
Abstract
Objectives
Design:
The PubMed, Embase, and Allied and Complementary Medicine databases were searched to identify Ayurvedic clinical trials published from 1980 to 2009. A total of 45 Ayurvedic clinical trials were identified and grouped into two time periods: pre- and post-2000 periods. Each article was independently reviewed by two calibrated reviewers.
Results:
Analysis revealed that not 1 of these 45 studies, in either time period, reported “only-and-full” use of the 23 available Ayurvedic diagnostic criteria. In fact, 24.4% of these 45 articles never specified any diagnostic criteria at all. While the percentage of articles using Ayurvedic diagnostic criteria (either as “only use” or “combined use with Western Medicine diagnostic criteria”) doubled over the two time periods (27.7% to 59%), rarely were more than 2 of the 23 Ayurvedic diagnostic criteria ever used.
Conclusions:
To improve confidence in their findings, future studies should strive to correct this observed inappropriate and gross underuse of Ayurvedic diagnostic criteria in the designing of clinical studies that aim to rigorously test the effectiveness of Ayurvedic treatments.
Introduction
Ayurveda is based upon basic beliefs about health and disease. According to Ayurvedic principles, all living and nonliving things are made up of five basic elements: Kha (space), Vayu (air), Agni (fire), Jal (water), and Prithvi (earth). 2 These five elements combine and manifest in the human body as three humors (Doshas), known as Vatta, Pitta, and Kapha. 2 All the biologic, psychologic, and pathophysiologic functions are controlled by these three humors (Doshas), and any imbalance in these Doshas (also referred to collectively as the Tridosha) will be the cause of illness. 2 The second most important aspect of Ayurvedic treatment is a person's body constitution, known as Prakirti. The Prakirti is thought to be a unique combination of physical and psychologic characteristics that govern the way the body functions. It could be described as the temperament or the psychosomatic character of the individual. 3 There are seven types of Prakirti, depending upon which Dosha, or combination of Doshas, dominate. 4 The Ayurvedic physician takes body constitution and imbalance among Doshas into diagnostic consideration when treating a patient. 2
As shown in Figure 1, Ayurvedic physicians have to follow a specific three-part diagnostic approach that markedly differs from the diagnostic approach of modern (Western) medical science. A proper patient examination includes assessing Dashavidha Rogi Pariksha (via the tenfold patient examination) and Ashtavidha Rogi Pariksha (via the eightfold patient examination) while a proper disease examination includes Roga Pariksha (via the fivefold disease examination). Ayurvedic physicians make diagnoses based on the information, collected through these examinations (i.e., Prakirti, Vikriti, level of Doshas, Samprapti (stage of disease), Dhatu and Mala imbalance). Besides other issues, these examinations are done to evaluate both the levels of the Tridosha (Vatta, Pitta, and Kapha) and the influence of Prakirti as necessary factors to arrive at an accurate and proper Ayurvedic diagnosis and treatment planning. The brief description/definitions for all the components of the tenfold patient examination are presented in Table 1 and for all the components of the eightfold and fivefold diagnostic criteria are presented in the boxes inserted in Figures 4 and 5, respectively.
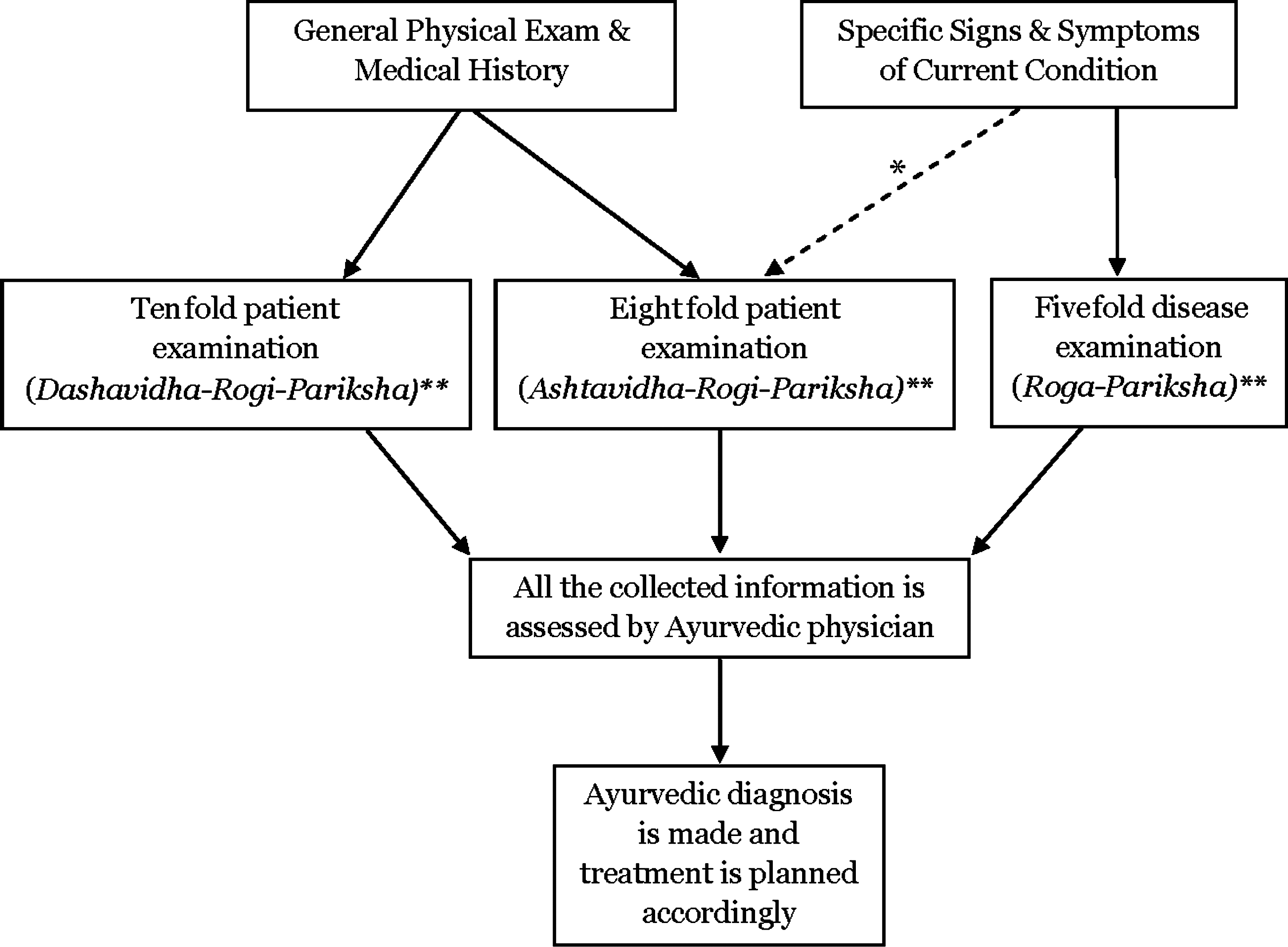
Ayurvedic diagnosis and treatment planning: Flow chart. *Weakly evaluated by “eightfold” examination (primarily evaluated by “fivefold” examination). **Brief definitions/descriptions for “tenfold” examination are presented in Table 1, and for “eightfold” and “five-fold” examinations are presented in boxes inserted in Figure 4 and Figure 5, respectively.
Ayurvedic treatment routinely uses herbs as remedies, but also includes prescriptions for lifestyle regimens such as diet, exercise, meditation, and massage. The use of herbs is an important part of Ayurvedic treatment, and there is a growing worldwide interest in Ayurvedic herbal drugs. However, the vast majority of the existing evidence of the effectiveness of these Ayurvedic remedies lies primarily in the written source of ancient Ayurvedic texts (i.e., the texts of Charaka, Shushruta, and Bhela [150 BCE–500 CE]), rather than on a body of findings from rigorously conducted clinical trials. This is not surprising, as the development of today's clinical trials is not only a relatively modern means for evaluating the efficacy of comparative medical treatments (i.e., become the “gold standard” for evaluating medical treatments in the mid-20th century) but also it is clearly evolved from and within Western-based scientific thought, principles, and practices. 5
In the current globalization of people, cultures, and specific cultural practices, it is inevitable that the ancient medical system of Ayurveda would not only meet the modern Western practice of medicine, but also that Ayurvedic medicine would inevitably have the efficacy of its treatments tested within the research framework of the Western clinical trial. This report focuses on one critical element of the intersection of these two “medical worlds”: namely, when Ayurvedic treatments are studied in Western medicine–style clinical trials, are the subjects in these studies appropriately diagnosed using the full set of Ayurvedic diagnostic criteria, or are the subjects in these studies of Ayurvedic treatments less appropriately diagnosed using Western medical criteria? To the extent that the latter situation occurs, it would raise methodological concerns about the possible—if not likely—misclassification of subjects as regards the appropriateness of the treatments provided, and hence, draw into question the validity of the findings of the clinical studies. If diagnostic misclassification occurred routinely, it would raise serious questions about the validity of the collective findings from this growing body of clinical trials on Ayurvedic interventions/treatments. This situation is much like acupuncture, which has been used by Chinese healers for at least 2000 years to treat pain and other ailments, gradually gained popularity all over the world, and tested within research frameworks in the Western world, but its supporters say “it is difficult to apply Western research standards to an ancient healing art.” 6
Specifically, this literature review presents findings on the extent to which Ayurvedic clinical trials performed over the past 30 years, both within Asian and Western countries, appropriately used Ayurvedic diagnostic criteria (either for eligibility criteria or to ensure balanced assignment to treatment groups) in Ayurvedic clinical trials that assessed the efficacy of Ayurvedic interventions/treatments (i.e., this study assesses the potential for subject misclassification within these Ayurvedic clinical trials). Additionally, this literature review discusses the possible impact of these methodological findings on the validity and interpretation of the body of these Ayurvedic clinical trials.
Materials and Methods
The collaborative team of this review, all based within the Department of epidemiology and health promotion at New York University's College of Dentistry, was composed of an Ayurvedic physician (BSB) who was also a graduate student in the MS in Clinical Research Program, an epidemiologist (RVK), an adjunct assistant professor (RM), and 3 other MS in Clinical Research graduate students (VMHS, RC, and BAD), 2 of whom formerly were health care providers (dentists) from India. The comprehensive literature search was conducted by a biomedical research librarian (RM) at New York University in the PubMed, Embase, and Allied and Complementary Medicine (AMED) databases. The search consisted of the key words and subject headings
Data were abstracted from each article using a uniform data abstraction form that consisted of items related to Ayurvedic and Western medicine diagnostic criteria. The form first guided abstractors into the collection of data on eight general observations about the clinical trials: (1) the title; (2) the author names; (3) publication date of the article; (4) the length of the follow-up observation period; (5) number of subjects in the study; (6) confirmation that the study was a clinical trial; (7) whether random assignment of subjects to study groups is used in the clinical trial; and (8) a judgment of whether the diagnostic criteria were clearly described. Then the data abstraction form required data collection regarding identification of the specific Ayurvedic and Western medicine diagnostic terms used in each clinical trial. While there are a few other styles of grouping the Ayurvedic examinations (e.g., some Ayurvedic texts mention Trivida Pariksha [the threefold examination]), the authors directly used the individual diagnostic terms (i.e., Tridosha [Vatta, Pitta, and Kapha], Prakirti, Vikriti, Nadi Pariksha, Mala Pariksha, Nidana, Rupa, Samprapti) to be certain of noting the mention of these specific diagnostic terms. For each clinical trial, the abstractors identified terms related to diagnostic criteria, including (1) Dashavidha Rogi Pariksha, the tenfold patient examination (i.e., Prakirti, Vikriti, Sara, Samhana, Pramana, Vyayam Shakti, Satmya, Satava, Ahara Shakti, and Vaya); (2) Ashtavidha Rogi Pariksha, the eightfold patient examination (i.e., Akara Pariksha, Drika Pariksha, Shabada Pariksha, Jhiva Pariksha, Sparsha Pariksha, Mala Pariksha, Mutra Pariksha, and Nadi Pariksha); (3) Roga Pariksha, the fivefold disease examination (i.e., Nidana, Samprapti, Purvarupa, Rupa, and Upashaya-anupshya); (4) Tridosha (Vatta, Pitta, and Kapha); and (5) terms related to Western diagnostic criteria such as blood pressure, electrocardiogram, radiographs, computed tomography scan, magnetic resonance imaging, ultrasonography, lung function tests, and laboratory examinations including urine examination, stool examination, and an array of blood tests.
For most of the data abstraction items (including tenfold examination and Tridosha), responses were in the form of Yes (= mentioned)/No (= not mentioned) choices. Recognizing that the authors of these published 45 articles might have addressed Ayurvedic diagnostic criteria in a way that was written to be comprehensible for the Western medicine–based readers, and given that these parallel Western medicine terms might have been the only terms used in these published articles that are found within the eightfold and the fivefold examinations, the data abstraction form item responses accommodated by having four available choices: clearly mentioned in Ayurvedic terms, clearly mentioned in Western medicine terms, mentioned but not clearly specified as either Ayurvedic or Western medicine (e.g., “Pulse examination,” in Ayurveda, is performed to evaluate the level of Doshas, which is entirely different from the Western medicine approach), and not mentioned at all. Each of the 45 studies was systematically and independently reviewed by two reviewers. The Ayurvedic physician (BSB) reviewed all 45 articles and three other team members (VMHS, RC, and BAD), reviewed a nonoverlapping set of 15 randomly assigned articles. The data collected by the 2 reviewers for each article were compared for agreement, with differences resolved by direct reference to the article itself by the 2 assigned reviewers. A database was designed using Epidata 3.1 software to record all the information extracted from these 45 articles and then exported to SPSS Version 16 for data analysis. Figure 2 shows the stepwise details of the methods used in this literature review and analysis.
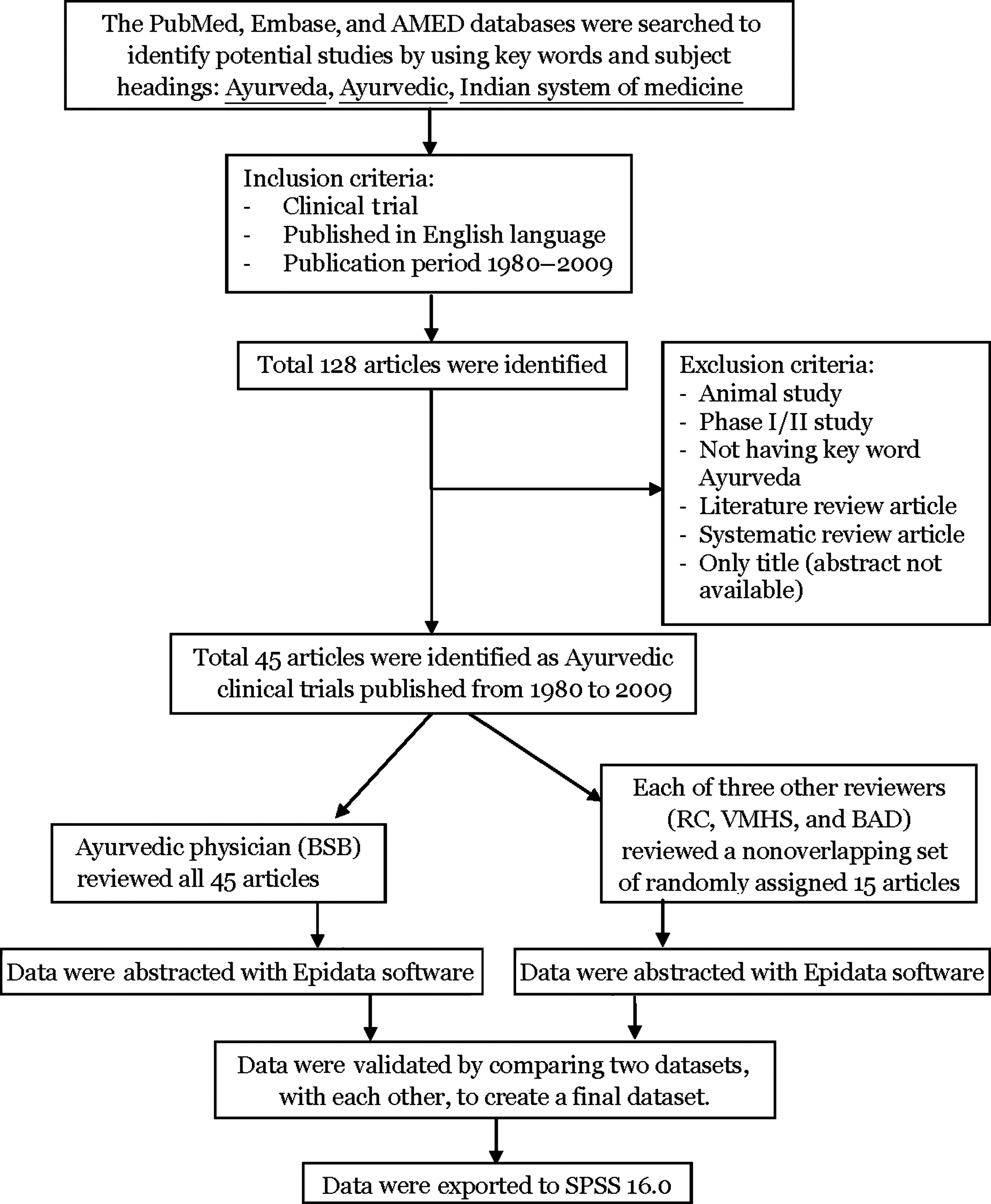
Literature search and data retrieval: Flow chart.
Results
The 45 published Ayurvedic clinical trials were unevenly distributed over the 3-decade observation period with 5% published in the 1980s, 35% published in the 1990s, and 60% published in the first decade of this century. For purposes of analysis, these 45 published Ayurvedic clinical trials were categorized as either pre-2000 (n=18) or post-2000 (n=27). As presented in Table 2, the post-2000 period notably had more clinical trials (27 versus 18), with a higher percentage being randomized clinical trials (74% versus 66.6%), and the studies were of longer duration (days) (i.e., 94.4±88.2 versus 61.8±53.9).
SD, standard deviation.
Figure 3 shows the mention of the 10-fold patient examination terms in the 45 Ayurvedic clinical trials by publication period, and reveals that there was over a twofold increase in the frequency of mention of at least one of the tenfold diagnostic criteria (i.e., in 59% of the post-2000 clinical trial articles). However, even in this post-2000 period, only one criterion of these 10 criteria of the tenfold patient examination was frequently mentioned, and that was Vaya (Age). Furthermore, any increase in “more” terms being mentioned in this latter time period was almost exclusively due to the one article that did mention all 10 criteria of “the tenfold examination.” More typically these post-2000 articles, as with the pre-2000 clinical trials, mentioned only Vaya (Age) as the sole diagnostic criteria.
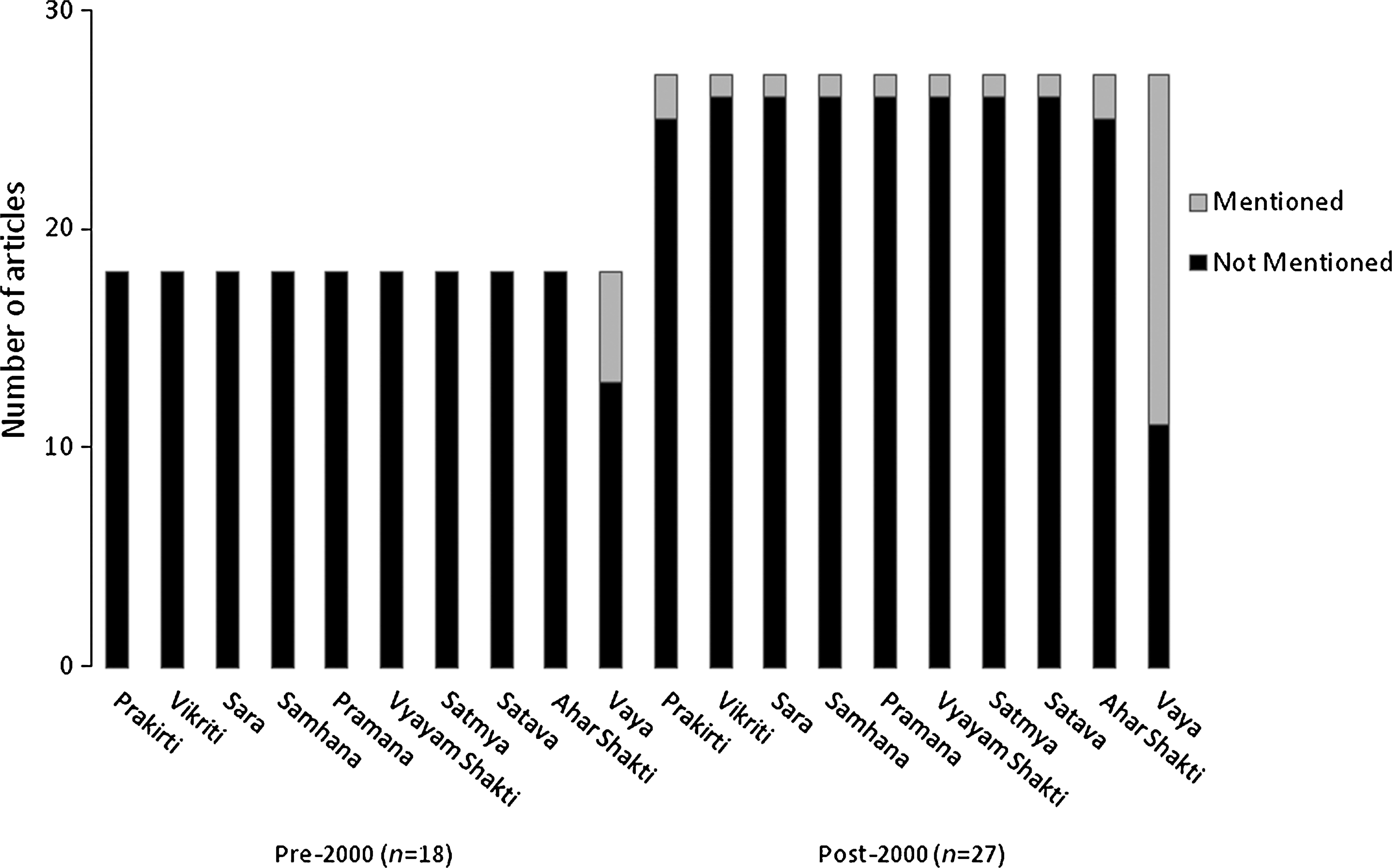
Tenfold patient examination in Ayurvedic clinical trials published pre-2000 versus post-2000. Definitions of these terms of tenfold patient examination are shown in Table 1.
Figure 4, which shows comparison of “eightfold” patient examination in Ayurvedic clinical trials by publication period, revealed that (1) none of the articles, either in the pre- or post-2000 publication periods, reported the use of any of the eightfold examination criteria specifically in Ayurvedic terms

Eightfold patient examination in Ayurvedic clinical trials published pre-2000 versus post-2000: Use of Ayurvedic versus Western medical terminology. *None of the articles reported any of the eight diagnostic criteria in Ayurvedic terms.
Figure 5 shows comparison of Roga Pariksha, the fivefold disease examination in the 45 Ayurvedic clinical trials by publication period, and revealed that at least two thirds of the articles in both publication periods did not report any of these fivefold diagnostic criteria at all, with the observed 66.6% in pre-2000 publication periods increasing to 74% in the post-2000 publication period. Conversely, the percentage of articles that reported at least one of these five criteria but did not specify whether the criteria were considered in Ayurvedic or Western medicine diagnostic terms increased by fourfold in the post-2000 publication period. Not one of the articles in pre- or post-2000 publication periods reported all of the “five” diagnostic criteria specifically in Ayurvedic terms.
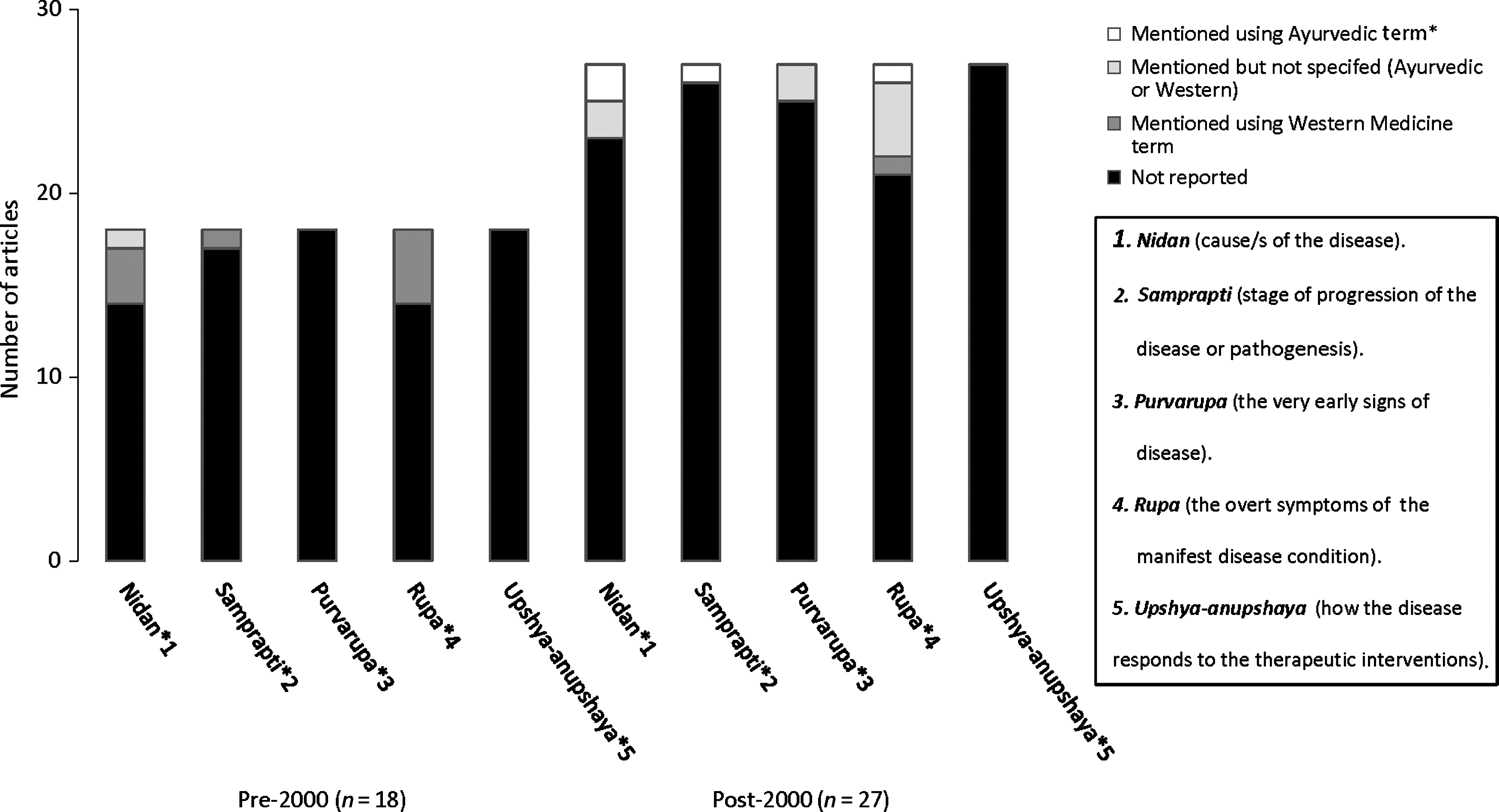
Fivefold disease examination in Ayurvedic clinical trials published pre-2000 and post-2000: Use of Ayurvedic versus Western medical terminology.
Figure 6, which shows the comparison of the use of Ayurvedic versus Western medicine diagnostic criteria by publication period, revealed a clear, if shallow, trend over time. Specifically, while the percentage of articles that mentioned Ayurvedic diagnostic criteria in the post-2000 publication period (55%) was two times more frequent than in the pre-2000 publication period, this observed increase in frequency of Ayurvedic criteria was due to the sole use of the one Ayurvedic diagnostic criteria Vaya (Age). Use of only Western medicine diagnostic terms was similar in both the pre- and post-2000 publication periods, slightly decreasing from 33.5% in the earlier period to 26.0% in the latter period. The number of articles that did not report any of the diagnostic criteria (neither in Ayurvedic nor in Western medicine diagnostic terms) was reduced to 15% in post-2000 publication period versus 39% in the pre-2000 publication period. Noteworthy was the fact that no article, either in the pre- or post-2000 publication periods, reported use of “ALL” the Ayurvedic diagnostic criteria (i.e., the ideal for an Ayurvedic clinical study).
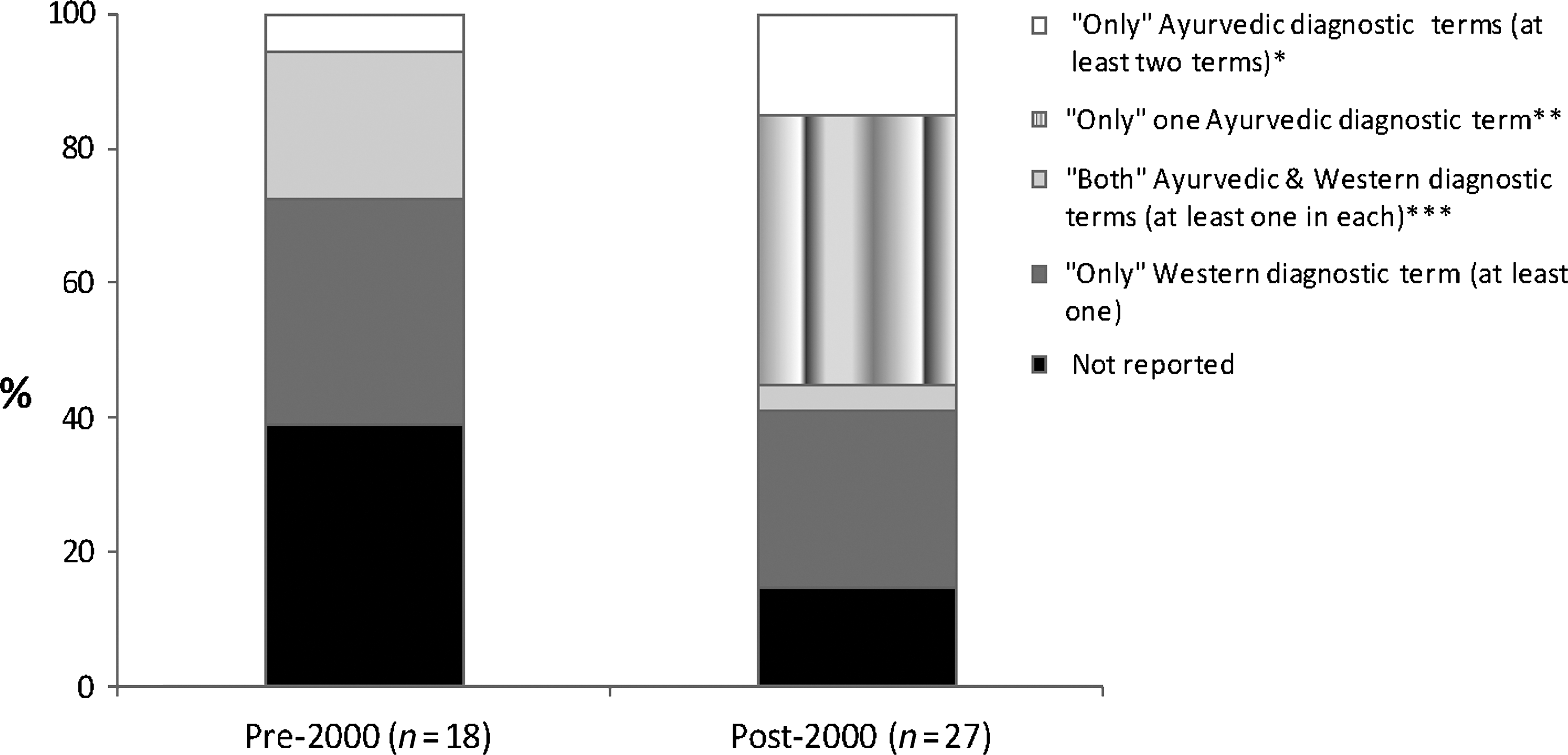
Comparison of “Ayurvedic” versus “Western” diagnostic criteria in Ayurvedic clinical trials published pre-2000 and post-2000. *“Only” Ayurvedic diagnostic terms (at least two terms); only one reported 10 and all other less than five of 23 Ayurvedic diagnostic terms that should have been used. **“Only” Ayurvedic diagnostic term (only one term); only single term was reported of 23 Ayurvedic diagnostic terms. ***Articles that reported both Ayurvedic and Western diagnostic terms (at least one term); not more than two Ayurvedic terms have been reported of 23 Ayurvedic diagnostic terms.
Discussion
The purpose of this literature review was to determine whether Ayurvedic or Western medicine diagnostic criteria had been used to categorize subjects in published Ayurvedic clinical trials over the past 30 years. The rationale for assessing whether Ayurvedic diagnostic criteria have been typically, if not always, used in the published body of clinical trials testing an Ayurvedic intervention lies in the concern for the validity of the findings of that body of published clinical trial literature, given that “diagnostic misclassification” of subjects would likely—if not most certainly—occur if Western medicine diagnostic criteria had been used when testing Ayurvedic interventions. In fact, only clinical trials that used Ayurvedic diagnostic criteria to categorize subjects, either alone or in combination with Western medicine system, would have been certain to avoid this misclassification. Hence, this review was undertaken to determine the extent to which our current knowledge of Ayurvedic treatment outcomes as based upon published Ayurvedic clinical trials might be flawed due to diagnostic misclassification of subjects resulting from the sole use of Western diagnostic criteria to classify patients when testing Ayurvedic interventions.
The number of published Ayurvedic clinical trials over the 30-year observation period increased markedly by decade (2 in the 1980s, 16 in the 1990s, and 27 in the 2000s), with a 50% increase in the number of the trials using Ayurvedic interventions in the post-2000 decade period (n=27) as compared to the pre-2000 2-decade period (n=18). This marked increase in published Ayurvedic clinical trials reflects the well-recognized growing awareness of, and interest in, complementary and alternative medicine over these 3 decades around the world. First, the plan was to compare the articles published in past 3 decades (1980–1989, 1990–1999, and 2000–2009). However, only two articles in the 1980–1989 period could be found, so it was decided to combine the first 2 decades, and articles were compared in two groups (i.e., pre-2000 and post-2000 publication periods).
Statistical analysis of the data abstracted from the articles revealed that there were no meaningful changes in trends in the pre-2000 publication period and post-2000 publication period regarding eightfold patient examination and fivefold disease examination. However, statistical analysis revealed that there was a 2+ increase in the number of articles that reported at least one diagnostic term of 10-fold patient examination (Dashavidha Rogi Pariksha) in the post-2000 publication period (59%) in comparison to the pre-2000 publication period (27.7%), and interestingly only Vaya (Age) was the most commonly specified criteria in this category. “Age” is a common concept that can be considered in both the Western as well as the Ayurvedic system of medicine, so it was difficult for the reviewers to judge whether this specific diagnostic criterion was mentioned in the Ayurvedic or Western aspect. Reviewers decided, unanimously, to assume Age (Vaya) as an Ayurvedic concept because all the articles that were reviewed were based on Ayurvedic interventions. It is also noteworthy that only one article, among all of the 45 articles, mentioned all of the 10 criteria of Dashavidha Rogi Pariksha (2.2%).
According to Ayurvedic principles, all of the biologic, psychologic, and patho-physiologic functions are controlled by Doshas (three humors: Vatta, Pitta, and Kapha) and any imbalance in these three Doshas (also referred to collectively as the Tridosha) will be the cause of illness. 2 The second most important aspect of Ayurvedic treatment is a person's body constitution, known as Prakirti. The Prakirti is thought to be a unique combination of physical and psychologic characteristics that governs the way the body functions. 3 Tridosha and Prakirti are two most important aspects of Ayurvedic treatment; these should never be ignored while considering an Ayurvedic intervention. But, interestingly, the percentage of articles that mentioned Tridosha was negligible (i.e., only 3.7% in the post-2000 publication period [n=27] and 11% in the pre-2000 publication period [n=18]). It was even worse for the Prakirti, as none of the articles in the pre-2000 publication period ever mentioned the term Prakirti (0%) and only two articles in the post-2000 publication period mentioned this term (7.4%).
According to Ayurveda, the treatment is very individualized: A specific Ayurvedic treatment for a specific disease will “only” be beneficial to a specific group of people who share same Prakirti (Body constitution): for example, Commiphora wightii (Guggal) is effective in the treatment of arthritis, and Ayurveda recommends specific formulations for patients with different Prakirtis: a Kapha Prakirti individual will respond to Yograj guggal, Hingwashtak churan, and Dashmool; a Pitta Prakirti person to castor oil and Sinhanad guggal; and a Vatta Prakirti person to Panchatiktaghruta guggal and Maharasandiquath (Gogte 2000). 3 This raises a further concern regarding generalization of the results of the clinical trials designed to test effectiveness of Ayurvedic interventions, which did not consider the Ayurvedic diagnostic criteria.
One possible limitation of this report and its findings might lie within the articles accessed in the comprehensive literature search, as conducted by a biomedical research librarian (RM) at New York University using the PubMed, Embase, and AMED databases. To the extent that these prominent literature search engines failed to capture any clinical trials reported in journals of Ayurveda published in India or other south Asian countries that were not indexed in any of these three specific database indices, the current findings might be biased in the direction of overstating the absence of use of Ayurvedic diagnostic techniques. However, given the vast number and the breadth of journals indexed in these three prominent electronic database indices, the influence of this potential bias is likely to be small as regards all published literature, and very likely to be zero as regards readers of Western medicine literature for whom these three indices serve as the standard for comprehensive literature searches.
In these 45 articles of “Ayurvedic Interventions Clinical Trials,” not a single article reported use of “Purely” Ayurvedic diagnostic criteria (0/45). Although a few articles reported some of the Ayurvedic diagnostic terms, it was not clearly stated in any of these articles whether the treatment assignment was, in fact, based on any of the Ayurvedic diagnostic criteria, so the reader was left to assume that this usual practice of using diagnostic criteria was essential to determine the eligibility of subjects for inclusion in the study.
Conclusions
Based upon a literature review of the 45 Ayurvedic clinical trials published in past 3 decades, despite their intent to test the effectiveness of Ayurvedic interventions, the findings of this literature review call into question the validity of the findings from these 45 Ayurvedic clinical trials due to the serious and near ubiquitously detected design flaw of possible subject misclassification due to the virtual lack of use of Ayurvedic diagnostic criteria. This design flaw would manifest in either eligibility criteria or in balanced subject assignment to treatment and control groups, both of which would impact on the interpretation, as well as on the implementation decisions, of study findings. Unfortunately, the time trend observations suggest only very modest improvements as regards this design flaw over the two time periods (i.e., it has not been “self-correcting” at an acceptable pace). Future studies should overtly strive to correct this inappropriate underuse of Ayurvedic diagnostic criteria in the designing of clinical studies that aim to rigorously test the effectiveness of Ayurvedic treatments.
Footnotes
Disclosure Statement
No competing financial interests exist.