
Abstract
Background:
Studies on alternative medicines for generalized anxiety disorder (GAD) are few. Manasamitra Vataka (an Ayurveda preparation) is explored for its efficacy in patients with GAD with comorbid generalized social phobia.
Materials and methods:
Seventy-two (72) patients with GAD with comorbid social phobia meeting DSM IV TR criteria, and who were between the ages of 20 and 55 of either sex, participated in the study. They were randomly divided into three treatment groups: Group 1 (n=24) and Group II (n=24) received Manasamitra Vataka tablets (100 mg twice daily for 30 days). Group II, in addition to Manasamitra Vataka, underwent Shirodhara (therapy involving dripping of medicated oil [Brahmi tail] over the forehead) treatment for the first 7 days. Group III (n=24) received clonazepam 0.75 mg daily in divided dose for 30 days. The assessment of the study was done using the Hamilton Anxiety Rating Scale, Beck Anxiety Inventory, Beck Depression Inventory, Epworth Sleepiness Scale (ESS), World Health Organization Quality of Life BREF, and Clinical Global Impression scales (Improvement and Efficacy).
Results:
Patients from all the groups showed significant reduction in clinical parameters evaluated. However, improvement in ESS was observed only in Group II. The treatment outcome was comparable between the three groups.
Conclusions:
This is the first study conducted on the efficacy of Manasamitra Vataka in anxiety disorders. The results suggest that Manasamitra Vataka is effective in the management GAD with comorbid generalized social phobia. Add-on effect of Shirodhara reduced the daytime sleepiness. Further studies on Manasamitra Vataka need to be carried out to judge its potential as a first-line treatment modality.
Introduction
Conventional medications for GAD/GAD with comorbid social phobia include benzodiazepines, selective serotonin reuptake inhibitors (SSRI), selective norepinephrine reuptake inhibitors (SNRI), and others. However, these pharmacologic agents have their own limitations and shortcomings such as dependence, tolerance, and adverse effects, compelling patients to increasingly seek help from alternative systems of medicine. An epidemiological study showed that 42% of the U.S. national population used alternative therapy in the previous year, 15 and this accounted for an increase of 34% when compared to a similar study conducted in the previous decade. 16 Accordingly, anxiety was found to be one of the strongest predictors (odds ratio 3:1; 95% confidence interval, 1.6–6.0) for the patients to use an alternative system of medicine. 17
Ayurveda, the Indian system of medicine, is one of the earliest documented health systems of the world, practiced for more than 4000 years. Manasamitra Vataka 18 is a well-known Ayurvedic medicine used as an anxiolytic in anxiety disorders by Ayurveda practitioners. Shirodhara therapy with oils such as Brahmi tail 19 (dripping of medicated oil over the forehead) is also widely used in psychiatric conditions, and this therapy has been demonstrated to be beneficial in state anxiety of healthy subjects. 20 Hence, there is need for validation of these forms of medications in anxiety disorders.
Methods
Aim and objective
The aim of this study was to evaluate the effect of Manasamitra Vataka on GAD with comorbid generalized social phobia.
The null hypothesis states that there is a difference in clinical outcome of Manasamitra Vataka on GAD with comorbid generalized social phobia when compared to the standard drug clonazepam.
The study was an open label, randomized, controlled, parallel group study.
Patients attending the outpatient Department of Psychiatry, National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore, India were recruited for the study. The CONSORT statement guidance was used to ensure the quality of the study. 21
Patients
Patients, between age 20 and 55 years, diagnosed as having GAD with comorbid social phobia as per DSM IV TR criteria by a psychiatrist and meeting Hamilton Anxiety Rating scale (HARS) >18, 22 were recruited for the study. Advertisements were placed in newspapers to facilitate recruitment. Patients with significant depression (Beck Depression Inventory [BDI] scores >17), any other Axis I and medical disorders, or on any psychotropic drugs 4 weeks prior to the study were excluded. Patients with substance abuse, and pregnant and lactating women were also excluded. The nature and design of the study were explained to patients, and informed consent was obtained. The study was approved by the Institute ethics committee.
Methods
Patients recruited were randomized using blocked randomization into one of the three groups. The scholars involved in randomization, distribution, and administration of study articles were independent from the investigators. During the study, patients were asked to adhere to the interventions given. However, participants were asked to report any medications taken or any treatment received during the intervention phase. Subjects were instructed to record any adverse effects after the commencement of interventions and to report back to the investigator at the earliest convenience. Intervention groups were as follows.
• Group I: Patients (n=24) received tablet Manasamitra Vataka 100 mg, twice daily, for 30 days. Manasamitra Vataka tablets were procured from Central Research Institute (Ayurveda), Cheruthuruthy, Kerala, a unit of Central Council for Research in Ayurveda & Siddha, Department of AYUSH, Ministry of Health & Family Welfare, Government of India, New Delhi. Dose was selected as per available literature. 18
• Group II: Patients (n=24) received Shirodhara for the first 7 days in addition to Manasamitra Vataka as mentioned above.
Shirodhara. 23,24
The Shirodhara treatment was administered in the morning (between 8:00
Shirodhara (dripping of liquid medicaments over forehead) procedure is described in brief below.
The patient was made to lie supine and relaxed on the Dhara table, a special wooden table designed for Shirodhara therapy. Brahmi taila (oil) is heated to 95°–100°F on a water bath and poured into a dhara patra, a specially designed vessel with a hole at the bottom that is placed 3 inches above the forehead of the patient lying supine on the dhara table. A steady stream of the oil was made to fall on the forehead of the patient in a specific pattern for 45 minutes. The eyes of the patients are covered with a piece of gauze so that the eyes are protected from accidental spilling of oil during the procedure. After the therapy, the patient was made to relax on the table for 30 minutes and was asked to take a head bath.
• Group III: Patients (n=24) received clonazepam (0.25 mg in morning and 0.50 mg at night) for 30 days. Clonazepam (Clonotril) was procured from the NIMHANS hospital pharmacy.
All patients were subjected to clinical evaluation on the 15th and 30th day of the treatment (Fig. 1).
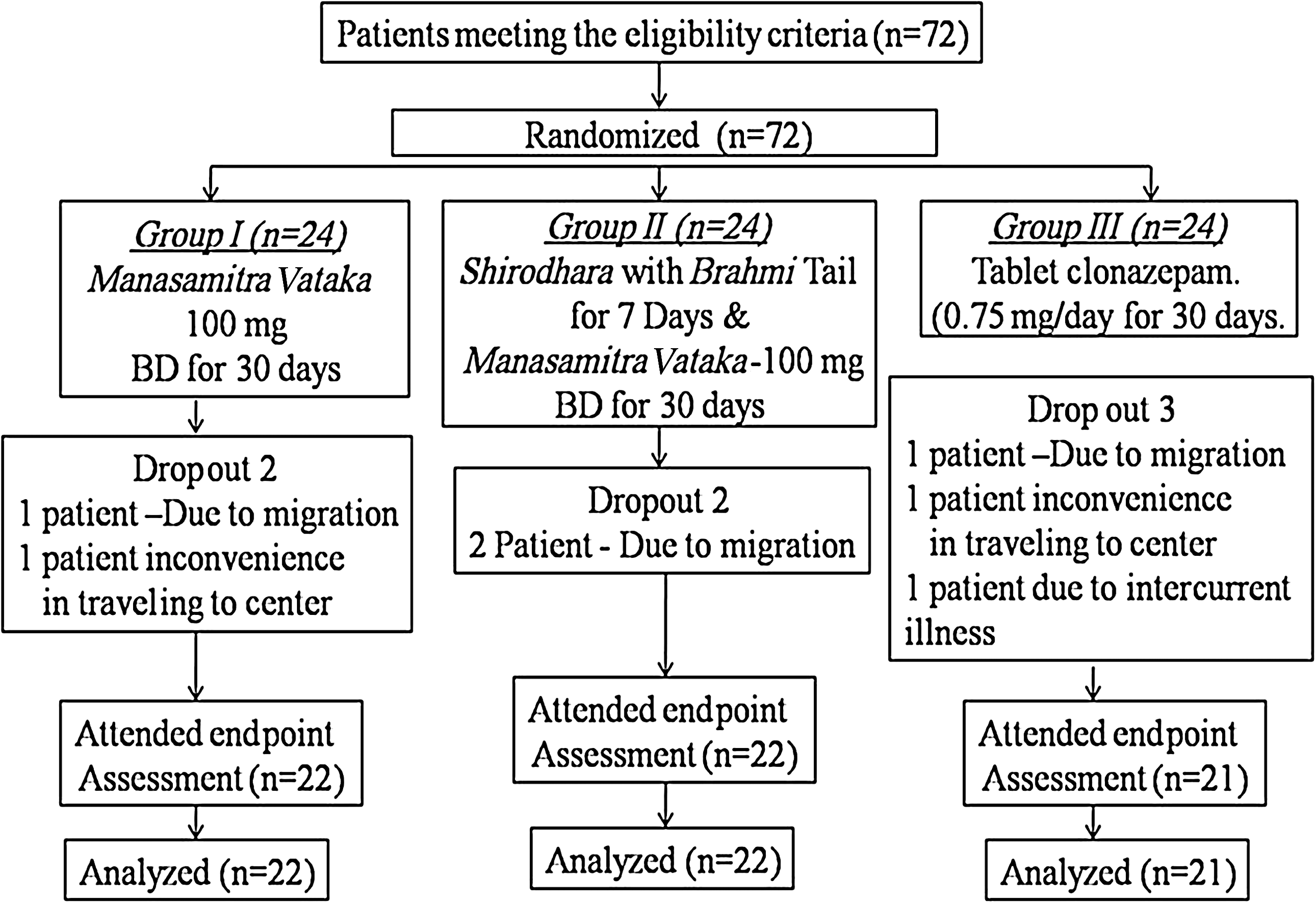
Subject flow chart through the study. BD, twice a day.
Assessments
HARS 22 and Beck Anxiety Inventory (BAI) 25 were used to assess anxiety. BDI 26 was used to exclude patients with significant depression and to measure mood disturbance during the course of intervention. Epworth Sleepiness Scale (ESS) 27 was used to evaluate the daytime sleepiness in the patients. World Health Organization Quality of Life Assessment Scale brief version (WHOQOL BREF) 28,29 was used to investigate the quality of life in patients. Quality of life was evaluated under the four different domains, namely, physical health, psychologic, social relationships, and environment. The Clinical Global Impression Scale (CGI) (severity, improvement, efficacy index) 30,31 was used to note severity and changes associated with the interventions. Ratings were done by a trained rater, and the self-report measure scales were completed by the patients.
Primary Outcome
The primary outcome was to note the changes in HARS, BAI, and CGI-Improvement (CGI-I). Response to treatment was defined as reduction of 50% or more in the HARS and BAI scales. Symptom remission was defined as HARS <8, BAI score <7, and CGI-I (very much and much improved) of 1 or 2 scores.
Secondary Outcome
The secondary outcome was to note changes in other scales such as BDI, ESS, WHOQOL-BREF, and CGI-Severity and efficacy index.
Statistical methods
Statistical analysis was carried out using SPSS Version 15.0. Homogeneity of the data across the groups was evaluated by the χ2 test. Comparison of groups across different time points was carried out by repeated-measure analysis of variance (ANOVA) with Tukey post-hoc test. Comparison of groups at baseline was analyzed by one-way ANOVA with Tukey post-hoc test. Effect size calculated by Partial Eta Square method was used to assess the effect of treatment through the outcome from baseline to 30th day of treatment. The criteria used for interpreting effect size measures were as follows: 0.2–0.3 as small, 0.3–0.5 as medium, and above 0.8 as large effect size. 32 Values are reported as mean±1 standard deviation. All tests were considered statistically significant at p<0.05.
Results
A total of 74 patients participated in the study. Seven (7) patients (Group I=2, Group II=2, and Group III=3) dropped out of the study due to migration (n=4), difficulty in traveling to NIMHANS (n=2), and intercurrent illness (typhoid) requiring stopping medication (n=1). No patients in either group discontinued due to adverse effects of treatment. Mild adverse and side-effects were noted with the interventions: 4 patients (2 patients from each Group I and II) reported mild abdominal colic for the first 5 days, which subsided without any intervention. Six (6) patients in Group III reported daytime sleepiness in the morning during the first week of medication. However, they reported no deficits in their daytime functioning.
Subject characteristics
The mean age (p=0.126), gender (p=0.518), occupation (p=0.405), socioeconomic status (p=0.250), education (p=0.913), and marital status (p=0.711) were comparable between groups (Table 1). Clinical variables such as height (p=0.674), weight (p=0.730), body–mass index (p=0.435), duration (p=0.735), severity of illness (p=2.03), and history of sleep disturbance (p=0.336) of the patients were comparable in all three groups (Table 2). Clinical assessments such as HARS, BAI, BDI, ESS, CGI–severity (Table 3) and parameters of WHOQOL-BREF (Table 4) at baseline were comparable between the groups.
Values are expressed as mean±standard deviation.
Values are expressed as mean±standard deviation.
H/O, history of.
Values are expressed as mean±standard deviation.
HARS, Hamilton Anxiety Rating Scale; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; ESS, Epworth Sleepiness Scale; CGI, Clinical Global Impression.
Values are expressed in mean±standard deviation.
WHOQOL-BREF, World Health Organization (WHO) Quality of Life BREF; GP, Group.
Primary outcome
Significant improvement on both the 15th and 30th day of interventions was observed (Figs. 1 and 2) in HARS (F(2,124)=698.82, p<0.001), BAI (F(2,124)=361.92, p<0.001), and CGI-I (F(1,62)=96.623, p<0.001). No significant differences were observed in any of these parameters between groups on both 15th and 30th day of treatment. Effect size of Groups II and I showed moderate to large effect compared to Group III (Table 5). However, the response and remission were comparable between the groups (Table 6).
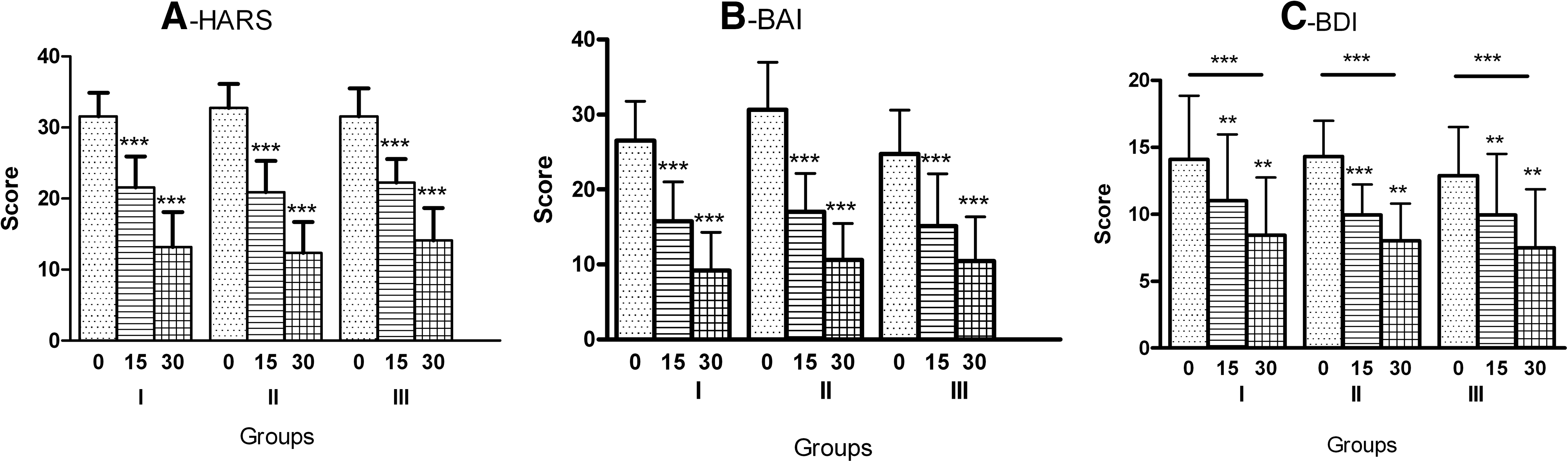
Changes in clinical assessment scales in Group I (n=22), Group II (n=22), and Group III (n=21) as assessed on 0 (baseline), 15th and 30th day of intervention:
Values are expressed in mean±standard deviation.
p<0.01, *** p<0.001.
HARS, Hamilton Anxiety Rating Scale; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; ESS, Epworth Sleepiness Scale; CGI, Clinical Global Impression; BL, baseline.
Values are expressed as number of patients and their percentage.
HARS, Hamilton Anxiety Rating Scale; BAI, Beck Anxiety Inventory; CGI-I, CGI, Clinical Global Impression-Improvement.
Secondary outcomes
All interventions produced significant linear improvement in BDI (F(2,124)=117.880, p<0.001) (Fig. 2). Raw values of WHOQOL BREF were used for the analysis. WHOQOL BREF total score showed significant improvement (F(2,124)=61.078, p<0.001) across time. However, post-hoc test revealed a significant improvement at the end of the treatment (p=0.008) in Group I. Group II showed significant improvement in the first 15 days and at the end of treatment (p<0.001). Consistent significant improvement was seen only in Group III (p<0.001). Significant improvement in all the domains was observed only in group III. However, no change was observed in any of the domains in group I. Group II showed significant improvement in domain 2 and 4 (Table 7). ESS showed significant effect of time (F(2,124)=16.290, p<0.001) when compared with groups as between-subject factor. However, post-hoc test revealed that only group II showed the decrease in the scores with the intervention. CGI-severity showed significant improvement with time (F(2,124)=135.760, p<0.001), and a similar observation was made in the CGI-Efficacy index (F(1,62)=122.727, p<0.001). All these parameters (BDI, ESS, WHOQOL BREF total score, CGI-severity and Efficacy index) showed no significant difference when compared between the groups on both the 15th and 30th day. Most of the parameters showed small-to-large effects in Groups I and II compared to Group III (Table 5) (Figs. 2 and 3).
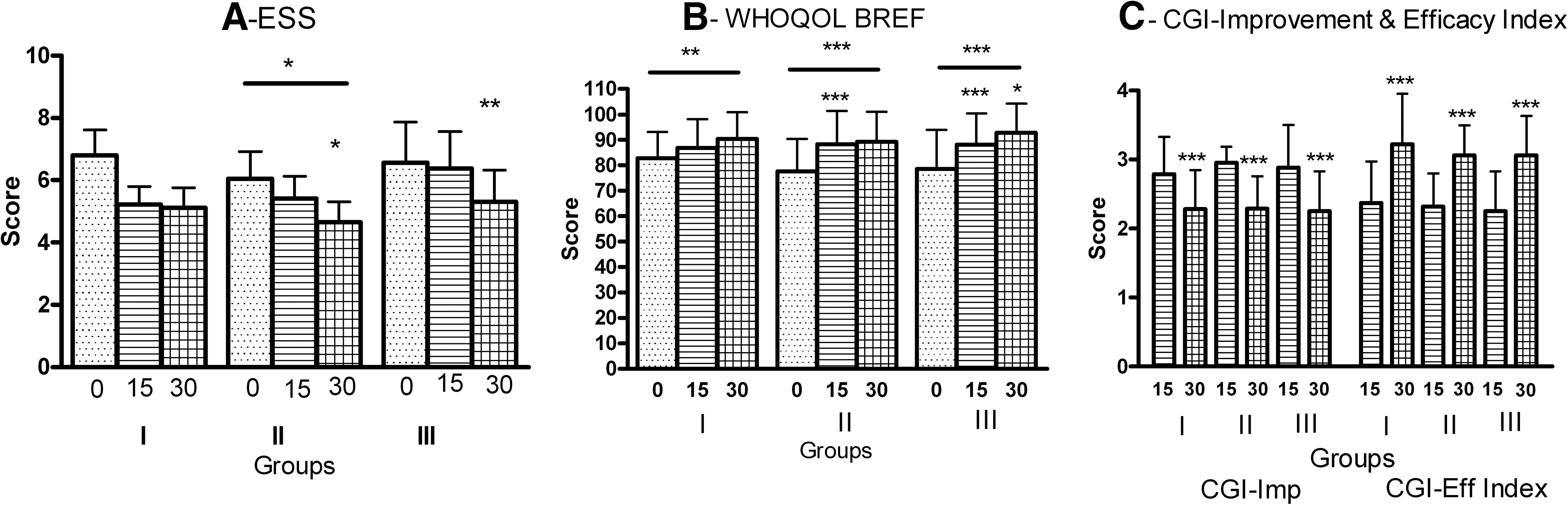
Changes in clinical assessment scales in Group I (n=22), Group II (n=22) and Group III (n=21) as assessed on 0 (baseline), 15th and 30th day of intervention:
Values are expressed as mean±standard deviation.
p<0.05, ** p<0.01, *** p<0.001.
WHOQOL-BREF, World Health Organization (WHO) Quality of Life BREF; BL, baseline; Gp, group.
Discussion
The present study demonstrates the clinical effectiveness of Manasamitra Vataka in the treatment of GAD with comorbid generalized social phobia. Thirty (30) days of treatment with Manasamitra Vataka reduced the anxiety, severity of the disease, increased quality of life, and improved clinical profile significantly. Shirodhara as an add-on therapy to Manasamitra Vataka decreased the daytime sleepiness and improved the quality of life in the patients.
Most of the patients (98.5%) were diagnosed with a severe grade of anxiety (HARS score >24) with duration of more than 7 years. The majority of the patients (83.5%) were diagnosed for the first time and had not received treatment for anxiety earlier. Comorbidity in anxiety and mood disorders is associated with increased severity and persistence. 33 Generalized social phobia is associated with a broad array of fears in interaction and performance (DSM IV) and is more severe and disabling than other social phobias. 34 GAD also has an adverse effect on the quality of life. 6 Social phobia strongly affects the quality of life with reduced social functioning, education, and career and also has a negative impact on work performance and social relationships. 35 In this study also, the clinical improvement was associated with improvement in quality of life. Insomnia is one of the most prevalent symptoms in GAD patients. 36 In the present study, 56% of patients reported a history of disturbed sleep. However, the daytime sleepiness assessed through Epworth Sleepiness Scale was in normative limits. 37 This may be attributed to irregularity in sleep disturbance in these patients.
Manasamitra Vataka was effective in reducing anxiety by reducing HARS scores and BAI scores. It was also effective in decreasing the mood disturbance as noted by changes in BDI. However, though the quality of life did not change on any domains, the gross score showed improvement with the treatment. Clinical global improvement and efficacy index also improved significantly. Coupling Shirodhara treatment with Manasamitra Vataka showed added advantages over Manasamitra Vataka alone. With the combined therapy, daytime sleepiness reduced significantly in the patients. The quality of life also improved across physical and environmental domains.
Manasamitra Vataka is a compound formulation (Table 8) with drugs having reported effects on the central nervous system. Ingredients such as aswagandha (Withania somnifera) are known to enhance cognition 38 ; vacha (Acorus calamus) when combined with Polygala root helps to maintain mental and intellectual health of the elderly 39 ; draksha (Vitis vinifera) is adaptogenic and nootropic 40 ; bala (Sida cordifolia Linn) is a known antioxidant 41 ; yashtimadhu (Glycyrrhiza glabra) has anxlolytic 42 and antioxidant 43 effects; and so on. In the Ayurveda literature, these drugs are described as medhya (neuroprotective, cognitive enhancer) and rasayana (health and cognitive promoting). 44 Brahmi (Bacopa monniera) enhanced cognition in healthy individuals when administered orally. 45 However, the effect of external use of Brahmi oil (B. monniera; Table 9) has not been reported. Shirodhara in healthy individuals has shown an anxiolytic effect as assessed by State–Trait Anxiety Inventory. 20,46 –48 Here, a similar anxiolytic effect by Shirodhara with Brahmi taila is reported when used along with Manasamitra Vataka in patients with GAD and generalized social phobia.
Whole plant includes stem, root, leaf, flower, and fruit of the plant.
Sl, no., serial number.
Benzodiazepines are the most commonly used drugs to treat anxiety disorders, and many studies have proved their efficacy in the management of GAD. 49 –53 The other preferred drugs in the management of GAD are SSRIs, SNRIs, and so on. 54,55 Benzodiazepines are also effective in the management of social phobia. 56 Clonazepam is a high-potency benzodiazepine effective in anxiety disorders and is the second most commonly used drug in GAD. 1 To the best of our knowledge, there are no studies reporting the use of clonazepam in GAD. However, clonazepam has been more widely studied in social phobia, and has been shown to be very effective. 57 –60 Clonazepam effectively reduced anxiety and mood disturbance, improved quality of life and also clinical outcome. The improvement was associated with increase in physical and psychologic health, and improved environmental and social relationships. It was also well tolerated with minimal adverse effects.
In the current study, the percentage of patients who responded to the treatment was comparatively more in Group II while remission was greater in Group I, though not statistically significant. The response and remission to HARS and CGI-Improvement criteria were comparable in all the groups.
Ayurveda treatment adopts an individualized, philosophical, and patient-centered approach in the diagnosis and treatment of psychiatric diseases. The treatment is a multimodal approach, comprising of spiritual, psychologic, dietary, and pharmacologic agents. Whole system research (WSR) 61 is a better and more suited approach for such systems of medicine. WSR has strong external validity compared to the strong internal validity of randomized controlled trials (RCTs). Model validity in WSR is the key component, which is complex and requires additional research studies. However, in the present study, specific treatments of Ayurveda such as Manasamitra Vataka and Shirodhara were evaluated and their assessment in the psychiatric population was carried out for the first time. Hence, the RCT format was followed, which is a conventional “gold standard” approach for evaluating the efficacy and can establish the causal relationship in biomedicine. The information obtained through this type of study might be of use in designing the WSR for Ayurveda treatments in anxiety disorders.
The strength of the present study is that alternative systems of medicine such as Ayurveda have the potential for providing effective, economical, and safer remedies for the ailing population. This study effectively establishes the efficacy of Manasamitra Vataka in GAD with comorbid generalized social phobia. The randomized control study provides clarity in the outcome of treatment across groups. The clinical scales and outcome measures demonstrated the global effect of the treatment on severity, associated sleep disturbance, daytime sleepiness, quality of life, improvement, and efficacy.
This study has several limitations, the foremost being that it was an open-labeled study. As both Manasamitra Vataka and Shirodhara are being studied scientifically in a psychiatric population for the first time, stringent criteria such as blinding could not be adopted. Clonazepam was administered in a fixed and smaller dose, but its tolerance and outcome profile were good. A longer period of intervention might have revealed a better treatment outcome. Lack of specific assessment for GAD and social phobia gave an indistinct view of the extent of change in these conditions with the interventions. Additional studies are required to detail the profile of the medications. Further assessment with other biologic parameters can give added information.
Conclusions
This study highlights the potential of Manasamitra Vataka and Shirodhara. Manasamitra Vataka significantly reduced the anxiety, severity of the disease, stabilized the mood, increased the quality of life, and improved the clinical profile of patients with GAD and comorbid generalized social phobia. Shirodhara therapy as an add-on to Manasamitra Vataka treatment helped in decreasing the daytime sleepiness and improving the quality of life in patients. Hence, the current medications are proposed as an effective treatment strategy in GAD with generalized social phobia.
Footnotes
Acknowledgments
We sincerely thank The Central Council For Research in Ayurveda & Siddha (CCRAS), Department of AYUSH, Ministry of Health & Family Welfare, Government of India, New Delhi, India for funding the project (Project No.13-18/ 2002/ Tech./ Vol. III). We acknowledge with thanks the excellent support provided by Dr. DeviDas, Assistant Director (Retired), Advanced Centre for Ayurveda in Mental Health and Neuro-Sciences, NIMHANS, Bangalore, India, during the initial stages of the study.
Disclosure Statement
No conflicts of interest exist.