
Abstract
Objectives:
The study examined differential autonomic nervous responses to acupuncture stimulation at the wood points ( ) and the metal points (
) and the metal points ( ) among the five-shu points of the Pericardium and Triple Energizer Meridian.
) among the five-shu points of the Pericardium and Triple Energizer Meridian.
Design:
This was a crossover study of different acupuncture points with randomized order.
Subjects:
The study subjects were 30 healthy female volunteers (22.8±2.6 years old).
Interventions:
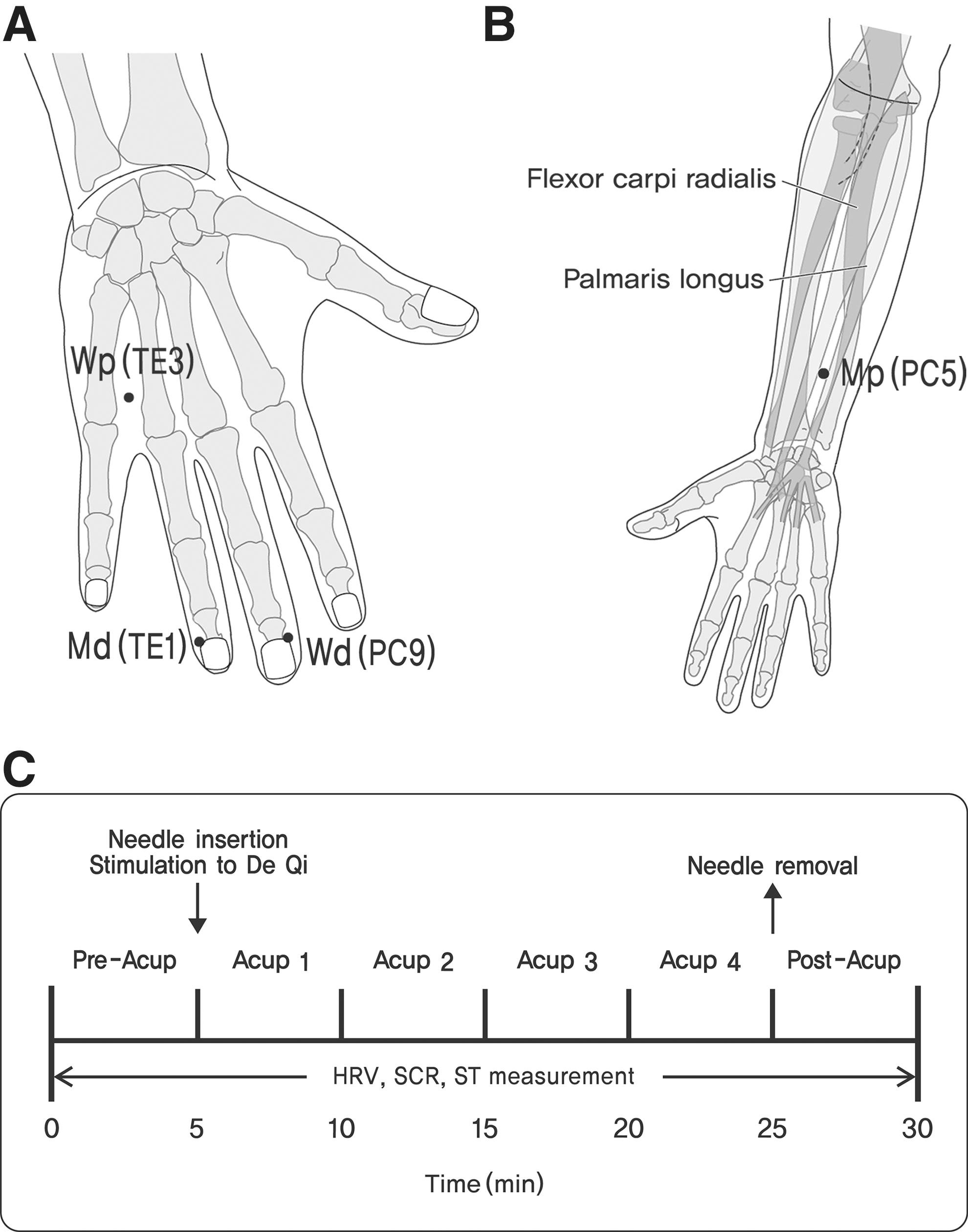
The acupuncture sessions were carried out over four sessions at 2–5-day intervals at the same time of day with one of the four acupoints: the wood distal point (Zhongchong, PC9), metal distal point (Zhongzhu, TE3), wood proximal point (Jianshi, PC5), and metal proximal point (Guanchong, TE1) on the left hand. After 5 minutes' rest (Pre-Acup), acupuncture needles were inserted, manipulated promptly, and were retained for 20 minutes followed by 5 minutes' rest (Post-Acup).
Main outcome measures:
Heart rate variability, skin conductance response, respiration rate, and peripheral skin temperature were measured.
Results:
For the normalized low-frequency band of heart rate variability, there was a statistically significant increase during Acup and Post-Acup at the PC9 and TE3 wood points compared with Pre-Acup. Statistically significant decreases for PC5 and TE1 were evident at the metal points. Skin conductance response and peripheral skin temperature, which are indicative of sympathetic activity and blood flow, respectively, were significantly induced at PC9 during Acup compared to Pre-Acup.
Conclusions:
The wood points PC9 and TE3 increase sympathetic activity; and the metal points TE1 and PC5 increase the parasympathetic activity. The effect of acupuncture on the autonomic nervous system differs between the wood and the metal points.
Introduction
According to the classical acupuncture theory, which originated from Huangdineijing Lingshu ( ), every channel and some of the acupoints on it have a certain property out of “yin and yang” and “five phases” respectively. The five-shu points are located in the peripheral part of each channel, distal to the elbow or knee: Jing (
), every channel and some of the acupoints on it have a certain property out of “yin and yang” and “five phases” respectively. The five-shu points are located in the peripheral part of each channel, distal to the elbow or knee: Jing ( ), Ying (
), Ying ( ), Shu (
), Shu ( ), Jing (
), Jing ( ), and He (
), and He ( ).
1,2
Each of the five-shu points corresponds to one of the five phases; the positions of the five phases are different on the Yin and the Yang channels though. On the Yang channel, the Jing points correspond to metal, one of five phases, while on the Yin channels, it corresponds to wood.
1,3
Some acupuncture therapies have been practiced based on this principle.
).
1,2
Each of the five-shu points corresponds to one of the five phases; the positions of the five phases are different on the Yin and the Yang channels though. On the Yang channel, the Jing points correspond to metal, one of five phases, while on the Yin channels, it corresponds to wood.
1,3
Some acupuncture therapies have been practiced based on this principle.
The five-shu points have various characteristics according to the properties of the distinctive five phases theory and have been widely utilized in acupuncture treatment, including Sa-Am acupuncture, which specifically use the five phase theory for the acupoint selection. 4 However, physiologic research with autonomic response concerning the distinctive characteristics of the five-shu points has not been done so far to our knowledge.
Also, many studies on acupuncture-mediated autonomic nerve modulation have yielded inconsistent results, depending on the type of points, the methods of stimulation, and the timing of physiologic measurement.
For heart rate variability (HRV), Haker et al. 5 reported that there was a statistically significant increase of low frequency (LF) and high frequency (HF) at LI4. Streitberger et al. 6 reported that there was a statistically significant increase of HF at LI4. Strudwick et al. 7 reported a decrease of HF and LF/HF ratio, but an increase of LF also at LI4. Chang et al. 8 reported an increase of LF/HF ratio at ST36. On the other hand, Won 9 reported a statistically significant increase of HF and a decrease of LF and LF/HF ratio after acupuncture at LI4 and LR3. For BL15, Hsu et al. 10 reported a statistically significant increase of normalized high frequency (HF norm), and a statistically significant decrease of normalized low frequency (LF norm). Lee et al. 11 reported an increase of HF norm and a decrease of LF norm and LF/HF ratio, although the changes were not statistically significant at BL15. Huang et al. 12 reported a statistically significant increase of HF norm following acupuncture at PC6. Shi et al. 13 reported no change of HF in the patients with coronary heart disease, but a statistically significant decrease of LF. Hsu et al. 14 reported an increase of HF and a decrease of LF after stimulating HN23 and Shenmen in auricular acupuncture points. Wang et al. 15 reported a similar phenomenon after acupuncture at HN23.
The aforementioned experiments were mostly based on the hypothesis that HF will increase and LF will decrease following acupuncture. However, according to the type of point and even with the same point, discordant results have been reported concerning the effect of acupuncture on HRV. It may due to partially different needling techniques, stimulation intensity, and time point of measurement such as during stimulation or after stimulation compared to before acupuncture. Skin conductance response (SCR) is a measure for exclusive sympathetic activation. Hsu et al. 10 reported that stimulation by electro-acupuncture at BL15 decreased SCR. For the skin temperature, Hsieh et al. 16 found that electro-acupuncture at ST36 lowered skin temperature (ST) due to the contraction of skin blood vessels, according to the stress response of sympathetic nerve. Increase of the sympathetic activity causes a lowering of peripheral skin temperature. 17
Accordingly, this research was conducted with the assumption that stimulation at different points would control the autonomic nervous system differently on HRV, SCR, and peripheral ST. The present research selected two wood and metal acupoints in the tip of the finger and two other wood and metal points in the hand and forearm to increase the contrast of needle sensation between the fingertips and other regions and to cover the same or neighboring dermatomes between two different kinds of acupoints (Fig. 1).
A factor considered for this selection was needle sensation. There are two different perspectives about the needle sensation. One is that the needle sensation is influential in the generation of acupuncture effects, while the other is that the needle sensation is not necessary or even an obstacle. For example, both Japanese acupuncture and some forms of sham acupuncture have shown considerable effects. All the acupoints on the tip of the fingers induce strong and pricking sensations. Therefore, an intentional choice was made in favor of these acupoints, which also have different properties of the five phases, wood and metal. Among the five phases, wood has properties of stimulus, growth, and extension; while metal has properties of sedation, suppression, and control. It is believed that wood increases Fire (Yang), whereas metal increases Water (Yin). Therefore, in general clinical settings, metal points are selected for the treatment of symptoms caused by the lack of Yin, while wood points are selected for symptoms caused by the lack of Yang.
Materials and Methods
Subjects
The research was conducted upon the approval of the Institutional Review Board of the Korean Medical Hospital of Sangji University. Thirty (30) females volunteers aged 20–29 years (mean age 22.8±2.6 years) participated in the experiment and were used for data analysis, while 2 subjects were excluded due to exclusion criteria and nonappearance at the second session. In order to reduce gender effect and age effect that can possibly affect the result of this research with a small subject group, only young female subjects were recruited. The subjects recruited by flier or Internet received a detailed explanation of the study and provided informed written consent for their participation. The medical history of each subject included disease history, age, height, weight, alcohol consumption, tobacco use, and medication history. To eliminate any influence on HRV and body temperature, subjects were excluded if they presented with a present or previous history of diseases such as stroke, psychologic disorders, heart disease including hyperpiesia and arrhythmia, and endocrine disorder. Subjects were also excluded if they had consumed alcohol, used a medicinal drug, or had overworked the day prior to the procedure.
Acupuncture procedure
Disposable, sterile, 0.25×30-mm stainless needles were used for acupuncture (Dongbang Acupuncture, Inc., Korea). The four acupuncture sessions were carried out over four sessions at 2–5-day intervals at the same time of day so that possible carryover effect might be removed. In each session, one of the four acupoints, the wood distal point (Wd, PC9), metal distal point (Md, TE3), wood proximal point (Wp, PC5), and metal proximal point (Mp, TE1) on the left hand was used. To eliminate order effects, the order of the four points was randomized. We employed a crossover design because this study with healthy subjects measured short-term autonomic nervous system (ANS) response other than clinical outcome measures of patients. After submitting a consent form, the subjects were seated in an armchair to rest for around 10 minutes. A needle was inserted after the baseline of another 5 minutes rest and was retained for 20 minutes before removal. Physiologic monitoring was done during the entire period and for 5 minutes following needle removal. During the entire 30 minutes of measurement, each participant was instructed to keep stable without any conversation. Also they were seated and were not prone to avoid excessive relaxation or sleeping, and were instructed not to close their eyes. The needle insertion at PC9 and TE1 was done to a depth of 2–3 mm, and at PC5 and TE3 to a depth of 8–10 mm; all insertions were at an angle of 45–60° with nine rotations for 3 seconds. In order to have the needle follow the direction of meridian flow, the needles were turned toward the distal and proximal directions in PC and TE meridian, respectively. 3 It took about 5 seconds in total for both acupuncture insertion and manipulation, and this procedure was started 5 seconds prior to the Acup1 period. Thus, throughout all the ACU periods (20 minutes, Acup1–4) the subjects were in the resting state with needle retained in an acupoint (Fig. 1).
Psychophysical data collection
To ascertain the amplitude of de qi experienced and the intensity of pain caused by acupuncture, the participants were asked to fill out the MGH Acupuncture Sensation Scale (MASS) questionnaire after each session. The MASS index, a weighted average based on formulas related to exponential smoothing with 12 sensation items, was developed for assessing acupuncture needle sensations by a research group in Massachusetts General Hospital (MGH). 18
Physiologic measurements
Electrocardiogram (ECG), skin conductance (SC), and skin temperature (ST) were measured using a physiologic monitoring device (Procomp Infiniti, Thought Technology Ltd., Canada). ECG electrodes, electrical SC electrodes, and a thermometer were attached to the inner side of both forearms and left lower leg, the right index finger and ring finger, and the right little finger, respectively. Heart rate variability was calculated sequentially from ECG data. SCR data in micro-Siemens (μS) were classified as tonic and phasic responses for the analysis.
In order to obtain the percent change in HRV, tonic SCR, and ST, the average values for the six 5-minute periods in each session were calculated based on the percentage of change from the initial baseline measurement (Pre-Acup). Also for the phasic SCR, average values of the last 30 seconds in the period of Pre-Acup (Pre-Stim) and the first 30 seconds in the period of Acup 1(Post-Stim) were compared. (Fig. 1.) SPSS/WIN 15.0 was used for the analysis of all the data. Paired t-test was used to compare the data obtained in six periods: before acupuncture (Pre-Acup), during acupuncture (Acup 1, 2, 3, 4), and after acupuncture (Post-Acup).
Results
Psychophysics
The MASS index based on the measurement of de qi experienced showed the following scores: 4.67±2.82 for PC9, 4.60±2.84 for TE1, 2.89±2.31 for PC5, and 3.65±2.91 for TE3. The score of PC5, which is a proximal point, was significantly low compared to the scores of the distal points, PC9 and TE1 (p<0.001) (Fig. 2) while another proximal point, TE3, only has a trend for a difference from the distal points (p=0.06 with PC9, p=0.09 with TE1). Also for sharp pain, PC9 (4.30±3.14) and TE1 (4.50±3.03) are different from PC5 (1.67±1.83) and TE3 (2.47±2.46) (p<0.01 for all the comparisons).
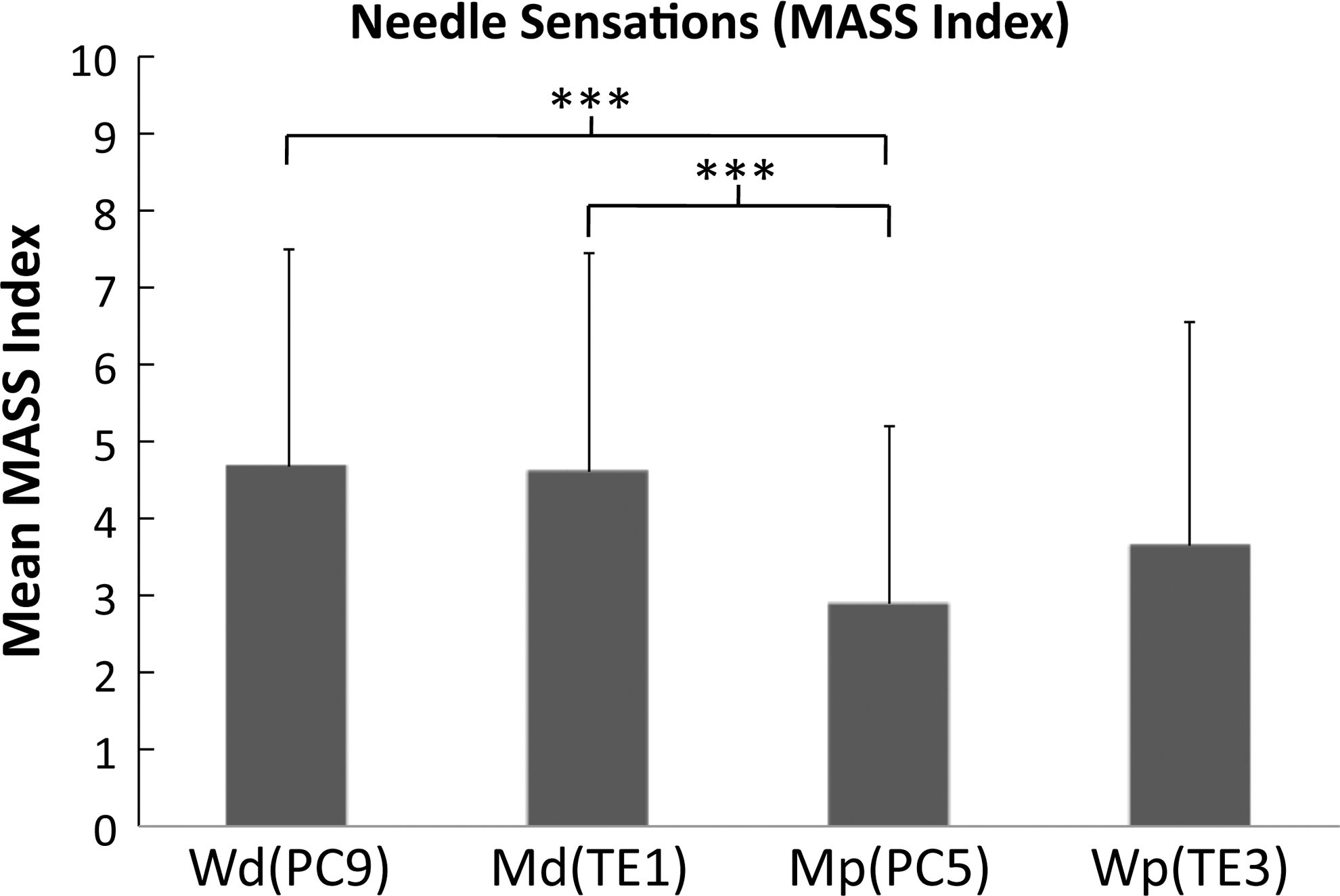
Results of psychophysics analysis. MASS index, a measure of de qi intensity, was greater for PC9 (a wood distal point) and TE1 (a metal distal point), compared to PC5 (a metal proximal point). (***p<0.001). Note that distal point, regardless of wood or metal point, induced stronger sensation than proximal point. MASS, Massachusetts General Hospital (MGH) Acupuncture Sensation Scale. Wd, Wood distal point; Md, Metal distal point; Wp, Wood proximal point; Mp, Metal proximal point.
HRV
For HRV, the wood points induced increasing sympathetic activity (LF norm) and decreasing parasympathetic activity (HF norm) and the metal points showed inverse trends. At the wood points, PC9 and TE3, LF norm displayed significant increase during Acup 1, Acup 2, Acup 3, Acup 4 and Post-Acup, compared with Pre-Acup (p<0.05) while at the metal points, PC5 and TE1, there were significant decreased LF norm during some of the needle-retained period and Post-Acup (p<0.05) (Table 1). Consequently, a statistically significant decrease was evident in HF norm at the wood points, PC9 and TE3, compared to Pre-Acup (p<0.05), while the metal points, PC5 and TE1 showed inverse trends (p<0.5) (Figs. 3 and 4, Table 1).
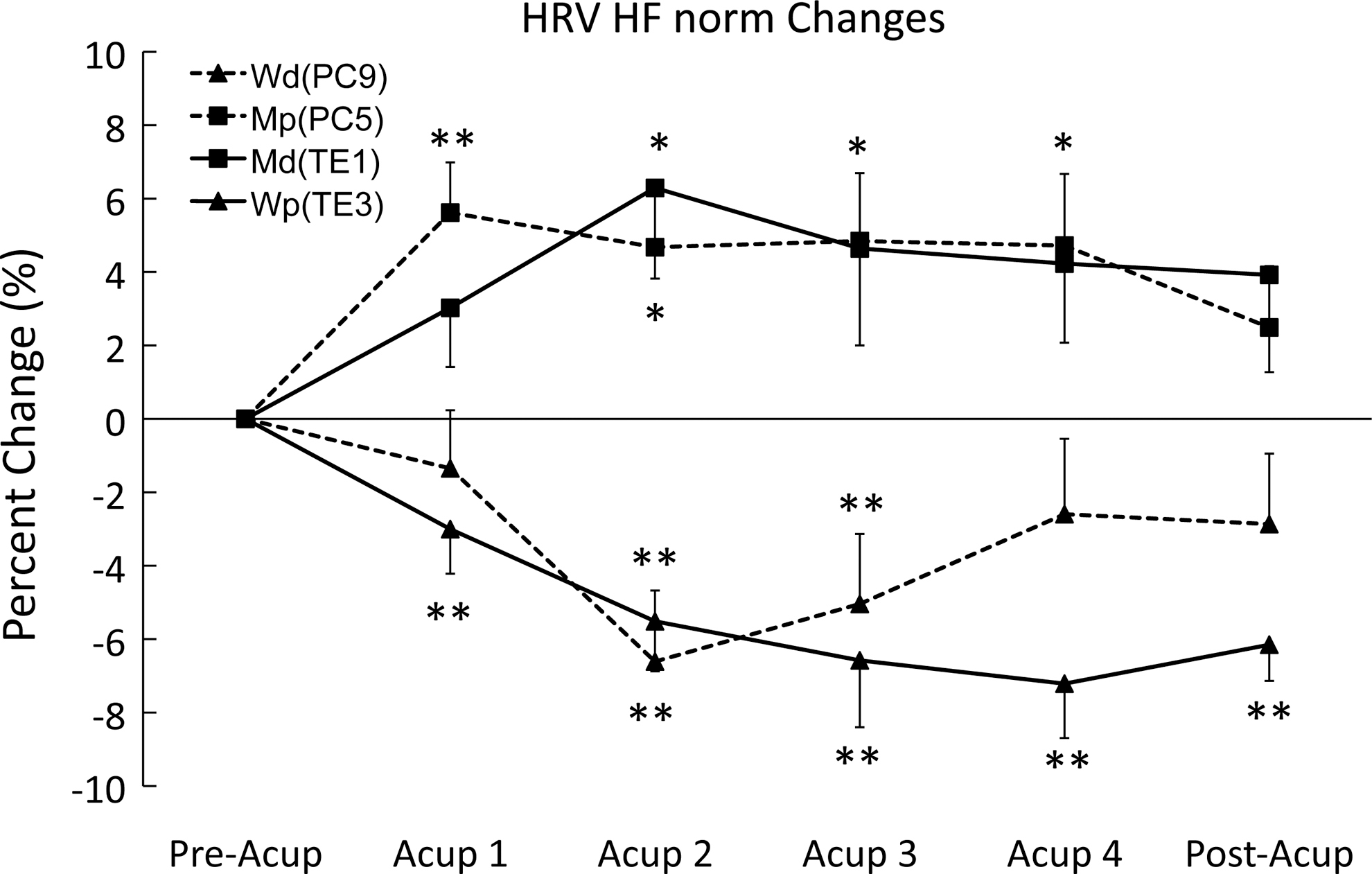
Change of high-frequency (HF) norm among preacupuncture (Pre-Acup), during acupuncture, and postacupuncture (Post-Acup) periods on PC9, TE1, PC5, and TE3. Paired t-tests were performed for the comparison between each period and Pre-Acup period (*p<0.05, **p<0.01). HF norm, normalized high-frequency power in heart rate variability (HRV).

Change of low-frequency (LF) norm among preacupuncture (Pre-Acup), during acupuncture, and postacupuncture (Post-Acup) periods on PC9, TE1, PC5, and TE3. Paired t-tests were performed for the comparison between each period and Pre-Acup period (*p<0.05, **p<0.01). LF norm, normalized low-frequency power in heart rate variability (HRV). Wd, Wood distal point; Md, Metal distal point; Wp, Wood proximal point; Mp, Metal proximal point.
HRV, heart rate variability; LF, power in low-frequency range; HF, power in high-frequency range; LF norm, LF power in normalized units (n.u.); HF norm, HF power in normalized units. SCR, skin conductance response; ST, peripheral skin temperature; Pre-Acup, preacupuncture; Acup 1, during 0–5 minutes after acupuncture stimulation; Acup 2: during 5–10 minutes after acupuncture stimulation; Acup 3, during 10–15 minutes after acupuncture stimulation; Acup 4, during 15–20 minutes after acupuncture stimulation; Post-Acup, postacupuncture. All the paired t-tests were performed for the comparison between each period and Pre-Acup period. Values represent mean±standard deviation.
p<0.05, ** p<0.01.
Values represent mean±standard deviation.
SCR: Phasic and tonic responses
SCR phasic responses at all the four points displayed statistically significant increases during the 30 seconds after needle stimulation compared to the 30 seconds before stimulation p<0.01) (Table 2).
Pre-stim, 30 seconds before acupuncture stimulation (the last 30 seconds in pre-acup); post-stim, 30 seconds after acupuncture stimulation (the first 30 seconds in Acup 1). Values represent mean±standard deviation. Unit: μS.
At PC9, a statistically significant increase of SCR appeared during Acup 1, Acup 2, Acup 3, and Acup 4, compared with Pre-Acup (p<0.05), while at TE3, there's an increase tendency at Post-Acup but not statistically significant. In contrast, there were no changes at the metal points, PC5 and TE1 (Fig. 5) (Table 1).

Change of SCR among preacupuncture (Pre-Acup), during acupuncture, and postacupuncture (Post-Acup) periods on PC9, TE1, PC5, and TE3. Paired t-tests were performed for the comparison between each period and Pre-Acup period (*p<0.05). SCR, skin conductance response. Wd, Wood distal point; Md, Metal distal point; Wp, Wood proximal point; Mp, Metal proximal point.
ST
A statistically significant increase in ST was evident at PC9, the wood point, during Acup 1, Acup 2, Acup 3, Acup 4, and Post-Acup, as compared with Pre-Acup (p<0.05), while other points did not induce skin temperature changes (Fig. 6, Table 1).

Change of ST at preacupuncture (Pre-Acup), during acupuncture, and postacupuncture (Post-Acup) for PC9, TE1, PC5 and TE3. Paired t-tests were performed for the comparison between each period and Pre-Acup period (*p<0.05). ST, peripheral skin temperature. Wd, Wood distal point; Md, Metal distal point; Wp, Wood proximal point; Mp, Metal proximal point.
Discussion
The present study tested five-shu points theory in terms of autonomic response to acupuncture. Two wood points, PC9 and TE3, and two metal points, TE1 and PC5, were employed. The guiding hypothesis was that one of the predominant factors for determining the property of a particular certain acupoint is the five phases theory, rather than the acupoint's location and related properties including induced needling sensation (i.e., tip of finger, hand, or forearm areas). For this purpose, acupuncture was conducted in healthy subjects at PC9 and TE3, which are the wood points of Yin Pericardium Meridian and Yang Triple Energizer Meridian, respectively, as well as at the metal points PC5 and TE1. For contrasting the acupoint properties, according to the five phases acupuncture theory, the wood and metal point were selected instead of the fire and water, which are more related to the contrast of yin and yang or activation and inhibition. It was due to the clinical convention that selects the wood and metal point to respectively activate Fire and Water qi in the human body. One example of this clinical practice is Saam acupuncture, which has been developed in Korea. Based on the HRV, SCR, and ST data, a comparative analysis was carried out to ascertain the difference between the periods prior to and during or following acupuncture. Also, to have more contrast between wood and metal points, the authors selected the two acupoints (TE1 and PC9) on the fingertips that have been believed to induce stronger needle sensation and consequently more sympathetic activation than other acupoints. As expected, the intensity of needling sensations is dependent on where the points are located. The distal points produced greater de qi sensation as well as sharp pain than the proximal points.
However, regardless of needle sensation, the needling at the wood points consistently induced sympathetic shift and parasympathetic drop for HRV and also sympathetic activation for tonic SCR and ST while the needling at the metal points induced parasympathetic increase and sympathetic decrease for HRV and no change for tonic SCR and ST. Here HRV results should be carefully interpreted because the appropriate selection among HRV parameters has been controversial. 19 In contrast, phasic SCR was evident in all of the points. This may indicate an orienting response to acupuncture needling. The orienting response is a physiologic response to any novel, moderate-intensity stimulus. 20
These results are likely to be attributed to the five-phase property of acupuncture points rather than to the point location, induced needling sensation, nerve innervation, and the meridian's yin–yang property. The MASS, needling sensation, is more influenced by point locations. The distal points produced stronger needling sensation than the proximal points. ANS responses to acupuncture are not consistent with either the MASS or point location. Also, any ANS response has no correlation with the needling sensation in the Pearson's correlation analysis. Furthermore, nerve innervation does not influence the difference of ANS response among points, as the points on the PC and TE meridian are innervated by the median nerve and ulnar nerve, respectively.
As a whole, the results of HRV, SCR, and ST showed differences that depended on the properties of the wood or metal points of the five phases, and not on distal or proximal locations of the points. The results may indicate that the wood points in five-shu points induce a sympathetic shift and a parasympathetic drop while the metal points showed inverse trends.
The study has certain limitations that prelude generalization to the entire five-shu points. Testing was done only on four acupoints for two of the five phases. Also, only young healthy female subjects were involved and autonomic outflows were used for the outcome measures. Results with patients may differ in various clinical settings. More studies with more various subject population will be required to ensure objectivity about the five-shu points of other meridian pathways, using more precise measuring methods to elucidate the properties of the five phases.
Conclusions
Acupuncture at the wood points PC9 and TE3 induced sympathetic activation and parasympathetic deactivation, while the metal points TE1 and PC5 modulated autonomic responses inversely. Therefore, the effect of acupuncture on the body is distinct between the wood and metal points among the five-shu points. It can be speculated that there is a connection between the two sets: the wood point, which has properties of growth and stimulus, and the sympathetic nerve, which functions in tensing the body. Also, it indicates a possibility of interference between the metal point, which has sedation and control as its properties, and parasympathetic nerves, which function in comforting or relaxing the body.
Footnotes
Acknowledgments
This research was supported by the Information Technology Research Center support program through the National IT Industry Promotion Agency funded by the Ministry of Knowledge Economy, Korea (NIPA-2012-(H0301-12-1004) and Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (KOSEF-2009-0076345).
Disclosure Statement
No financial conflicts exist.