and tingling; whereas intensities were relatively low in dull pain, warmness, and coolness. For other needling sensations, throbbing was reported in 5 (2.43%), and slight anxiety was felt during 7 (3.40%) and tension in 1 (0.49%) acupuncture procedures (Figs. 2 and 3).
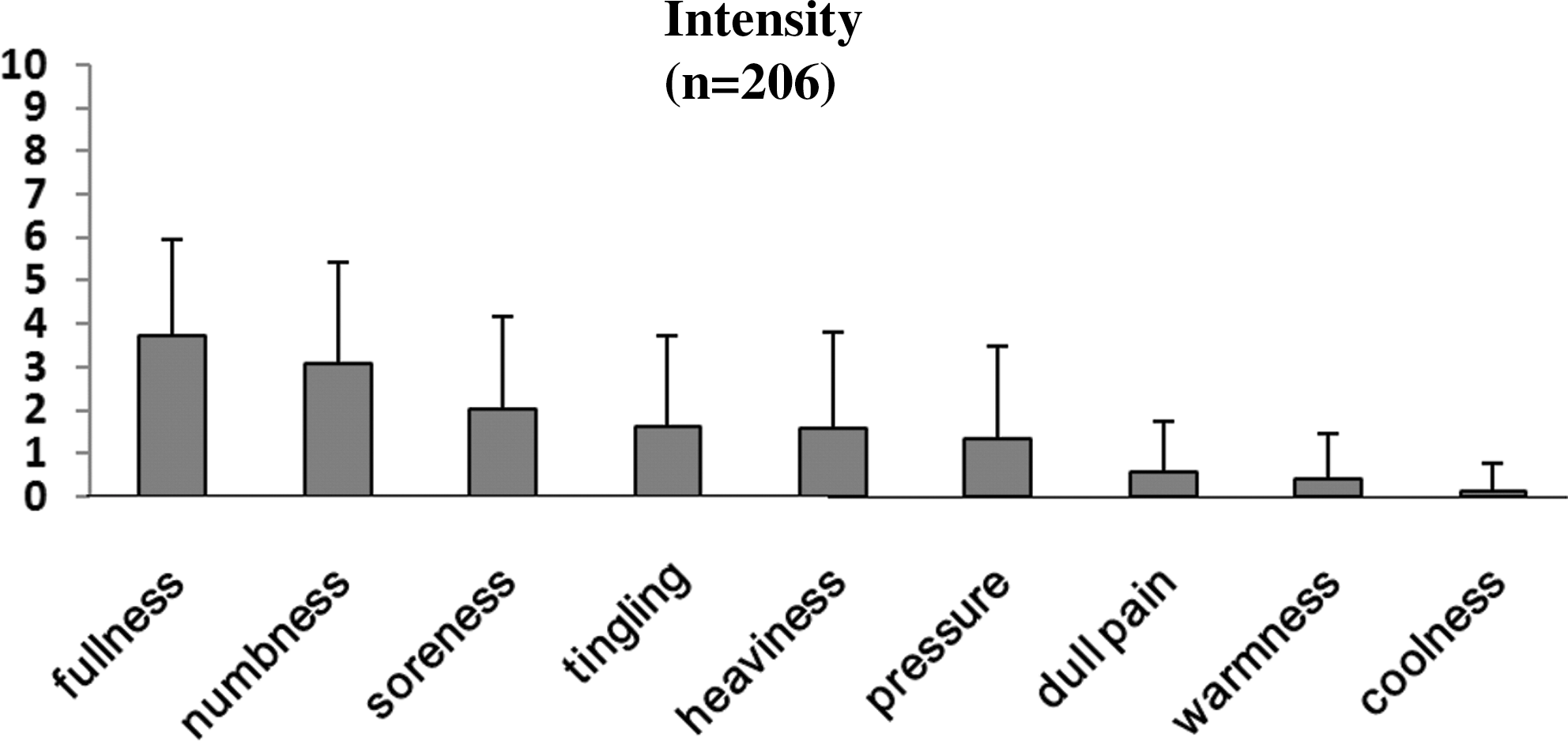
Intensity of various needling sensations in de qi. 0 indicates no feeling, and 10 indicates unbearable sensation.
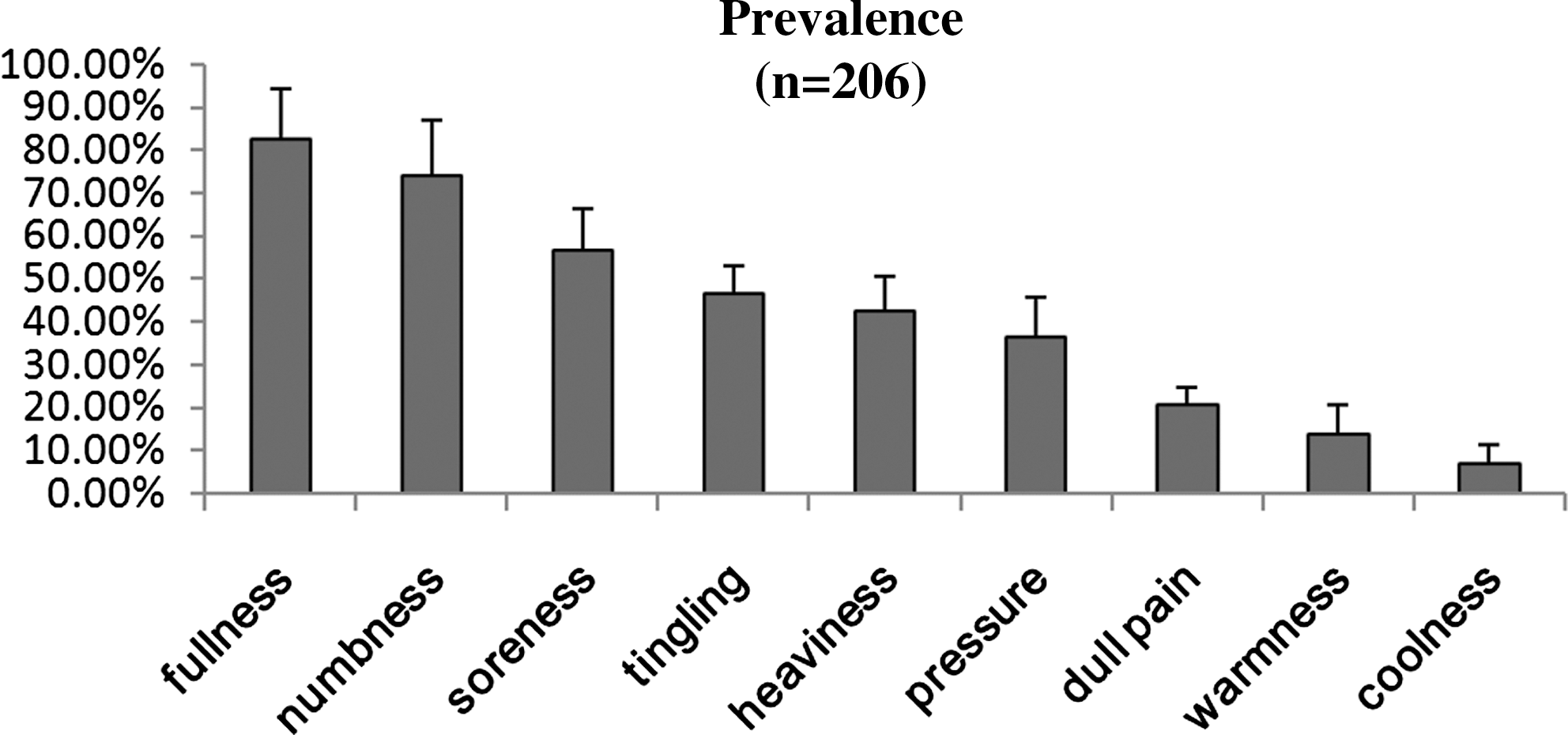
Prevalence of various needling sensations in de qi. 100% indicates that the individual sensation occurs in all acupuncture procedures and in all subjects.
Among 206 acupuncture procedures, sensation transmission occurred 168 (77.78%) times, and the average score for sensation transmission was 1.87±1.15 (mean±standard error [SE]), indicating that sensations mostly propagated over one joint; the average amplitude of electric current was 2.35±0.07 mA (mean±SE). No significant difference was found within each paired acupoints for sensation transmission and the amplitude of electric current.
Prevalence of individual sensations in paired acupoints
The prevalence of each individual sensation varies, and no significant difference was found between paired acupoints. However, it was noted that tingling sensation occurred more often than heaviness and pressure during EA at PC6 and PC7, ST36 (paired with CV4), whereas the frequency of tingling, heaviness, and pressure was similar in other acupoints. In this study, ST36 was paired with three different acupoints (GB34, CV4, and ST28). Interestingly, only when ST36 was paired with CV4, participants reported more frequent tingling sensation than heaviness and pressure (Table 1, Fig. 4).
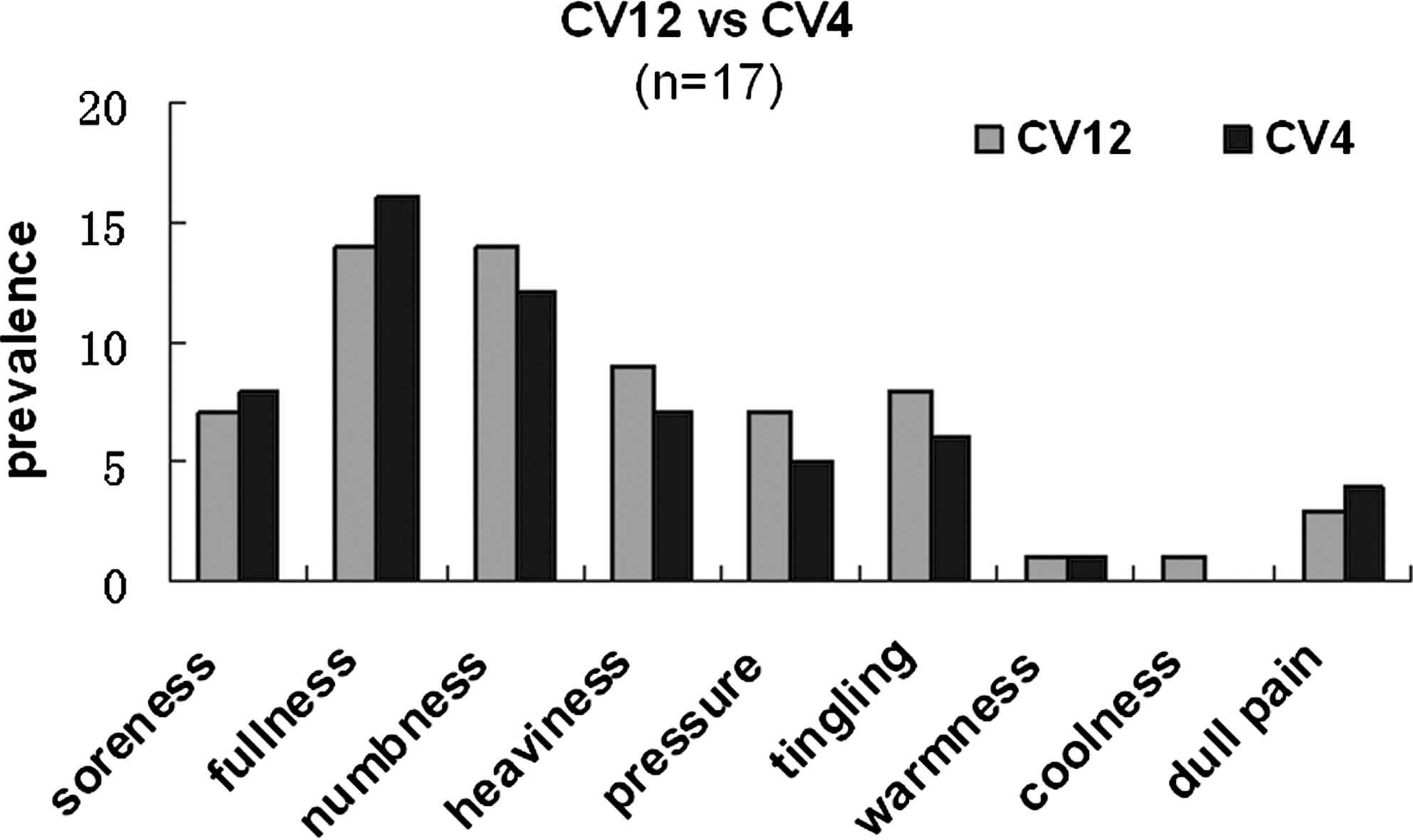
The bars indicate that among these 17 volunteers, the number of volunteers experienced the corresponding individual sensation in the study. Numbers in left axis represent numbers of volunteers.
Paired χ2 test was used, and no significant difference was found within paired acupoints; statistical difference was set at p<0.05.
Intensity of individual sensations within paired acupoints
The intensity of each individual sensation varies. Significant differences (p<0.05) were found in soreness, fullness, and heaviness between ST36 and ST28, in fullness and numbness between ST36 and CV4, and in fullness between CV4 and CV12. Tingling in PC6–PC7 and ST36 (paired with CV4) was stronger than heaviness and pressure, whereas similar intensities of tingling, heaviness, and pressure was shown between other paired acupoints. In this study, ST36 was paired with three different acupoints, and CV4 was paired with two different acupoints; however, the phenomenon of stronger sensation of tingling than heaviness or pressure was only noticed in ST36 as paired with CV4 (Table 2, Figs. 5 –7).

Intensity of individual sensation in paired acupoints CV12 versus CV4. Paired t test was used, and statistical difference was set at p<0.05 (*indicates significant difference).

Intensity of individual sensation in paired acupoints ST36 versus CV4. Paired t test was used, and statistical difference was set at p<0.05 (*indicates significant difference).

Intensity of individual sensation in paired acupoints ST36 versus ST28. Paired t test was used, and statistical difference was set at p<0.05 (*indicates significant difference).
Paired t test was used. a p=0.03, b p<0.01, c p=0.02, and d p=0.01.
SE, standard error.
Discussion
From a psychophysical perspective, needling sensation upon acupuncture de qi is a special compound sensation that consists of many individual components, such as soreness, numbness, fullness, and heaviness. 9,12 In this EA study using seven different acupoints, similar results were found in the prevalence and intensity of each individual sensation. Among these nine individual sensations, fullness, numbness, and soreness occurred more frequently and showed greater intensities, followed by pressure, heaviness, and tingling in a decreasing manner; whereas dull pain, warmness and coolness have a low occurring frequency and small intensity. Among these five paired groups of acupoints, ST36 was used three times and CV4 was used twice. In addition to the higher prevalence of tingling than heaviness and pressure noticed in ST36 as paired with CV4, prevalence and intensity were relatively similar for the same acupoint in different EA sessions, which indicates that acupuncture manipulation techniques used and subjects' psychophysical responses were relatively stable in this study.
In a study with manual acupuncture, Hui et al. 9 found that the prevalence and intensity of individual sensation was in a sequence from highest to lowest as follows: soreness, tingling, numbness, and dull pain; whereas warmness and coolness occur less frequently. Partially consistent results were found in this study; for example, soreness has a high prevalence and intensity, and warmness and coolness occurred less frequently with small intensity. However, differences also exist; for example, in this study, pressure and numbness occurred frequently with high intensities; fullness and numbness have higher prevalence and greater intensity than pressure and tingling. These differences may be caused by different needling methods (manual acupuncture versus EA), and it has been partially confirmed. Kong et al. 13 and Napadow et al. 14 found that EA had different modulatory effects in the brain cortex from those by manual acupuncture, and Leung et al. 16 found that “aching” was the predominant de qi sensation deriving from manual acupuncture, whereas “tingling” was the predominant de qi sensation deriving from EA. In addition, Mao et al. 8 found that the most common types of needling sensations reported by subjects were distended (94%), sore (81%), electric (81%), and numb (78%); in a study with 1095 subjects, Park et al. 6 found that distension (30.4%), soreness (4.7%), pulling (2.0%), heaviness (1.6%), tingling (1.5%), and numbness (0.9%) occurred during acupuncture procedures. Distension, which is similar to the fullness sensation in the present study, together with soreness both occurred relatively often in these two studies and the current study. Although both the study by Mao et al. 8 and the study by Park et al. 6 did not mention whether EA or manual acupuncture was used in their study, the overlapping of high prevalence of distension and soreness may indicate that people may respond with more fullness and soreness upon acupuncture procedures.
In this study, no significant difference was found in the prevalence and the amplitude of electric current upon de qi between each acupoint of each paired group, whereas significant differences (p<0.05) were found in the intensity of fullness between ST36 and CV4, CV4 and CV12, and ST36 and ST28, in the intensity of fullness and numbness between ST36 and CV4, and in the intensity of soreness, fullness, and heaviness between ST36 and ST28. As indicated in the study design, paired acupoints have different nerve innervations, especially for the groups of ST36-ST28 and CV4-CV12. Acupoints in these two groups share the same meridian category and tissue structure, but vary in nerve innervations. ST36 is innervated by L3/4; ST28 is innervated by T12; CV12 is innervated by T7/8. Meanwhile, needling methods were the same and no significant difference was found in the amplitude of electric current upon de qi. Therefore, the differences in the intensity of EA upon de qi may be caused by different nerve innervations. A further reflection on ST36 and CV4 reveals that besides different nerve innervations (ST36 is innervated by L3/4, and CV4 is innervated by T12), they have different meridian categories and tissue structures. Therefore, it is conjectured that the difference in sensation intensities is more related to different nerve innervations. Within paired groups, ST36 had greater sensation intensities than ST28 and CV4, and CV4 had greater sensation intensity than CV12. These results indicate that de qi sensation can be predominantly induced on EA at ST36 and CV4. Whether this inclination is related to the broad clinical use and multiple effects of ST36 and CV4 in clinical practice deserves further study, with which it will be possible to supply further research evidence for the relative specificity of different acupoints in clinical practice.
The hypothesis that these differences may be caused by different nerve innervations is consistent with recent electrophysiologic studies. Distension, heaviness, aching, soreness, warmness, and dull pain are conveyed by the slower-conducting Aδ and C fibers, whereas numbness is conveyed by the faster-conducting Aβ fibers, 17 –19 and pressure is transmitted through multiple different types of nerve fibers. Meanwhile, nerve innervations and tissue structures are actually closely interrelated to each other; for example, tendinomuscular layers have more Aδ and C fibers distribution. 20,21 In addition, Langevin et al. 22 found that mechanical signal to connective tissue and the winding of tissue around needle are essential factors associated with needling sensations upon acupuncture de qi, and researchers in Shanghai reported that needling sensations were characterized as fullness at muscle tissue and as stabbing pain at vascular tissue. 21
Furthermore, in this study, sensation transmission occurs frequently (77.78%) in participants, a result that is close to that of the study (89%) by Mao et al. 8 Sensation transmission is usually described by acupuncture practitioners and researchers as “propagated sensation along meridians (Xun Jing Gan Chuan)” or even as “qi's arrival at pathological sites (Qi Zhi Bing Suo).” Since 1950, when a Japanese scholar reported the phenomenon of sensation transmission, 23 a large number of studies have been carried out to test the existence and characteristics of sensation transmission. 24,25 Li et al. 26 have done a series of studies in China and report that “propagated sensation along meridians” exists on people and have characteristics such as tendency to follow meridians, tendency to travel toward pathological sites, and bidirectional propagation. The results of this study further substantiate that the existence of sensation transmission upon acupuncture de qi and sensation transmission can be used as an evaluation criterion for acupuncture de qi, which is essential to the therapeutic effectiveness of acupuncture.
Nevertheless, this study was performed on only seven different acupoints of 21 healthy volunteers at only one TCM hospital in China; therefore, the result of this study may not well characterize the general response of patients with different disorders with needling at one specific acupoint. Furthermore, sensation transmission was subjectively reported by volunteers through their feelings rather than objectively measured in biological parameter changes as other researchers did. 26 Given that acupuncture, especially EA, is becoming more popular, in order to better characterize patients' de qi response at clinical settings upon acupuncture needling with electric current added, further studies on a large sample of patients at different medical centers are warranted.
Conclusions
With similar individual sensation prevalence and electric current, the significant intensity differences of individual sensations between different acupoints may be caused by different nerve innervations. Among these sensations associated with EA stimulation, fullness, numbness, and soreness were the most common and obvious, followed by heaviness, pressure, tingling, warmness, coolness, and dull pain.
Footnotes
Acknowledgments
This study was funded by National Institutes of Health (National Center for Complementary and Alternative Medicine, F05 AT003022-03-04), United States, the National Natural Science Foundation of China (Grant Number: 30870668), and the internal funding of Guang An Men Hospital (2006).
Disclosure Statement
No competing financial interests exist.