
Abstract
Objectives:
What are the outcomes of acupuncture for back pain? According to well-regarded trials, acupuncture is little better for back pain than biomedicine, and active acupuncture is no better than sham acupuncture. These trials occurred in the West. Patients are inside the clinic a miniscule amount of time in relation to the time they are outside the clinic and enmeshed in the wider sociocultural context. Nevertheless, trials have largely overlooked potential effects of sociocultural context. The main objective of this article is to draw attention to designated features of sociocultural context that, as compared with outcomes obtained in the West, may enhance outcomes of acupuncture for back pain in China. Additional objectives of the article are to reconceptualize “sociocultural context” so that it is measurable, and to measure pre-existing acquaintance with acupuncture and other forms of Traditional Chinese Medicine (TCM) within the sociocultural context of China.
Design/Setting/Subjects:
Back pain patients (N=86) were recruited from the Acupuncture Clinic and Pain Clinic of West China Hospital (Chengdu, Sichuan Province). Patients completed questionnaires on their use of TCM before they came to the Acupuncture Clinic and their families' use of TCM.
Results:
Most patients had used TCM, and those who did so likely used it repeatedly, which indicated substantial acquaintance with TCM beliefs in the cultural context. Patients whose families used TCM were also likely to use it themselves, which indicated that TCM use was anchored in the social context of the family.
Conclusions:
Although multiple studies substantiate biologic mechanisms of acupuncture, there is not necessarily a fixed relationship between those mechanisms and people's experience of them. Rather, sociocultural context may interact with biologic mechanisms and mediate this experience. The theory proposed here explains why outcomes of acupuncture for back pain will potentially be more pronounced in the sociocultural context of China than in the West.
Introduction
Back pain is occurring along with the rapid rise of biomedicine in China. According to prominent reports, upwards of 80% to 90% of all medical care in China consists of biomedicine, but this presumably pertains to medical care in formal settings. 6,7 Injections, a symbol of biomedicine, 8 are commonly used in China. Almost the entire population of China has received injections for immunization against common preventable diseases. 9 Antibiotics, either injected or administered orally, transformed biomedicine and constitute another symbol of it, 10 and the high prevalence of resistance to various antibiotics indicates that they are overused in some areas of China. 11,12 In short, biomedicine has become pervasive in China.
The rise of biomedicine in China, however, is unlikely to result in a corresponding fall in its back pain problem. From the perspective of biomedicine, back pain remains an ambiguous and troubling clinical entity. 13 According to highly regarded back pain researchers in Europe and the United States, a definite cause of back pain may be identified in less than 15% of all cases. 14,15 Few biomedical treatments of back pain have proven to be more effective than any other biomedical treatment or placebo. 16 –19 Clearly, back pain is among the symptoms on the margins of biomedical competence. 20
In their search for more effective treatment, researchers have looked beyond biomedicine. Among the treatments they have tested is acupuncture. High-quality trials, however, have yielded a perplexing result. Outcomes of acupuncture for back pain appear to be better than outcomes for wait-list controls, 21 biomedical treatment based on guidelines, 22 and biomedical treatment as usual. 23 Nevertheless, active acupuncture in these trials is not significantly better than “sham” acupuncture. This conclusion comes with caveats. The use of sham acupuncture in trials has elicited a number of criticisms in the literature, 24 –26 and, of course, its use also necessarily implies that the trials were not double-blinded (acupuncturists administering the sham were cognizant of doing so). 27 In comparing outcomes of acupuncture (active or sham) with outcomes of biomedical treatment, effects sizes are small. 28, 29 Finally, and central to this article, the high-quality trials of acupuncture for back pain discussed here have taken place in the West (the United States and Germany). Similarly, systematic reviews of the literature have revealed, in general, a lack of high-quality trials conducted in China, 30 and, more specifically, no high-quality trials in China that pertain to acupuncture for back pain. 29, 31
Although there is a lack of consensus in the literature on the labeling of different types of medicines, 32 the particular type of medicine practiced at the research site will be referred to as “Traditional Chinese Medicine” (TCM). Practitioners and patients at the research site used this term, and acupuncturists whose patients were recruited for the study received their training from Chengdu University of Traditional Chinese Medicine. TCM is indigenous to China, which raises the question of what outcomes of acupuncture for back pain would be if high-quality trials had been performed in China instead of the West. The contemplation of those outcomes, of course, presupposes that, despite the rise of biomedicine, a substantial presence of TCM has remained in the sociocultural context of China. In other words, even if biomedicine is nearly a constant, there may be “medical pluralism” in China, with two (or more) separate medical currents within the mainstream of its health care. 33,34 The central government of China subsidizes TCM in various ways (training, research, patient care). 6,35 In contrast, the question explored here is the depth of TCM within the sociocultural context of a population of patients in China seeking care for back pain and the families of those patients.
To lay out the organization of this article, its next two sections are empirical. The intent of each of these sections is to convey a certain point. The Materials and Methods section concerns the social and cultural context in which acupuncture occurs, hereafter referred to as “sociocultural context.” This is an elusive concept, however, and to propose its theoretical potential (which is the point of the Discussion section) begs the question of how to measure it in the first place. As Kelvin famously stated, “If you cannot measure, your knowledge is meager and unsatisfactory.” 36 Accordingly, the main purpose in Materials and Methods is to break down the concept of sociocultural context and reconceptualize it so that it is measurable. The Results section presents findings on the depth of TCM within the sociocultural context of a population in China.
In a sense, the empirical sections are a prelude to the final Discussion section of the article. The purpose of the Discussion is to direct attention outward to the larger sociocultural context and the often overlooked but potentially influential effect it may exert on the outcomes of acupuncture for back pain. There is no inherent contradiction between such an outward viewpoint and clinical trials. Nevertheless, in practice, clinical trials tend to be inwardly focused and concentrate on what is most readily observable in the clinic, especially a discrete disease, its treatment, and miscellaneous moderators of treatment (notably, demographic variables such as patient's age, race, and sex). The inward viewpoint, furthermore, logically leads to the search for underlying “biologic mechanisms” of disease and its treatment. Clinical trials and the attendant reduction of disease and treatment to biologic mechanisms largely delineate the realm of biomedicine. Charles Rosenberg, a preeminent historian of medicine whose observations extend to present times, has remarked upon the widespread “assumption of hierarchy,” with biomedicine's “right to ultimately define the true and efficacious in the profession's own terms.” 37
Nevertheless, the concentration on the inward viewpoint with only peripheral attention to the outward viewpoint at least theoretically leads to imbalanced investigations of acupuncture for back pain, because patients are inside the clinic only a minuscule amount of time in relation to the time they are outside the clinic and enmeshed in the larger sociocultural context. In short, this article aims to broaden the focus of investigations, to retain the inward viewpoint but, at the same time, offer a complementary viewpoint and direct attention outward to the larger sociocultural context in which the clinical encounter occurs. Before doing so, however, it is first necessary to demonstrate that features of sociocultural context are measurable and that a substantial presence of TCM has remained within the sociocultural context of China.
Materials and Methods
Research site
The research occurred at West China Hospital, which is located in Chengdu, a city with a population of nine million in the southwestern province of Sichuan. West China Hospital, affiliated with Sichuan University, is one of the largest hospitals in China, with 4,300 beds and 2.55 million outpatient visits per year. 38 Aside from patient care, West China Hospital is a well-recognized research institute. Its Institutional Review Board approved of this study.
Investigators recruited patients for the study from two outpatient clinics of West China Hospital, i.e., the western-style Pain Clinic (in the Department of Anesthesiology) and the Acupuncture Clinic (in the Department of Rehabilitation Medicine). Customarily, patients in China do not have a primary care physician. Those who came to West China Hospital for treatment of back pain arrived in the morning, most of them with their families. In the vast hospital lobby, they had only a few moments to present their symptoms to a triage nurse, while other patients and their families waited their turn. There was little time to present a detailed history and family background. Some patients expressed a preference for a clinic, but others did not. The nurse then directed them to a clinic.
Patient selection and administration of questionnaires
Once patients arrived at the Pain Clinic or Acupuncture Clinic, investigators selected those who presented with nonspecific back pain and otherwise fulfilled the criteria in Table 1. “Post-graduates” (residents) in anesthesiology and acupuncture administered questionnaires to patients, who filled them out while waiting for their first visit of an episode of care (defined as no other care for back pain at West China Hospital in the previous three months). 39
The adult literacy rate for China is >94% and is higher in urban areas (such as Chengdu, where West China Hospital is located). 67
Construction of variables
Using data from questionnaires, investigators constructed variables on three distinct “levels of analysis”: 40 cultural, social, and individual. These levels of analysis, depicted in Figure 1, are described below.
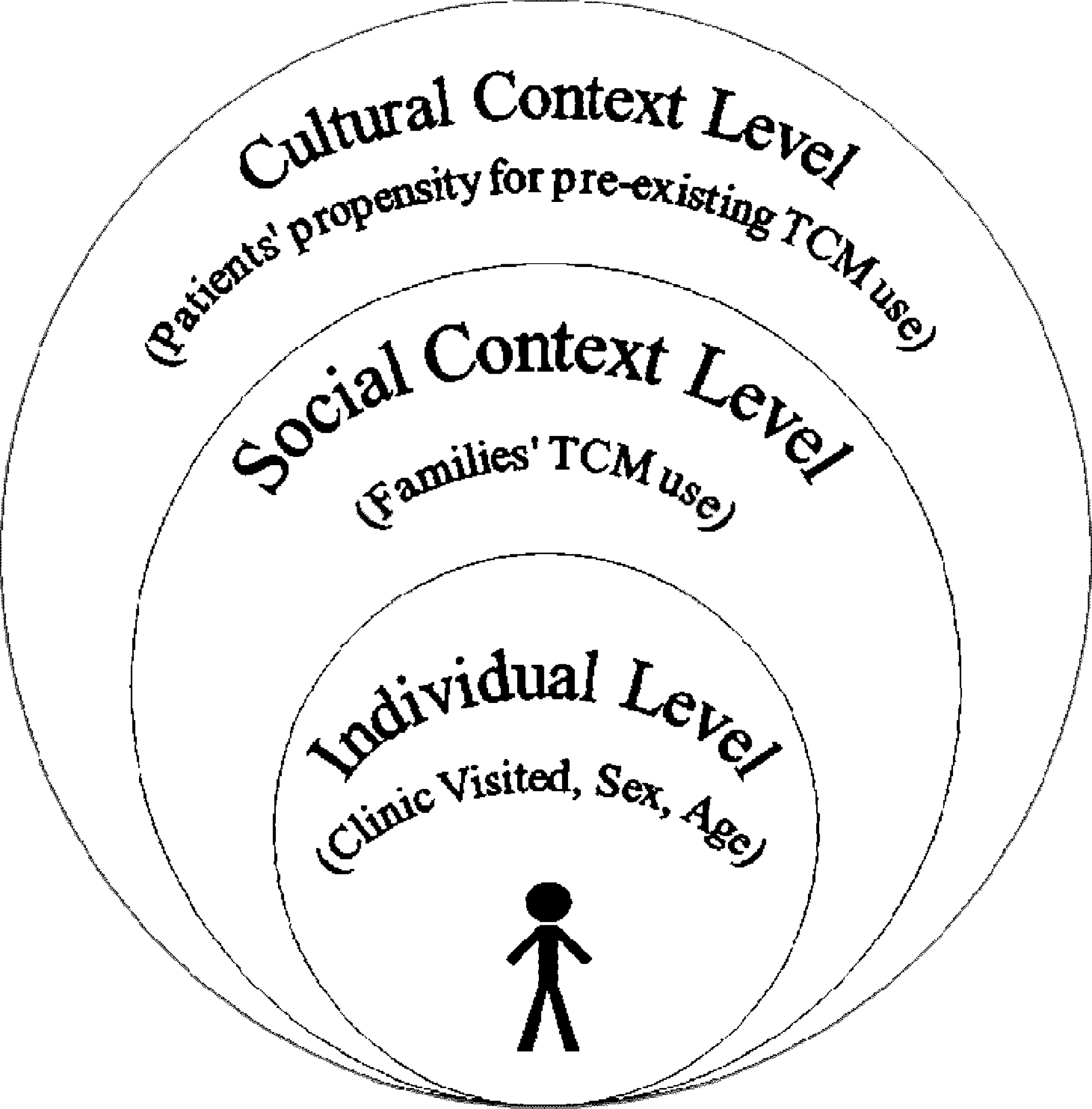
Levels of analysis.
Cultural level
“Sociocultural context” is a vague and abstract term. Its reconceptualization is required to proceed from the more abstract to the less abstract so that, finally, measures of it may be devised. Regarding culture first (the cultural part of “sociocultural context”), Kroeber et al. assembled 164 definitions of it two generations ago, 41 which did not deter their successors from renewed attempts to define it. Rather than the definitive definition, presented here are core features of culture commonly found in the anthropological literature. As depicted in Figure 1, a core feature of culture, then, is that it is passed down from one generation to another, and, as such, it is supra-individual, as distinct from a property of an individual. To move from a more abstract to a less abstract and more measurable feature, beliefs inhere within culture. 42 Although “beliefs” is a term that has elicited objections, 43 it often represents culture in patient-centered analyses of health care. A search for “beliefs” in the PubMed bibliographic database retrieves more than 9,000 citations to relevant articles published in the past five years. 44
Beliefs of patients in the study, of course, resided in their heads and were not directly observable. Questions in the questionnaire were necessary to draw out beliefs. Questions simply ascertained patients' history of TCM use, particularly whether they reported a pattern of its repeated use. In other words, having tried TCM, had patients tried it again? Repeated use represents underlying beliefs. If those who used TCM found afterward that they disbelieved in it, they would have been unlikely to use it again.
Patients' propensity for repeated TCM use was thus made up of two components: (1) their pre-existing use of TCM for conditions other than their current back pain, and (2) their pre-existing use of TCM for current back pain (prior to their episode of care at West China Hospital). “Pre-existing TCM use” was broadly construed. If patients used acupuncture in the past five years, or besides acupuncture, if they used any other type of TCM in the past one year, they were classified as TCM users. In order to trigger patients' recall and obtain as comprehensive responses as possible, 45 the questionnaire specified “other types of TCM,” i.e., prescribed and nonprescribed TCM soup, TCM preprocessed medicine or decoction, TCM application cream or ointment, and all other forms of TCM. Patient's use of TCM was a dichotomous (yes vs. no) variable.
Social level
The social level of analysis (the social part of “sociocultural context”) implies interaction between two or more individuals. Social interaction is supra-individual, and, as shown in Figure 1, it as well as culture compose the individual patient's context. In particular, this analysis considered fundamental social interaction that takes place within the “primary group” of the family. 46 Questions on the family's TCM use were structured the same as questions on the patient's TCM use. A family was classified as using TCM if one or more of its members used either acupuncture in the past five years or any other type of TCM in the past one year. When inquiring about family TCM use, the questionnaire again prompted patients' recall and specified each close family member (husband, wife, father, mother, brother, sister, and children). Family's TCM use was another dichotomous (yes vs. no) variable.
In responding to questions about their families' TCM use, patients served as proxies for their family members. The U.S. Census and other well-established surveys accept proxy responses from family members. 47, 48 For questions about use of health products and services (among which would be TCM products and services of TCM providers), studies have shown good agreement between proxy responses from family members and self-responses. 49 –51
Individual-level variables
As shown in Figure 1, individual-level variables were also entered into the analysis in order to determine whether they moderated variables within the patient's sociocultural context. Individual-level variables were the following: Type of Clinic Visited (Pain Clinic vs. Acupuncture Clinic), Sex (Male vs. Female), and Age (≤30, 31–40, 41–50, ≥51).
Cross-cultural adaptation of questionnaire
Questions used to collect data for this analysis were part of a larger survey on back pain treatment.
52
In accordance with recommendations on “the cross-cultural adaptation of self-report measures,”
53
the survey was put through three stages of translation, with translators involved in one stage not involved in the others. In other words, the survey first went through two independent forward translations (English to Chinese), then two independent backward translations (Chinese to English), and, finally, two more independent forward translations. At each stage, a committee whose members were not involved in the translations resolved discrepancies between translators. The English version and the cross-culturally adapted Chinese version of the questionnaire are accessible through the electronic version of this article (see the Appendix of Supplementary Materials, available at
Data analysis
In analyzing the data, investigators collapsed two overlapping variables—Use of Acupuncture and Use of Other Forms of TCM—into one variable, “TCM use.” They then performed two multiple logistic regression analyses:
As described earlier, with the exception of age, all variables were dichotomous, including the dependent variables in both analyses, the explanatory variables of interest, clinic visited, and sex. “Families' TCM Use,” the explanatory variable of interest in Analysis 2, was also an explanatory variable in Analysis 1, although not the one of interest. Additionally, all individual-level variables were entered into both analyses.
Results
A total of 86 patients, 45 from the Acupuncture Clinic and 41 from the Pain Clinic, completed questionnaires. Descriptive statistics are in Table 2. Patients from the Acupuncture Clinic for the most part did not differ significantly from those from the Pain Clinic (rows 1–3,5). However, the families of patients from the Acupuncture Clinic were significantly more likely to use TCM than the families of patients from the Pain Clinic (row 6). Additionally, the difference with which patients from each clinic used TCM for other conditions besides current back pain bordered on statistical significance, with patients from the Acupuncture Clinic marginally more likely to use it than those from the Pain Clinic (row 4). These findings (rows 4,6) suggest that when patients first came to West China Hospital and spoke with the triage nurse (described in Materials and Methods, Research Site), their personal preference for a clinic had an effect on the clinic where they were sent for treatment but was not determinative of where they were sent. Notably, most patients (58.5%) sent to the western-style Pain Clinic had used TCM for current back pain or another recent condition (row 5).
t-Tests and χ2 tests were used to test for significant differences between means and percentages, respectively.
Investigators first examined bivariate relationships in both logistic regression analyses (Analysis 1 and Analysis 2, both of which are described in Materials and Methods). For both analyses, the p values of bivariate relationships for all but two explanatory variables was >0.25, and thus only two explanatory variables entered into final, multivariate models. 54 In each multivariate model, however, one more explanatory variable was insignificant. Only a single explanatory variable, the one of interest, remained significant in each of the analyses.
Main results from Analysis 1 and Analysis 2 are shown in Figures 2 and 3, respectively. Recall that data for the study were collected as patients waited for their first visit at West China Hospital for current back pain, although most had otherwise tried treatments before they came to the hospital. Analysis 1 compared patients who had used TCM for other conditions besides current back pain with patients who had no evident use of TCM for these other conditions. Patients who had used TCM for other conditions were more than eight times more likely to have also used it for current back pain than patients with no evident use of TCM for other conditions (p<0.001). Analysis 2 found that patients whose families used TCM were about three-and-a-half times more likely also to use TCM themselves (for any reason) than patients whose families did not use TCM (p=0.014).
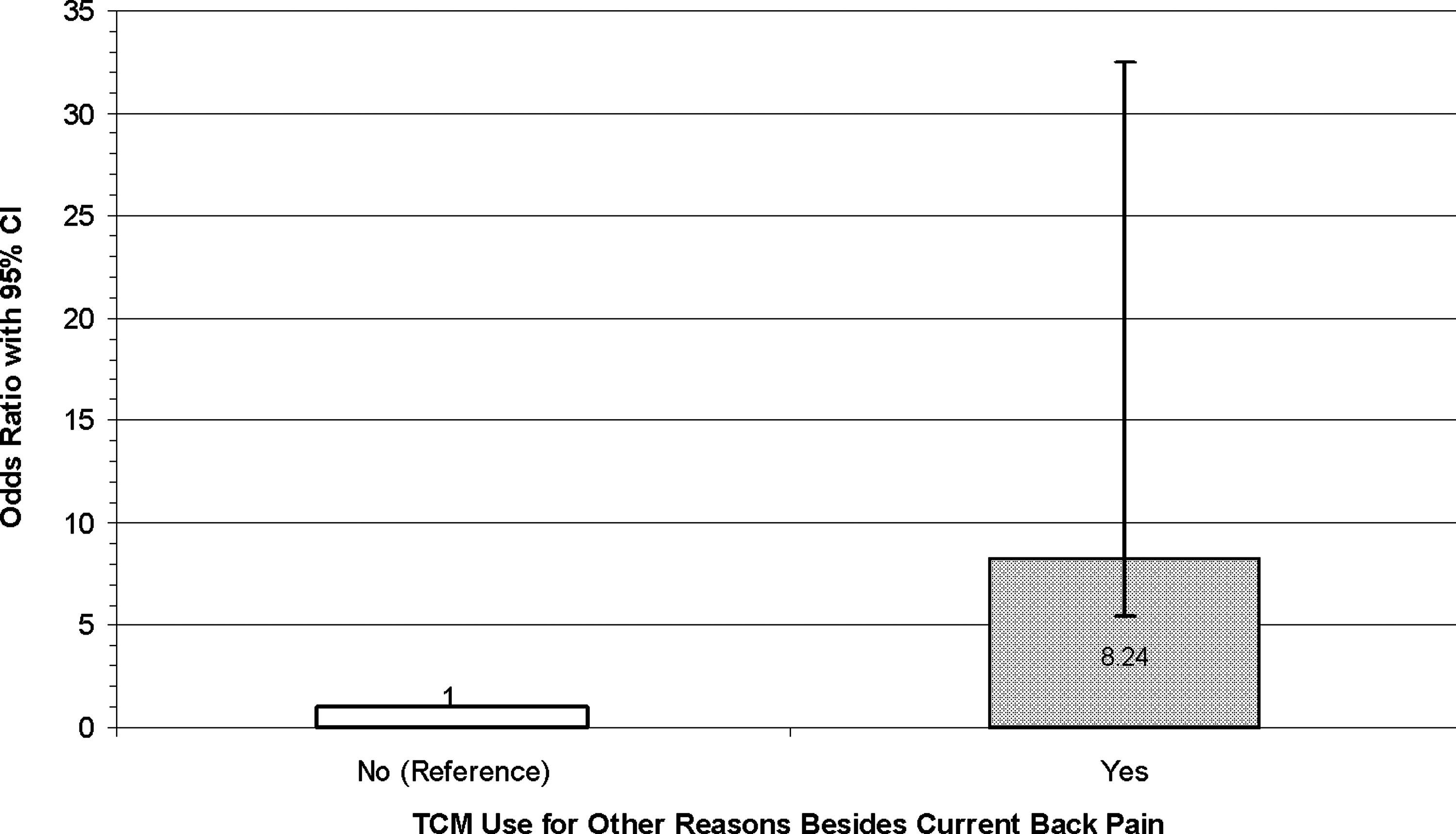
Logistic Regression Analysis 1, effect of Patients' TCM Use for Other Reasons Besides Current Back Pain (explanatory variable of interest) on their TCM Use for Current Back Pain (dependent variable).
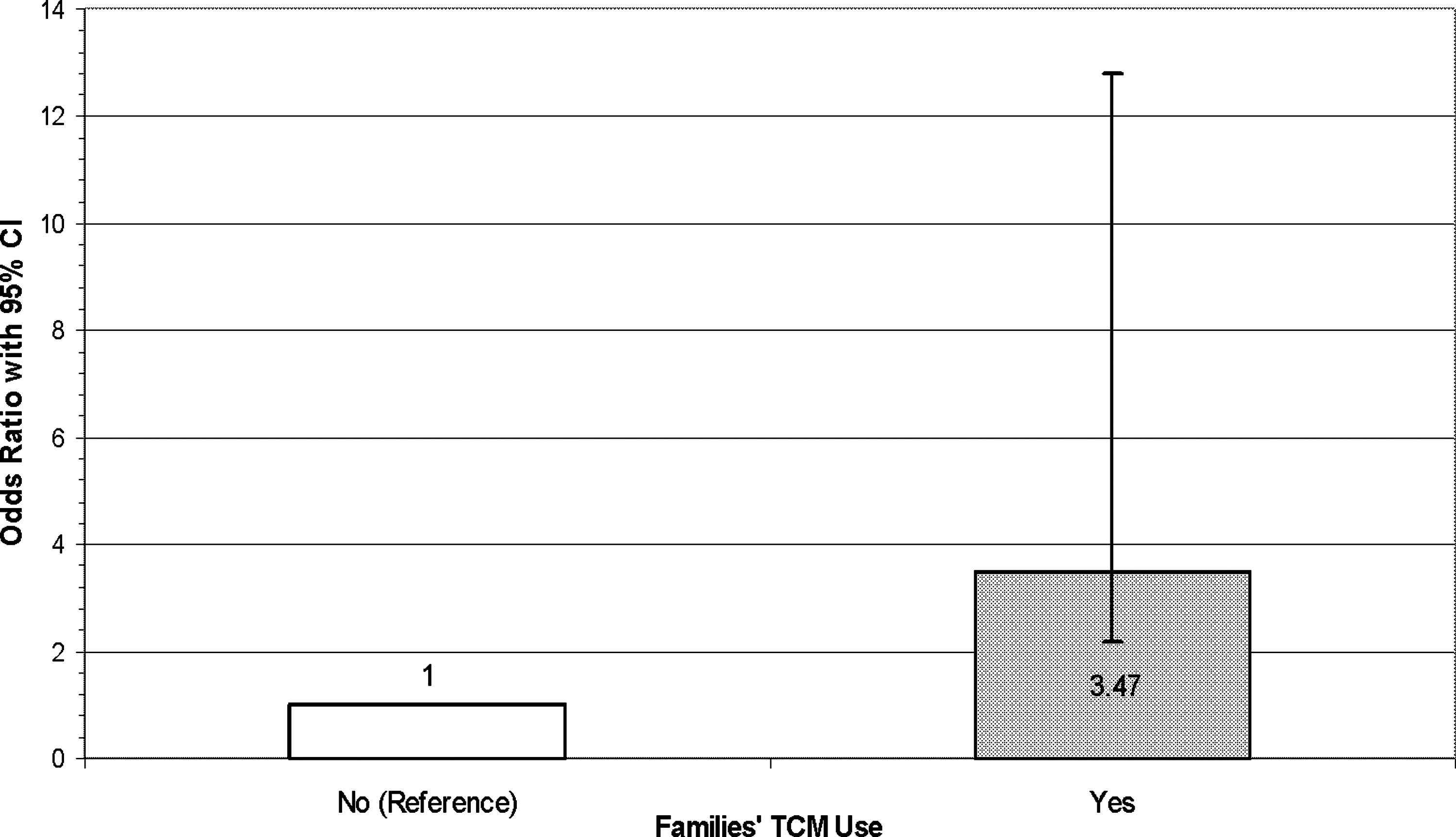
Logistic Regression Analysis 2, effect of Families' TCM Use (explanatory variable of interest) on Patients' TCM Use for Any Reason (dependent variable).
Detailed results of the bivariate analyses and the final multivariate analyses are accessible through the electronic version of this article (see Table 1 of Supplementary Material, which follows English and Chinese versions of the questionnaire, all available online at
Discussion
A substantial presence of TCM existed within the sociocultural context of the study population. Before their first visit for current back pain, two-thirds of all patients had used TCM for their current back pain or another recent condition (Table 2, row 5). Included in this population were patients who visited not only the Acupuncture Clinic but also the western-style Pain Clinic.
Prior to their arrival at West China Hospital for current back pain, patients who had used TCM for conditions other than current back pain were more than eight times more likely to have tried it again for current back pain than those with no evident use of TCM for other conditions (Fig. 2). TCM use was seldom an anomalous attempt to relieve current back pain but instead most likely led to TCM use again. Repeated TCM use of this nature represented beliefs in the cultural context. In the final, multivariate model, the finding that use of TCM most likely led to repeated use was not significantly affected by the clinic to which patients were triaged (Pain Clinic or Acupuncture Clinic), age, or sex.
Patients whose families used TCM were about three-and-a-half times more likely to use TCM themselves (for any condition) than patients whose families did not use TCM (Fig. 3). Again, in the final, multivariate model, this finding was not affected by the clinic to which patients were triaged, age, or sex. Beliefs in TCM were thus not free floating within the culture of China but rather were anchored within the social context of the family.
These findings came from a population of patients (N=86) who visited two outpatient clinics of a hospital in China. This is thus a “pilot study.” More studies elsewhere in China as well as larger patient populations are necessary to determine whether findings from it are representative of TCM in the sociocultural context of China as a whole.
Treatment of the patient takes place within the confines of clinics. How may the larger sociocultural context impinge upon the consciousness of individual patients and affect the outcomes of their treatment? The case made in the discussion that follows is that beliefs within the cultural context as well as the social context of the family may both exert effects on outcomes of individual patients.
Why beliefs within cultural context matter
The propensity for repeated TCM use indicates that those who had experienced TCM treatment believed that it was beneficial, and they came back for more. The potential of beliefs to affect health outcomes is demonstrated in a study published in The Lancet. 55 It also pertained to people of Chinese origin, although it was conducted in the United States. Subjects in the study who were born during what according to Chinese astrological beliefs were “ill-fated” years and also had what was believed to be an ill-fated disease given their birth years did not live as long as matched (“white”) controls born in the same years and with the same disease. The reduction in longevity was especially marked among those born in China, whose commitment to traditional Chinese beliefs was the greatest; longevity in this subgroup was 6% to 7% less than in matched controls. If the potential to exert an influence on life and death inheres within such beliefs, they may have still more of a potential to influence the effects of pain treatment.
In particular, patients may bring certain beliefs to the clinical encounter that promote or, alternatively, inhibit the effects of acupuncture. In other words, beliefs, although in themselves not determinative of outcomes, may influence outcomes. To explain how they may do so, the distinction between “knowledge about” and “acquaintance with” is useful. As demonstrated in Table 3, this is a distinction built into the structure of many languages, and commentary on it has a venerable lineage. 56 To apply the distinction specifically to acupuncture treatment of back pain, most patients in China, already well acquainted with beliefs that underlie TCM before they enter the clinical encounter, would readily comprehend diagnoses the acupuncturist provides to them. With successive treatments, patients in the West may acquire some “knowledge about” TCM diagnoses, which is to be distinguished from direct “acquaintance with” TCM. “Acquaintance with” pertains to a deep-set, insider perspective, and as compared with the “knowledge about” perspective of an outsider, it potentially exerts more of an effect on outcomes. For example, patients in the West may recoil from the sensation brought on by acupuncture needling, especially when first experiencing it. 57 In contrast, patients in China would be more likely to apprehend the sensation as “de qi” and immediately associate it with therapeutic effects.
From RK Merton. 56 Used with permission of University of Chicago Press.
Why the social context of the family matters
The questionnaire administered to patients restricted inquiries about family TCM use to close family members, including husband, wife, parents, siblings, and children. Epidemiological studies have repeatedly found “concordance” in mental and physical health mainly between spouses but also between siblings and among parents and their children. 58,59 The possibility of concordance between family members may be extended to treatment effectiveness as well. To use Cooley's term, close family members serve as a “looking-glass self,” 46 or, to use a more contemporary term, a “mirror” of the self. In explaining the dynamic within the family, Cooley alludes to Lewis Carroll's Alice through the Looking Glass:
“Each to each a looking-glass
Reflects the other that doth pass.”
In other words, people come to define themselves and their circumstances in life largely through the eyes of close family members. Of all patients in the study population, more than half (56%) had one or more close family members who had recently used TCM (Table 2, row 6). Regarding acupuncture treatment in China, patients return home to a family context commonly supportive of its therapeutic effects. On the other hand, family members of patients in the West, in large part unacquainted with TCM, may be more likely to be dismissive of the acupuncturist's diagnoses for back pain or question the experience of de qi. Family context in this way would serve to sustain or offset the effects of acupuncture.
Interaction between sociocultural context and underlying biologic mechanisms
The two viewpoints of acupuncture described in the Introduction are conducive to parallel lines of investigation that do not intersect. Those who investigate biologic mechanisms of acupuncture (representing the inward viewpoint) do so in laboratories and brain-imaging centers set apart from sociocultural context. On the other hand, the emphasis on sociocultural context (outward viewpoint) gives rise to the question of what the role of acupuncture itself may be. Is acupuncture essentially an inert procedure, and is sociocultural context a placebo that brings about its observed effects?
The position presented here is that the interaction of viewpoints is necessary to understand the outcomes of acupuncture for back pain. Multiple studies substantiate the biologic mechanisms of acupuncture, and they are inducible irrespective of sociocultural context. 60 –63 Nevertheless, patients treated with acupuncture for back pain are people, as opposed to insensate recipients of biologic mechanisms. There is no necessary or simple relationship between biologic mechanisms of acupuncture and people's experience of them. As classic studies reviewed in Table 4 show, marijuana, epinephrine, and alcohol induce biologic effects, but variations in sociocultural contexts produce differences in people's experience of those effects. Just as sociocultural context serves to mediate the experience of these chemical substances, so too may sociocultural context interact with the biologic effects of acupuncture to mediate people's experiences of acupuncture.
Note: Marijuana, epinephrine, and alcohol induce biologic effects, but as the studies reviewed in the above table show, variations in sociocultural contexts produce differences in people's experience of those effects. Just as sociocultural context serves to mediate the experience of these chemical substances, so too may sociocultural context interact with the biologic effects of acupuncture to mediate people's experiences of acupuncture.
Conclusion: Three Testable Predictions in Search of Trials that Account for Sociocultural Context
The authors of this article have assembled elsewhere a set of measures with which to evaluate acupuncture for back pain in four outcome domains: pain, physical disability, emotional functioning, and global rating of improvement. 52 English as well as cross-culturally adapted and validated Chinese versions of the measures are within the set. As distinct from outcomes, this article concerns sociocultural context that surrounds the clinical encounter and supposedly pervades outcomes. The measurement of “sociocultural context,” however, requires forethought. The Materials and Methods section of this article suggests a way to reconceptualize and measure TCM in the sociocultural context of China and, in so doing, formulate explanatory variables that may be entered into an analysis of treatment outcomes (i.e., patient's cultural beliefs in TCM as evidenced by repeated TCM use prior to the first clinic visit, Yes vs. No; patient's social context supportive of TCM as evidenced by close family members' TCM use, Yes vs. No).
The already cited high-quality trials of back pain were conducted with little regard to sociocultural context. 21 –23 According to them, the outcomes of active acupuncture are little better than the outcomes of biomedicine, and, furthermore, the outcomes of sham acupuncture and active acupuncture are similar. Results obtained from these trials may be generalizable to the West, where they occurred, but not necessarily beyond the West (by extension, results of systematic reviews and meta-analyses based on trials conducted in the West pertain to the West but not necessarily beyond). What would be the outcomes had acupuncture for back pain been tested in sociocultural contexts other than the West?
This article concludes with three predictions about those outcomes. Notably, these are predictions amenable to testing in trials. The first and most general of them sums up the theme of the article: Variations in sociocultural contexts will systematically bring about differences in the outcomes of acupuncture for back pain. The other predictions, derivable from the first one, pertain to specified features of sociocultural context and the proposed effect of these features on outcomes.
As evidenced especially in Table 2, patients in China, more commonly than patients in trials conducted in the West, enter the clinical encounter already having an “acquaintance with” TCM, and, additionally, they return home from the clinical encounter and to a family social context more likely to be supportive of the effects of acupuncture treatment. In view of such a sociocultural context, the second of the three predictions follows: In relation to outcomes of acupuncture for back pain obtained in trials in the West, outcomes will be more pronounced in China and still more distinguishable from outcomes of biomedicine. In China, as in the West, outcomes of active acupuncture and sham acupuncture both may be better than outcomes of biomedicine. Patients in China, most of whom are already acquainted with TCM before they enter the clinical encounter, are more likely than patients in the West to be preconditioned to perceive the effects of active acupuncture. The implication of this may be stated as the final of the three predictions: In China, outcomes of active acupuncture will be still better than the outcomes of sham acupuncture.
Footnotes
Acknowledgments
We obtained support from China Medical Board, Grant No. 88–486, West China Center for Medical Education, Research and Development, Sichuan University. We wish to thank participants in the cross-cultural adaptation of the measures, including Zhiqin (Julia) Xu, MS; Lin Sun, MD; He Huang, MD; Ying Brach, MS; Liang Li, MD, MS; Jimmy Lu, MBA; and Wen H. Kuo, PhD. Professor Deng Hong of the Office of International Affairs, Sichuan University, provided critical help throughout each step of the research. Faculty members and graduate students from The West China School of Public Health, Sichuan University, contributed greatly to the research and informed it in many ways, especially Xiaosong Li, MD, MPH, PhD, and Ping Shuai, PhD.
Disclosure Statement
All authors declare no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.