
Abstract
Objectives:
Pain induced by surgery is a dynamic symptom, which may be quite variable even in the same surgical procedures. The purpose of this study was to investigate the analgesic effect of far infrared rays on the patients during the postoperative period of total knee arthroplasty (TKA). The selection and application of analgesic methods after the orthopedic surgery are therefore valuable for advanced studies.
Design:
The quasi-experimental design with a total five consecutive days of far infrared ray (FIR) thermal therapy was employed in this study.
Subjects:
The study involved 41 participants assigned by register code entry on computer to either the intervention or the control group.
Intervention:
The FIR pads were applied on the acupoints of ST37 (Shang Chu Hsu), ST38 (Tiao Kou), ST39 (Hsia Chu Hsu), and ST40 (Feng Lung) of the patients involved in the experimental group from the third day to the fifth day after the TKA.
Outcome measures:
The analgesic effect was evaluated via the pain intensity of the numeric rating scale (NRS) level and serum concentration of interleukin-6 (IL-6) and endothelin-1 (ET-1).
Results:
The FIR showed that the significant effects are on relieving pain and lowering the levels of IL-6 and ET-1. The results cannot only be the reference for the postoperative pain relief of TKA, but it can also be the database of another clinical application.
Conclusions:
This study demonstrated that the FIR can lower the NRS of pain and thus reduce the discomfort experienced by the patient. Findings indicated that effective application of FIR decreased the serum level of IL-6 and ET-1, which represent the subjective indicator of pain.
Introduction
Surgery will induce the damaged tissue to secrete the precursor cytokines such as interleukin-1 (IL-1), interleukin-6 (IL-6), tumor necrosis factor-α, and endothelin-1 (ET-1). Additionally, prostaglandins, such as prostaglandin E2 and prostaglandin I2, and neurotransmitters, such as nerve growth factor, serotonin, and kinins (bradykinin), will be secreted. The damaged tissue will demonstrate an erythematous and swollen appearance with warm and painful sensation, with some hormones being released. 5,6
Far infrared ray (FIR) is one kind of electromagnetic wave, which has the properties of light and wave. FIR is an invisible portion of the electromagnetic spectrum with the wavelength ranging from 4.0 to 14.0 μm. It has three biologic effects: radiation, resonance, and thermal effects. The energy of the electromagnetic wave is absorbed by the skin and then transferred to heat by the irradiation, resonance, and molecular collision. It causes local vessel dilatation, increases capillary circulation, and improves tissue repairing, which increases the patient's pain threshold. Therefore, these effects relieve surgical pain, improve wound healing, 7 and activate physiologic function. 8
According to the theory of Chinese medicine, stimulating the specific acupoints brings about a beneficial physiologic effect. 9 Previous studies demonstrated that meridians have the physiologic properties of higher conductivity, lower impedance, latent transmission, and high resonance. 10 The FIR pad was applied to the acupoints of the limb following TKA surgery, and the effect of pain relief was evaluated via pain scores and biologic indicators (i.e., IL-6 and ET-1). Then, the recovery of ambulation and improvement of quality of life were also evaluated. 11 It is hypothesized that the FIR therapy pad will show a greater decrease in pain and serum IL-6 and ET-1 levels, compared to the experimental group and control group of patients with TKA. Also, the FIR therapy pad will cause a greater decrease in pain and serum IL-6 and ET-1 levels, compared to the pretest and post-test of the experimental group of TKA patients.
Materials and Methods
Study design
A total of 41 cases were recruited. Subjects (n=41) with a diagnosis of osteoarthritis treated by TKA were required to follow all the criteria for inclusion. According to different hospital orthopedic wards, these patients were randomly assigned by register code entry on a computer to either the intervention group or the control group. Forty-one (41) patients received TKA surgery at a medical center in northern Taiwan. They were divided into an experimental group of 20 subjects with intervention of FIR and control group of 21 subjects with no intervention. The inclusion criteria were as follows: (1) adults with clear consciousness, (2) patients with a diagnosis of osteoarthritis treated by TKA, and (3) more than 4 points on the numeric rating scale (NRS). Patients with infection, abrasion, or ulceration on the skin around the selected acupoints were excluded. There were no prescribed nonsteroidal anti-inflammatory drugs allowed 4 hours before the application of the FIR pad. All human protocols, intervention methods, and laboratory analyses were approved by the Institutional Review Board of the Tri-Service General Hospital and the Ethics Committee, Taipei, Taiwan, Republic of China. All subjects provided written informed consent prior to enrollment in the study.
Thermal therapy treatment
Subjects in the experimental group were provided with the thermal therapy pad with FIR for 15 minutes per day with a total of 5 times consecutively from the third day following the TKA surgery. The FIR pads were attached to the selected acupoints that were ST37 (Shang Chu Hsu), ST38 (Tiao Kou), ST39 (Hsia Chu Hsu), and ST40 (Feng Lung) of the involved lower extremities. On the third day and the eighth day following the TKA surgery, NRS, and serum sampling for biologic indicators such as IL-6 and ET-1 were analyzed.
Questionnaire and biologic index assessments
Demographic data and NRS
Subjects provided details and information on age, gender, the experience of surgical pain, the experience of most severe pain, the interventions used for pain relief, and endurance level of pain. The NRS was used to measure pain intensity. It could also measure the subject's emotional status. The NRS used a 10-cm-long horizontal line. One (1) calibration represents 1 point, with 0 representing no pain and 10 representing pain as bad as it could be, depicted on the horizontal line.
Assessment of IL-6 and ET-1 measurement
Blood samples of IL-6 were obtained before and after the FIR intervention. The serum level of IL-6 was determined by the specific enzyme-linked immunosorbent assay (ELISA) kit as described in the manufacturer's manual (ELISA Kit, Tecan Chemical Company). The spectrum reaction was measured at 450 nm in a micro-ELISA reader. Blood samples of ET-1 were again obtained before and after the FIR intervention. The serum level of ET-1 was determined by the same ELISA kit as described in assessment of IL-6. The spectrum reaction was measured at 405 nm in a micro-ELISA reader.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 12.0. Chi-square, independent samples t test, and paired-samples t test were used for data analysis. An α of 0.05 was used for all statistical tests.
Results
Demographic data
There was no statistically significant difference in the demographic data except for the gender between the experimental and control groups. Demographic data of both groups are shown in Table 1.
p<0.05.
NRS pain measurement
In the pretest, comparisons of the levels of NRS pain measurement indicated that there was no statistically significant difference between the two groups. For the post-test, the levels of NRS scores showed a significant difference between both groups (p<0.05). Furthermore, a significant difference of NRS was found between pretest and post-test in the experimental group (p<0.05) but not in the control group. The results are shown in Figure 1.
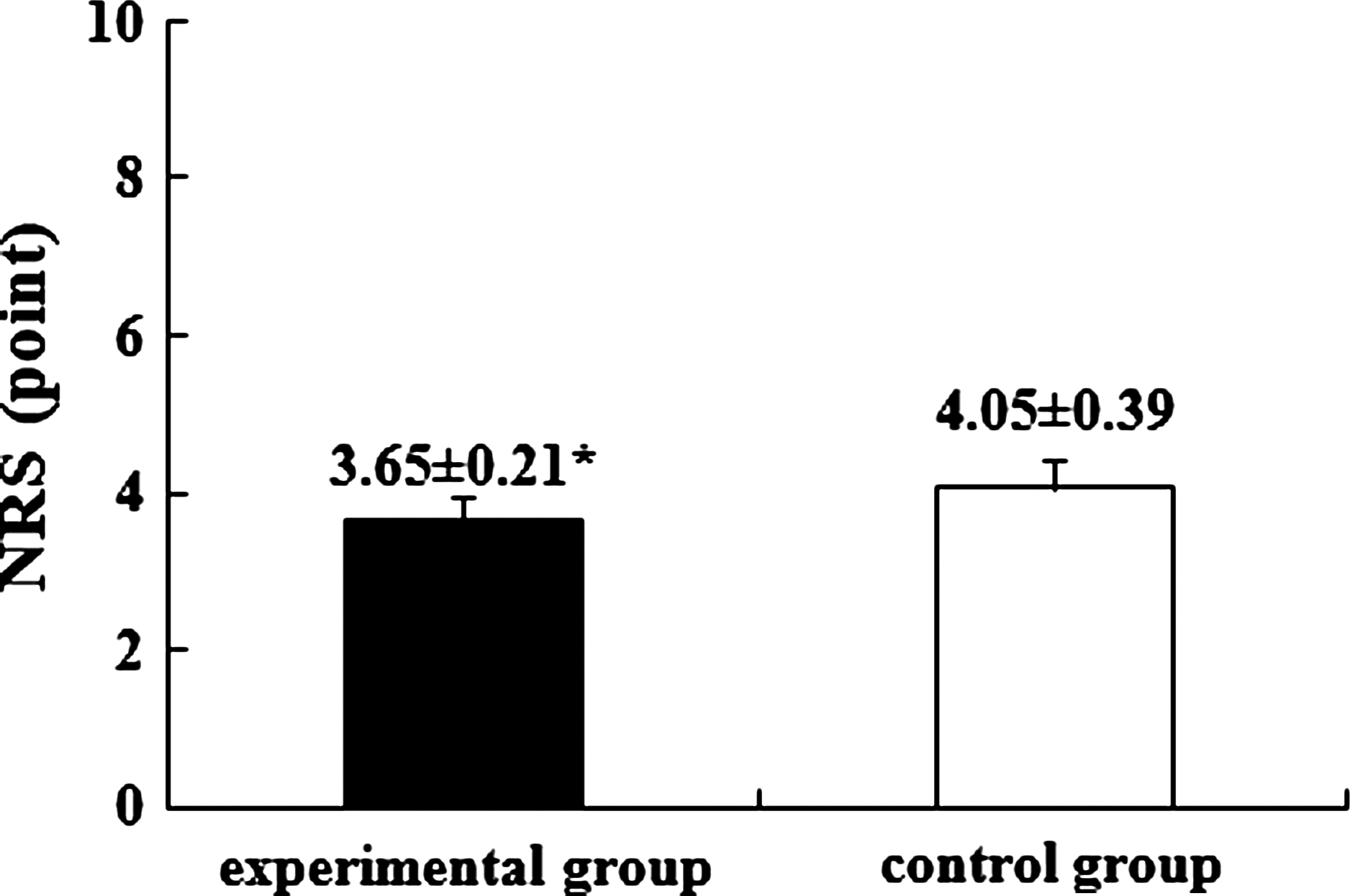
Means of numeric rating scale (NRS) levels for experimental and control groups. *p<0.05. Vertical bars indicate standard error of the means.
Comparison of IL-6 levels
There was no statistically significant difference for each comparison of levels of pretest IL-6 in both groups. The difference between both groups for each comparison of levels of post-test was statistically significant (p<0.05). Furthermore, a significant difference of IL-6 level was found between pretest and post-test in the experimental group (p<0.05), but not in the control group. The data are presented in Figure 2.
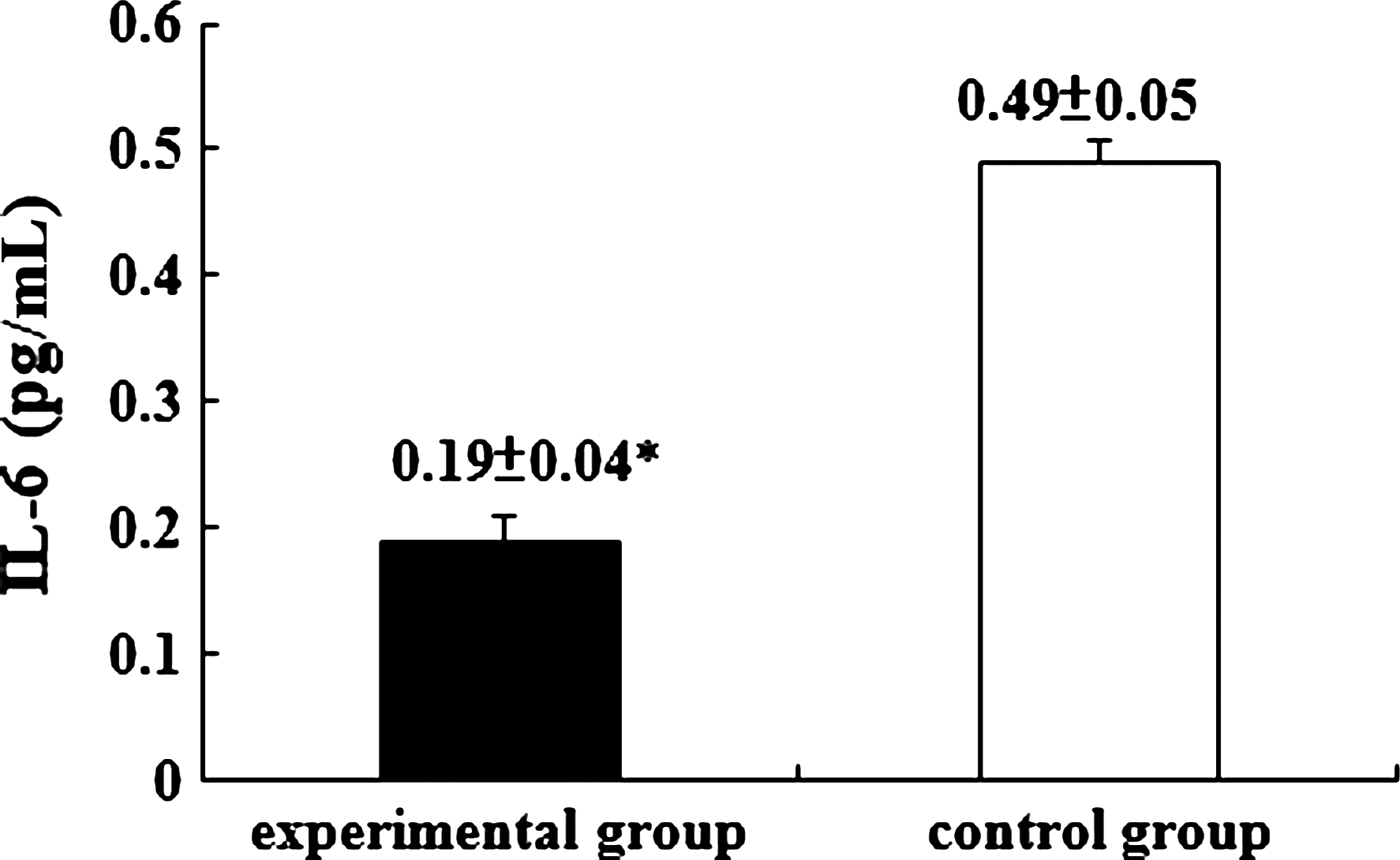
Means of serum interleukin-6 (IL-6) levels for experimental and control groups. *p<0.05. Vertical bars indicate standard error of the means.
Comparison of ET-1 levels
Similar results were also found on the levels of ET-1. A significant difference was revealed on the ET-1 level of post-test between both groups (p<0.05). The difference between the ET-1 levels of pretest and post-test in the experimental group was also found to be significant (p<0.05). The data are presented in Figure 3.
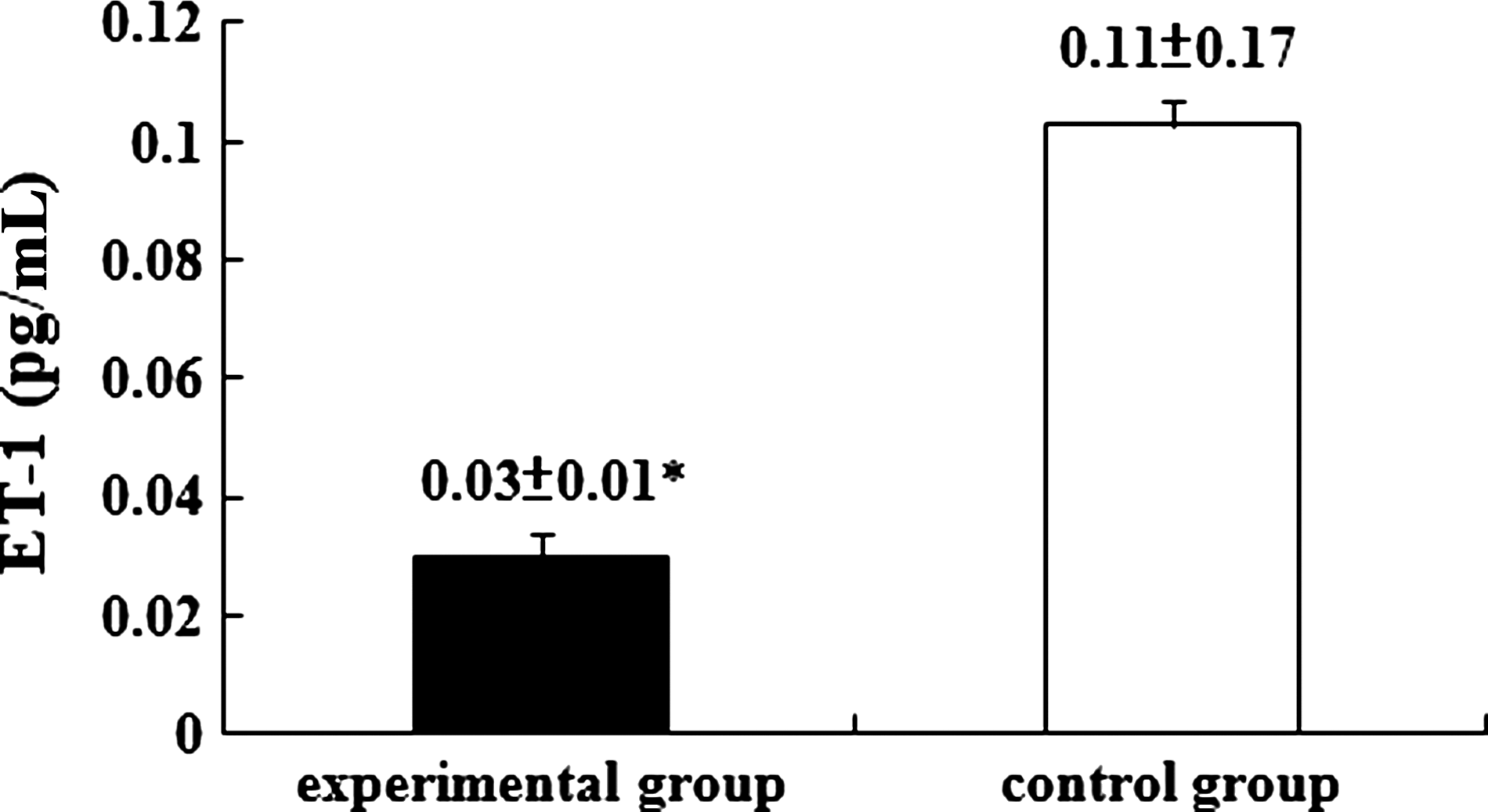
Means of serum endothelin-1 (ET-1) levels for experimental and control groups. *p<0.05. Vertical bars indicate standard error of the means.
Discussion
The main findings of the study were improvement of the clinical markers of pain and decrease of the serum biologic markers of IL-6 and ET-1 levels with the thermal therapy with FIR on the acupoints of ST37 (Shang Chu Hsu), ST38 (Tiao Kou), ST39 (Hsia Chu Hsu), and ST40 (Feng Lung). In this study, the experimental group after TKA had significantly lower NRS and serum IL-6 and ET-1 levels than the control group at post-test. They also had a greater decrease in pain, serum IL-6, and ET-1 levels, compared to the pretest and post-test of the experimental group of TKA patients.
There was no statistical significance in the demographic characteristics except in the comparison of gender (χ2=0.07, p<0.05). Both groups have a similar quality and quantity of demographic data that independent samples t-test revealed no significant difference statistically despite the unequal gender ratio. Analysis and comparison of subjects by gender are shown in Table 2. Accordingly, gender had no effect on the independent variables. More women in this study corresponded to the works of Oliveria et al. 1 and Cicuttini. 6 The sample demonstrated more female predominance (F:M=2:1) and multifactorial etiologies, with a strong family history or pattern of inheritance, growing body weight, and lowering level of estrogen during the postmenopausal period. 12,13
SD, standard deviation; NRS, numeric rating scale; IL-6, interleukin-6; ET-1, endothelin-1.
The intervention of FIR in the experimental group lowered the NRS with significant difference; however, in the control group, there was no significance. Consequently, the intervention of FIR had significant effects on the NRS group and hence improved pain relief. It corresponds to the regional exposure of FIR that causes local capillary expansion by energy transference and heat effect. Consequently, this increases nutrient supply to the tissue, accelerates tissue repair, improves waste removal, and elevates the patient's pain threshold. It eventually improves wound healing and pain relief. 8 The effect of FIR includes three biologic effects: the radiation effect, resonance effect, and thermal effect. 7 It can transfer the energy to the human body to accelerate local circulation and improve capillary flow. Then, it may increase tissue oxygenation and improve metabolism, causing elimination of chronic inflammation, pain relief, subsidence of swelling, acceleration of recovery, relief of muscle cramp, relaxation of musculotendinous structure, release of nervous condition, and eventual symptom relief. The FIR therefore can lower the pain indicator, decrease the NRS, release the painful discomfort, and then activates the physiologic function of the human body.
IL-6 is a multifunctional cytokine that regulates immune responses and acute phase reactions and may play a central role in host defense mechanisms. 14 It is also one of the chemical materials secreted by the injured tissue while the nerve ends are severed during injury. 6 IL-6 is involved in the induction of B-cell differentiation, acute phase proteins, and fever. 15 The concentration of IL-6 correlates with severity of inflammation, whereas high levels in the tissue cause local inflammation, which can be monitored clinically as an inflammatory indicator. 16 Elevated serum levels of IL-6 are found in patients with severe burns, and IL-6 is also a marker for septic shock, inflammatory arthritis, traumatic arthritis, and predicting postoperative complications. 17,18 IL-6 may increase rapidly during acute infections and is elevated in the presence of severe acute respiratory syndrome. It is the major glycoprotein induced during the acute phase of infection. 19 IL-6 is also a circulating multifunction protein produced by various tissues, including mononuclear cells, endothelial cells, and adipocytes. 20 The level of IL-6 in blood serum shows a significant difference between stress and the hypothalamic–pituitary–adrenal axis phase. 21 According to the result of this study, the average level of serum IL-6 after the intervention of FIR has lowered from 1.15 pg/mL to 0.19 pg/mL and demonstrated a significant decline and statistical difference (p<0.05). No significance was revealed in the control group. In conclusion, effective application of FIR can lower the level of IL-6 in the serum. The level correlates with not only the inflammatory marker but also the pain relief.
ET-1 is a 21–amino acid peptide originally isolated from the supernatant of cultured porcine aortic endothelial cells and is one of the most potent vasoconstrictors currently known. 22,23 The endothelin peptide family consists of three isoforms: ET-1, ET-2, and ET-3. Human ET-1 is produced primarily by endothelial cells and smooth-muscle cells, and the cells from the kidney, heart, brain, lung, pancreas, and spleen also synthesize this peptide. 24 The normal plasma level of ET-1 is very low (<1 pg/mL). However, elevated levels of ET have been detected in patients in cardiogenic shock, on chronic dialysis, and with pulmonary hypertension. Elevated levels have also been shown in case of hyponatremia, uremia, myocardial infarction, and several other medical disorders. 22,25 –27 The current study also concluded that the level of serum ET-1 lowered by 0.37 pg/mL (from 0.41 pg/mL to 0.03 pg/mL) after intervention of FIR. It also demonstrated statistical significance (p<0.05), whereas no significance was revealed in the control group. Accordingly, FIR can certainly lower the level of ET-1 and then improve the clinical manifestation of painful symptoms.
The main limitation of this study was the intervention that needed teamwork and hospital policies approved; therefore, selection of only the orthopedic ward of a medical center was needed for the study to be enrolled in research studies. Moreover, the study was based on a small sample and was exploratory in nature. Another limitation was that the period of the intervention was relatively short. In addition, future studies should consider a long-term follow-up or longitudinal studies that allow researchers to track changes at the individual level and collect data about the changes over time.
Conclusions
FIR has significant effects on both pain relief and lowering the serum levels of IL-6 and ET-1. The results may not only indicate FIR for the postoperative pain relief of TKA, but it also may be used as a guide for other clinical applications.
Footnotes
Disclosure Statement
No financial conflicts exist.